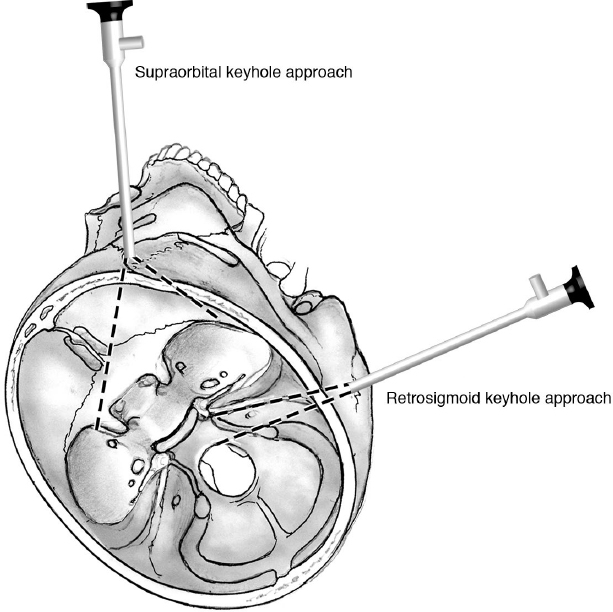
17 Endoscopic Keyhole Approaches Advances in anatomic knowledge, neuroradiological imaging, and endoscopic technology have evolved toward less invasive and less traumatizing surgical corridors to approach target lesions, as in the keyhole concept of minimally invasive neurosurgery.1 Endoscopy plays an important role in the keyhole concept, thanks to its main advantages: (1) superb illumination; (2) high magnification; (3) panoramic view; and (4) the ability to “look around corners,” even in deep surgical fields. Endoscopic neurosurgery is when the endoscope is used solely as an optical device. All procedures are performed under endoscopic view. Endoscope-assisted microneurosurgery combines microscopic/endoscopic techniques.2 The surgery is done with both techniques of visualization, with certain tasks assigned to certain stages of the procedure. Smaller incision, minimal brain exposure and retraction, and reduced blood loss with lower morbidity and mortality. Two-dimensional images (compensated by the advent of three-dimensional [3D] endoscopes); limitation of instrumentation; and learning curve for endoscopy. Pearl It is important to recognize that surgery involves more than just visualization. The principles of tumor access and resection as well as reconstruction remain the same as in more extensive openings. Because of the narrow corridor through the keyhole and coaxial manipulation under a straight or angled endoscope, intraoperative use of conventional micro-instruments becomes limited. Use of single-shaft instruments (e.g., scissors, grasping and coagulating forceps, and clip appliers) is mandatory.1 Endoscopy may help make the approach minimally invasive, but the surgery itself should also be minimally traumatizing.3 The supraorbital keyhole approach is one of the most frequently used keyhole variants, and has been safely applied for accessing skull base neoplastic and/or vascular lesions (Fig. 17.1). The supraorbital keyhole approach provides a less invasive alternative to more extensive skull base approaches such as coronal, pterional, and orbitozygomatic craniotomies.1,4,5 Table 17.1 Indications for the Endoscopic Supraorbital Keyhole Approach
 Keyhole Surgery
Keyhole Surgery
Advantages
Disadvantages
Instruments
 Supraorbital Keyhole Approach
Supraorbital Keyhole Approach
Meningioma (olfactory groove, tuberculum sellae, planum sphenoidale, anterior clinoid process) |
Pituitary adenoma with suprasellar and lateral extension |
Craniopharyngioma |
Intra-axial tumor (glioma, metastatic brain tumor) |
Anterior circulation aneurysms |
Advanced indication: Pathology at the medial temporal lobe in the middle skull base and around the upper brainstem in the posterior skull base |
Indications
Indications for the supraorbital approach include most tumors of the anterior skull base and aneurysms of the anterior circulation1,4–10 (Table 17.1).
Supraorbital Keyhole Craniotomy
• The patient is placed in the supine position, and the head is rotated 0 to 60 degrees to the contralateral side. The degree of rotation is dictated by the location of the target area (Fig. 17.2).
 Make the skin incision within the eyebrow, laterally to the supraorbital notch.
Make the skin incision within the eyebrow, laterally to the supraorbital notch.
 Retract the skin flap and incise the pericranium superiorly to the orbicularis oculi muscle. Strip the temporalis muscle laterally from the superior temporal line.
Retract the skin flap and incise the pericranium superiorly to the orbicularis oculi muscle. Strip the temporalis muscle laterally from the superior temporal line.
 Make a bur hole laterally to the superior temporal line at the level of the anterior skull base.
Make a bur hole laterally to the superior temporal line at the level of the anterior skull base.
 By means of the craniotome, make a straight-line cut from the bur hole parallel to the orbital rim, and then connect a C-shaped line from the bur hole to the medial edge of the previously made straight line.
By means of the craniotome, make a straight-line cut from the bur hole parallel to the orbital rim, and then connect a C-shaped line from the bur hole to the medial edge of the previously made straight line.
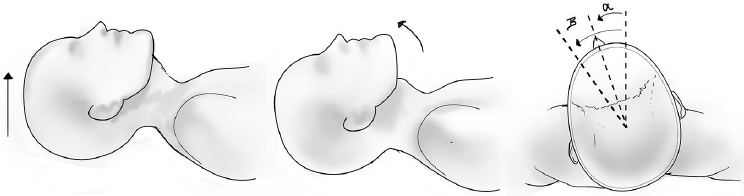
Fig. 17.2 Supraorbital keyhole craniotomy, and positioning of the head. Note the potentially different required angles, according to the surgical target.
• The supraorbital craniotomy is performed with a width of approximately 2.5 cm and a height of 1.5 cm.
 Drill the inner bony edge of the craniotomy off in order to facilitate visualization, access, and free manipulation of the instruments.
Drill the inner bony edge of the craniotomy off in order to facilitate visualization, access, and free manipulation of the instruments.
 Incise the dura mater in a curved fashion and reflect it toward the skull base.1,4,9
Incise the dura mater in a curved fashion and reflect it toward the skull base.1,4,9
 Introduce the endoscope into the surgical field.
Introduce the endoscope into the surgical field.
Medial Variation of the Supraorbital Craniotomy
The paramedian supraorbital craniotomy is placed to obtain simultaneous exposure of the suprasellar and interhemispheric structures, although supraorbital neurovascular structures and opening of the frontal paranasal sinus are unavoidable in some cases.1

