Fig. 27.1
Cerebellar atrophy related to phenytoin use. Coronal T2-weighted (a) and sagittal T1-weighted (b) MR images demonstrate disproportionate diffuse cerebellar atrophy
Another neurological effect of phenytoin is a transient focal lesion in the splenium of the corpus callosum. Splenial lesions are characteristically oval or round, measure less than 2 cm in size, and demonstrate hyperintense signal on T2-weighted sequences, hypointense signal on T1-weighted sequences, and restricted diffusion (Fig. 27.2).
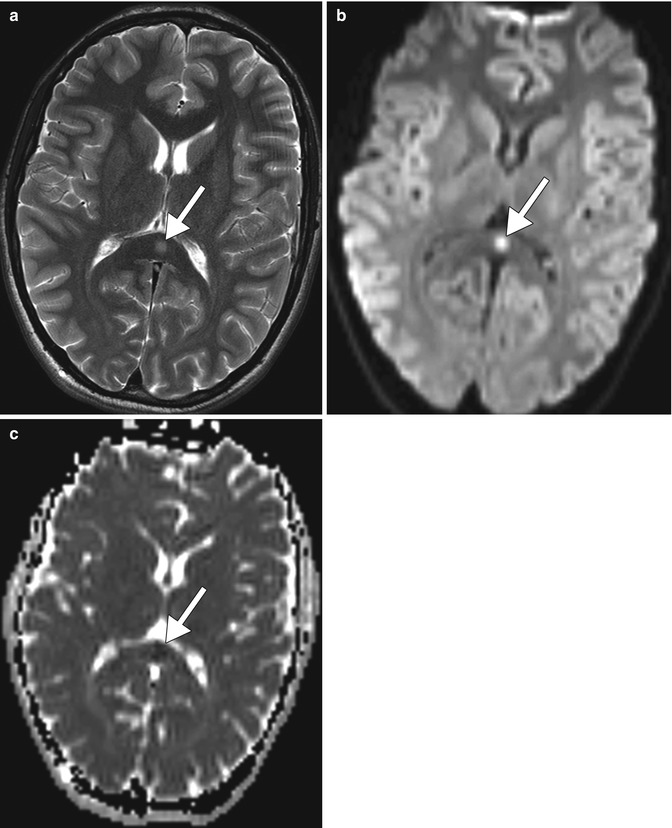
Fig. 27.2
Focal transient splenial lesion related to antiepileptic therapy. Axial T2-weighted MRI (a) demonstrates a focal hyperintense lesion in the splenium of the corpus callosum (arrow) in a patient taking phenytoin. DWI (b) and ADC maps (c) demonstrate restricted diffusion of the lesion (arrow)
Patients with chronic use of phenytoin may also present with acromegalic features with calvarial hyperostosis and coarsening of the face, hands, and feet. The incidence of calvarial thickening in epileptic patients treated with phenytoin is approximately 33 %. On imaging, progressive diffuse, smooth intramedullary expansion can be observed (Fig. 27.3).
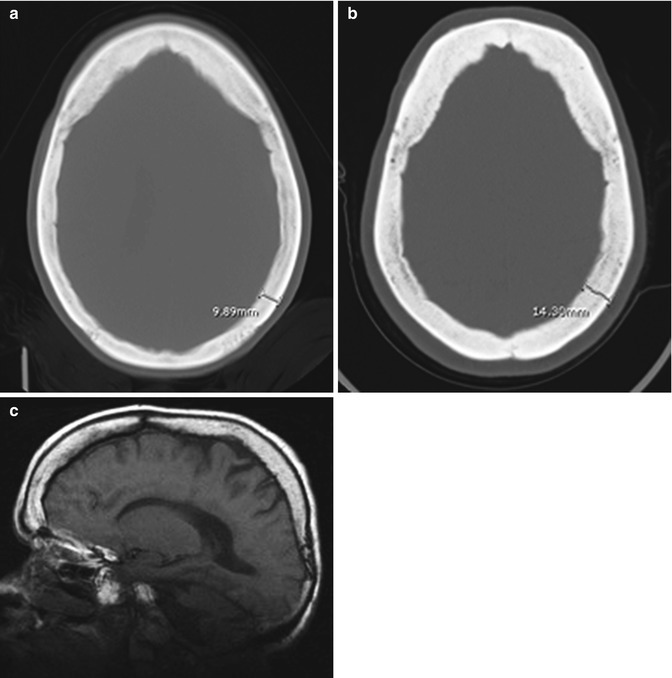
Fig. 27.3
Calvarial thickening secondary to chronic phenytoin use. Axial CT images obtained at initial presentation (a) and after over a decade of antiepileptic treatment (b) show development of substantial diffuse calvarial thickening. The sagittal T1-weighted MRI (c) also shows diffuse calvarial thickening with normal hyperintense fatty marrow signal
Fetal hydantoin syndrome is a known disorder caused by the in utero exposure of phenytoin. Patients taking phenytoin during their pregnancy have two to three times the risk of birth defects compared to the general population. Although not all exposed fetuses develop the syndrome, the risk of expressing the full syndrome is 5–10 %, while the risk of expressing isolated features is 33 %. The differences in expression are determined by maternal genetic characteristics and ability to detoxify the intermediate metabolites of phenytoin. The effect of phenytoin in the metabolism of folic acid plays a crucial role in the increased risk of spina bifida. The classic features of fetal hydantoin syndrome include a dysmorphic appearance (with craniofacial anomalies, such as hypertelorism, deep nasal bridge, small nose, and cleft lip or palate), mental retardation, growth deficiencies, and limb defects. Other features include microcephaly, ocular defects, spina bifida, and cardiovascular anomalies.
Signs and symptoms related to acute cerebellar dose-related toxicity usually reverse following discontinuation of the medication. However, other effects such as cerebellar atrophy and calvarial thickening may be permanent despite a change in anticonvulsive therapy. Nevertheless, the clinical implications of calvarial thickening are mainly cosmetic.
27.4 Differential Diagnosis
The imaging findings associated with the use of phenytoin are not specific and could be related to several conditions including other antiepileptic medications. The clinical history may be the differentiating factor for making the correct diagnosis.
Cerebellar atrophy: The differential diagnosis for cerebellar atrophy is broad, including aging, alcohol, paraneoplastic syndromes, radiation, hypothyroidism, the sequela of cerebellitis, hereditary cerebellar atrophy, and multiple system atrophy.
Alcoholic encephalopathy typically leads to disproportionate superior vermian atrophy and decrease in whole brain metabolism on F-18 FDG PET. A history of alcohol abuse is key in making the diagnosis (refer to Chap. 2).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



