26 Dural Sinus Management In skull base surgery, and especially in the posterior skull base approaches, it is of paramount importance to manage the dural sinuses, bridging veins (e.g., tentorial, petrosal), and the vein of Labbé. Whenever possible, aim to preserve the sinuses and bridging veins, as occlusion may lead to a number of often unpredictable events, despite the use of pre- and intraoperative tests. A meningioma with a dominant sinus invasion may be best managed by subtotal-partial resection followed by radiotherapy of the intrasinus component; in rare situations and in expert hands, a total resection with venous reconstruction may be achievable. • Preoperative magnetic resonance imaging (MRI), magnetic resonance venography (MRV), computed tomography venography (CTV), or cerebral angiogram are used to determine the involvement of the dural sinuses in the different pathologies (e.g., meningioma invasion of the sinus vs. compression of the wall), as well as the different anatomic variations of size and dominancy of the sinuses and the collateral drainage of the occluded sinuses. • Preservation of the sinuses/veins is the main goal of surgery. Their reconstruction or their sacrifice are dependent on the existence of outflow collaterals, in order to avoid brain/cerebellum venous infarct and/or swelling. Anatomic variations of the dural sinuses, vein of Labbé, and bridging veins should be studied in detail before deciding on the appropriate treatment (e.g., surgery vs. radiosurgery) and on the appropriate lateral approaches to the middle and posterior skull base (e.g., subtemporal/transpetrous approaches). Fig. 26.1 portrays the anatomy; also see page 33. • In type 1 invasion (see Fig. 26.2), the lateral wall of the tumor may be peeled away, whereas reconstructive or nonreconstructive techniques have to be used for the other types. • In general, occlusion of one cavernous sinus, superior petrosal sinuses, and nondominant transverse and sigmoid sinuses is well tolerated by patients. Occlusion of the anterior third of the superior sagittal sinus is generally tolerated when the anterior cortical veins have collaterals; otherwise, there is still the risk of frontal lobe venous infarction/edema. • Occlusion of a nondominant transverse sinus or a patent contralateral sinus is generally well tolerated by patients, but pseudotumor cerebri can develop, with subsequent headache and other symptoms related to raised intracranial pressure. There can be neuro-ophthalmological complications as well.2 • Iatrogenic cavernous sinus occlusion done intentionally by the skull base surgeon is usually well tolerated as long as the sinus is not overpacked. Over-packing can lead to cranial neuropathy, or internal carotid artery (or its branches) compression or occlusion. • There is uncontrolled evidence to support the use of intraoperative test occlusion. Sinus Invasion Classification System1 (Fig. 26.2) Type 1: attachment to the outer layer of the sinus wall Type 2: tumor fragment inside the lateral recess Type 3: invasion of the lateral wall Type 4: invasion of the lateral wall and roof Type 5: complete sinus occlusion Type 6: complete sinus occlusion with invasion of the contralateral wall
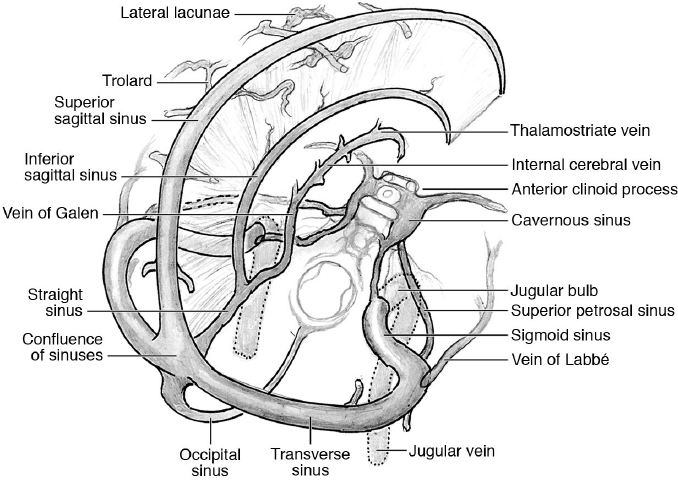
 Anatomy of the Dural Sinuses and Vein of Labbé
Anatomy of the Dural Sinuses and Vein of Labbé
 Intraoperative occlusion test3–5:
Intraoperative occlusion test3–5:
 Insert a 20-gauge butterfly needle into the sinus for measuring the venous pressure (normally < 15 mmHg, but it is related to the position of the head).
Insert a 20-gauge butterfly needle into the sinus for measuring the venous pressure (normally < 15 mmHg, but it is related to the position of the head).
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


