♦ Preoperative
Operative Planning
- Review imaging and determine the portion of the cavernous sinus requiring exposure and how it relates to cranial nerve anatomy of the cavernous sinus
Equipment
- Major set-up
- High-speed drill with a small cutting burr
- Cranial fixation plates and screws
- Osteotome/mallet
- Mayfield head holder
Operating Room Set-up
- Headlight
- Bipolar cautery
- Loupes
- Bovie cautery
- Anticonvulsants
- Perioperative antibiotic coverage
- Dexamethasone
♦ Intraoperative
Positioning
- Mayfield headholder placed in anteroposterior position with single pin set to the contralateral side
- Head is turned 30 to 60 degrees to the contralateral side with the zygoma as the most superior point of the operative field
- Shoulder roll is placed under ipsilateral shoulder to ensure jugular venous return
- The ipsilateral thigh or abdomen is prepped and draped (should there be a need for fat graft)
Planning
- Mark skin incision as a gentle curve 1 cm anterior to the tragus and at the inferior border of the zygoma to a point just lateral to the midline on the contralateral side
- Prep and drape
Craniotomy Incision/Exposure
- Infiltrate with 0.5% lidocaine and epinephrine
- Incise the skin and begin reflecting the scalp flap
- Dissect along the temporalis fascial plane until the subgaleal fat pad is identified
- To avoid damage to the frontalis and zygomatic branches of the facial nerve, the superficial fascial layer of the temporalis is incised and reflected anteriorly with the fat pad
- The fascia becomes continuous with the periosteum of the lateral orbit and zygoma at this point and is therefore bluntly dissected from the bone with the aid of a small periosteal elevator or Adson dissector
- Proceed with craniotomy of the pterional region (Fig. 7.1A) with or without orbitozygomatic or transzygomatic modification as described in prior chapters
- Place dural tacking sutures and obtain epidural hemostasis
- Bone edges are waxed for hemostasis
♦ Extradural Osteotomy (Fig. 7.1B)
- Flatten the sphenoid wing with a drill or a Kerrison rongeur
- The region of the meningo-orbital artery near the apex of the superior orbital fissure is identified and the artery is cauterized and cut
< div class='tao-gold-member'>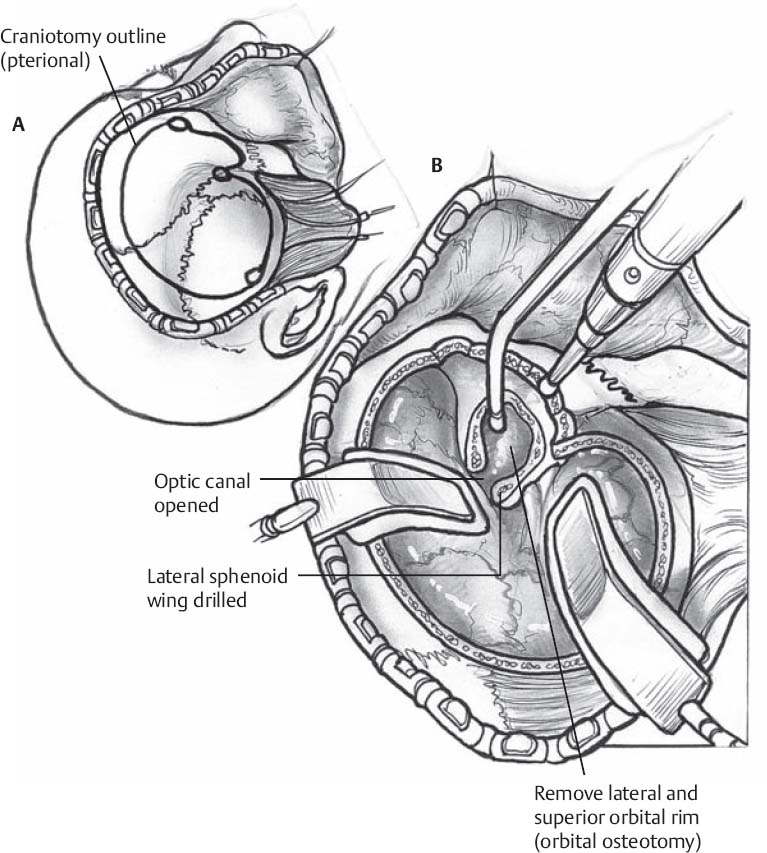
Fig. 7.1(A) The Dolenc approach begins with a pterional craniotomy. (B) Extradural drilling of the optic strut and anterior clinoid process.
Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel






Full access? Get Clinical Tree


