Chapter 24 Endoscopy-Assisted Thoracic Microdiscectomy
Historically, spinal surgeons have sought to find a surgical procedure of choice to treat thoracic disc herniations [1–14]. The threat of spinal cord, neural, vascular, and pulmonary injuries has stimulated many attempted approaches, including posterior laminectomy (seldom performed because it is too likely to result in neurologic injury), costotransversectomy, transthoracic, transpleural, posterolateral, transfacet pedicle-sparing, transpedicular, and, more recently, transthoracic endoscopic and posterolateral endoscopic procedures [4,5,11–17].
Many clever, minimally invasive surgical endoscopic thoracic procedures, including video-assisted thoracic surgery (VATS) [1,2,4,5] and thoracic sympathectomy, have been developed in an attempt to reduce operative trauma. Endoscopy-assisted thoracic discectomy (EATD) (i.e., posterolateral endoscopic thoracic discectomy) is an alternative procedure for treating symptomatic herniated thoracic discs through an endoscope to cause less tissue trauma than current conventional thoracic disc surgery and thoracoscopic procedures [5,11–21]. In laser thermodiscoplasty, tissue modulation technology of a lower-energy non-ablative laser is applied for shrinkage and tightening of the disc [5,10–15,18].
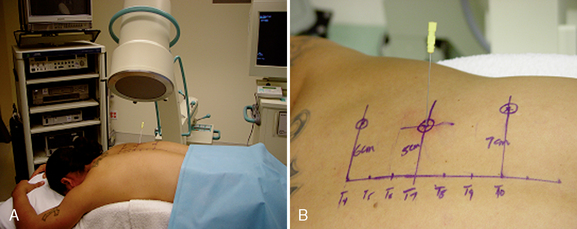
A significant number of patients with thoracic disc herniations complain of intractable thoracic spinal and paraspinal pain, intercostal or chest wall pain, upper abdominal pain, and, occasionally, low back pain due to thoracic disc protrusions without severe neurologic deficit. With improved diagnostic methods such as magnetic resonance imaging (the method of choice), computed tomography myelograms, and computed tomography scans, the diagnosis of these thoracic disc herniations or protrusions is now far more common [5,11–15]. Usually, patients with such conditions undergo some period of physical therapy, injection therapy, and analgesics, but if these treatments are not effective, the patients are often expected to live with their discomfort because of the fear of the potentially severe postoperative complications associated with surgical treatment [5,11–15].
Treatment objective of endoscopy-assisted thoracic discectomy
 The objective of EATD is the microdecompressive endoscopy-assisted thoracic discectomy of herniated thoracic disc and foraminal disc herniation. It is a minimally invasive, outpatient procedure with minimal tissue trauma and much less morbidity than open thoracic spinal surgery. There is no bone graft or fusion hardware to cause secondary problems, and the is procedure is associated with significantly lower associated convalescence periods and costs. Also, multiple thoracic discs may be treated at one sitting [5,11–15,19–21].
The objective of EATD is the microdecompressive endoscopy-assisted thoracic discectomy of herniated thoracic disc and foraminal disc herniation. It is a minimally invasive, outpatient procedure with minimal tissue trauma and much less morbidity than open thoracic spinal surgery. There is no bone graft or fusion hardware to cause secondary problems, and the is procedure is associated with significantly lower associated convalescence periods and costs. Also, multiple thoracic discs may be treated at one sitting [5,11–15,19–21].Indications
The indications for EATD are as follows [5,11–16]:
 Pain along the thoracic spine, often radiating to the chest wall, with possible numbness and paresthesia in an intercostal distribution related to thoracic disc herniation.
Pain along the thoracic spine, often radiating to the chest wall, with possible numbness and paresthesia in an intercostal distribution related to thoracic disc herniation.


Contraindications
EATD is contraindicated by the following findings or conditions [5,11–16]:
 Demonstration of severe cord compression or total block on radiographic studies secondary to severe thoracic disc extrusions that cause cord compression with severe neurologic deficit (paraparesis).
Demonstration of severe cord compression or total block on radiographic studies secondary to severe thoracic disc extrusions that cause cord compression with severe neurologic deficit (paraparesis).


















Instrumentation
The following instruments and equipment are needed for EATD:


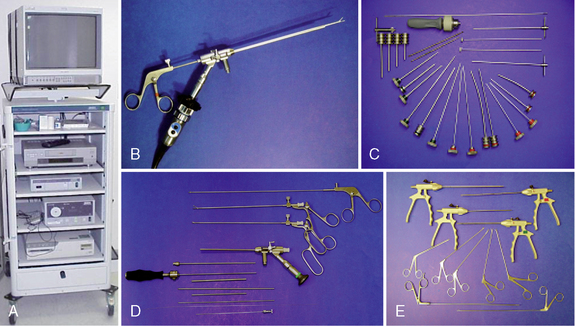
 Endoscopic tower equipped with digital video monitor, DVD recorder, light source, and photo printer, with tri-chip digital camera system (Karl Storz, Tuttlingen, Germany) (Fig. 24-2)
Endoscopic tower equipped with digital video monitor, DVD recorder, light source, and photo printer, with tri-chip digital camera system (Karl Storz, Tuttlingen, Germany) (Fig. 24-2)





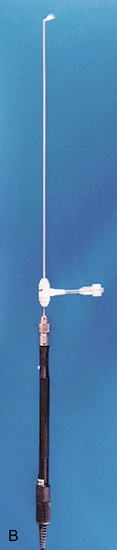
 Holmium:yttrium-aluminum-garnet (Ho:YAG) laser generator (Trimedyne, Inc., Irvine, CA) with and 550-μm holmium bare fiber with flat-tip right-angle (side-firing) probe (Fig. 24-3)
Holmium:yttrium-aluminum-garnet (Ho:YAG) laser generator (Trimedyne, Inc., Irvine, CA) with and 550-μm holmium bare fiber with flat-tip right-angle (side-firing) probe (Fig. 24-3)