 Make an eyebrow incision with medial extension to the glabellar region.
Make an eyebrow incision with medial extension to the glabellar region.

 Retract the skin flap and incise the pericranium superiorly to the orbicularis oculi muscle, and then retract frontally to expose the frontal bone.
Retract the skin flap and incise the pericranium superiorly to the orbicularis oculi muscle, and then retract frontally to expose the frontal bone.

 Make a bur hole frontally in the paramedian plane.
Make a bur hole frontally in the paramedian plane.

 Using the craniotome, make a curved-line cut from the bur hole forming the medial and basal edges, and then connect another curved line defining the frontal and lateral edges from the bur hole to the lateral edge of the previously made basal line.
Using the craniotome, make a curved-line cut from the bur hole forming the medial and basal edges, and then connect another curved line defining the frontal and lateral edges from the bur hole to the lateral edge of the previously made basal line.
• Medial variation of the supraorbital craniotomy is performed with a width of approximately 2.5 cm and a height of 2.0 cm.

 Drill the inner bony edge of the craniotomy off to facilitate visualization, access, and free manipulation of the instruments.
Drill the inner bony edge of the craniotomy off to facilitate visualization, access, and free manipulation of the instruments.

 Incise the dura mater in a curved fashion and reflect it toward the skull base.
Incise the dura mater in a curved fashion and reflect it toward the skull base.

 Introduce the endoscope into the surgical field.
Introduce the endoscope into the surgical field.
Application of the Endoscope
• Tumors and normal structures located around and behind the tuberculum sellae, sella turcica, optic apparatus, internal carotid artery, sphenoid ridge, and olfactory glove are well visualized by endoscopy.4,5
• In vascular neurosurgery, effective exclusion of the aneurysm and preservation of the parent artery and perforators, which cannot be visualized by microscope, are ensured by angled endoscopes in endoscope-assisted microscope surgery.1,9
• The endoscopic intracisternal navigation requires splitting of the arachnoid according to the same techniques and principles used in microneurosurgery.
 Endoscopic Anterior Skull Base Reconstruction via a Supraorbital Keyhole
Endoscopic Anterior Skull Base Reconstruction via a Supraorbital Keyhole
Dural defects resulting from surgical intervention must be reconstructed. A pedicled pericranial flap harvested endoscopically is an alternative option for reconstruction of the anterior skull base via a supraorbital keyhole.11 The pedicled flap receives blood supply from the supraorbital artery.
 Make an eyebrow incision and dissect to the subperiosteal plane.
Make an eyebrow incision and dissect to the subperiosteal plane.
 Make two incisions around the coronal line and proceed with the endoscopic subgaleal dissection.
Make two incisions around the coronal line and proceed with the endoscopic subgaleal dissection.
 Dissect down to the orbital rim. Connect this plane to the subperiosteal plane of the eyebrow incision. Identify vessels and protect a 3-cm pedicle.
Dissect down to the orbital rim. Connect this plane to the subperiosteal plane of the eyebrow incision. Identify vessels and protect a 3-cm pedicle.
 Incise the pericranial flap from the frontal bone and elevate in the subperiosteal plane.
Incise the pericranial flap from the frontal bone and elevate in the subperiosteal plane.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


