♦ Preoperative
Imaging
- Magnetic resonance imaging (level of nerve root involvement)
- Computed tomography
- Bone scan
- Metastatic work-up
Biopsy
- For diagnosis
- Plan extent of resection
- Plan biopsy tract to be included and excised in definitive surgery
- Patient counseling
- Postoperative deficits: bowel/bladder incontinence, sexual dysfunction, neurologic deficits
Bowel Preparation
- Neomycin/erythromycin and polyethylene glycol electrolyte solution by mouth
Equipment
- Basic spine tray
- High-speed drill
- Osteotomes
- Cell saver
- Andrews table
Operating Room Set-up
- Headlight
- Loupes
- Bipolar and Bovie cautery
- Fluoroscopy (if instrumentation needed)
Anesthetic Issues
- Prepare for large blood loss (3 to 10 liters)
- Large bore intravenous access
- Central line or Swan-Ganz monitoring if necessary
- Foley cather
- Consider steroids if neural manipulation is likely
♦ Intraoperative (Fig. 140.1)
Positioning
- Patient prone with face and eyes padded; Andrews frame is helpful
- Lateral position for combined abdominosacral approach
Sterile Scrub and Prep
- Include large volume intraoperative enema
Incision
- Midline for small, distal tumors in nonirradiated tissue
- Omega flap is needed for larger, proximal resection
< div class='tao-gold-member'>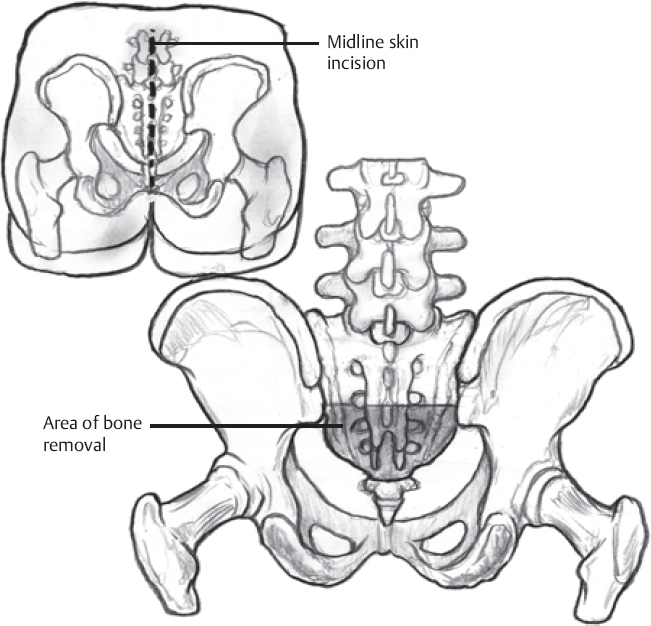 Only gold members can continue reading. Log In or Register to continue
Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel






Full access? Get Clinical Tree


