Chapter 3 Epidural Malignant Tumors
LYMPHOMA
EPIDEMIOLOGY
• Primary central nervous system lymphomas in immunocompetent individuals occur slightly more commonly in males than females with a peak incidence in the six and seventh decades of life.1
DISTRIBUTION
There are no reported segmental differences in the occurrence of lymphomas in the spine.
HISTOLOGY/GRADING
• The vast majority of primary central nervous system lymphomas are diffuse, large B-cell lymphomas; although rare, primary T-cell and Hodgkin’s lymphomas have been reported.1
• The spine is a potential site of involvement by the full spectrum of lymphomas described exhaustively elsewhere.
• The diagnosis rests with the identification of a clonal population through the use of immunohistochemical staining or flow cytometric analysis (Figs. 3-1 and 3-2).
RADIOLOGY
• Lymphoma can show osseous involvement, epidural mass with or without vertebral involvement, leptomeningitic mass, and intramedullary lesions.
OSTEOSARCOMA
EPIDEMIOLOGY
• In the largest series of primary vertebral osteosarcomas reported,2 the median age of the 198 patients was 34 years, and there were slightly more females than males.
HISTOLOGY/GRADING
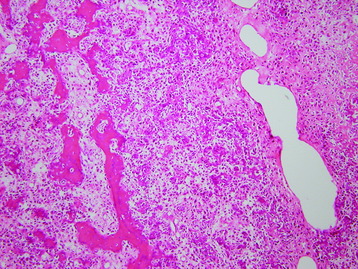
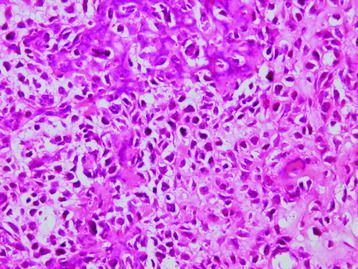
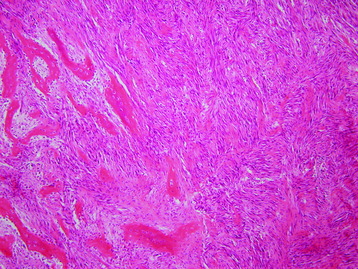
• Osteosarcomas are high-grade spindle cell neoplasms that form osteoid (Fig. 3-6) and often have associated giant cells.
• Conventional osteosarcomas are subtyped based on the nature of the matrix (e.g., osteoblastic, fibroblastic, chondroblastic) (Figs. 3-7 and 3-8).
RADIOLOGY
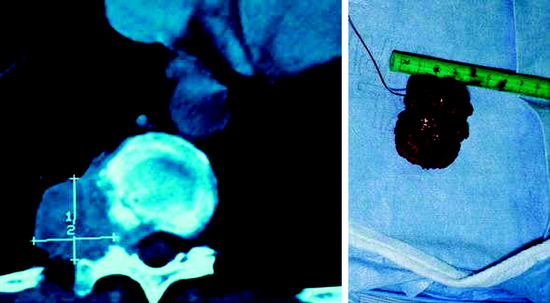
• They show cortical destruction and soft tissue mass formation. Bone matrix produced by the malignant cells can be seen on simple radiographs in most cases (Fig. 3-9).
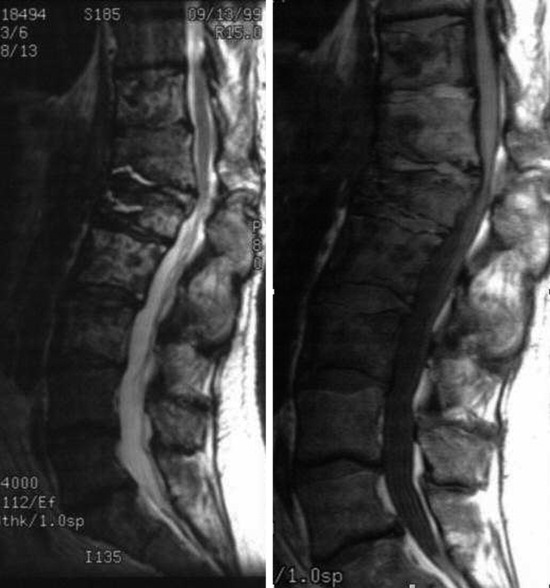
• For MR findings, the mineralized portion of the tumor mass is seen as low signal on T1WI and T2WI. Soft portion of the tumor mass is seen as low signal on T1WI and high on T2WI (Fig. 3-10). With contrast, the mass shows a moderate enhancement pattern.


EWING SARCOMA
EPIDEMIOLOGY
• Primary vertebral Ewing sarcoma is unusual and accounts for slightly less than 10% of all cases of this neoplasm.
• In the largest published series of primary vertebral Ewing sarcoma,3 the average patient age was 19 years and there was a definite male predominance (62%).
DISTRIBUTION
• More than one-half of all cases of primary vertebral Ewing sarcoma in the series just described arose in the sacrum. Another one-quarter of the cases were located in the lumbar segment, with approximately 10% in the thoracic region. The cervical segment was very rarely involved.
HISTOLOGY/GRADING
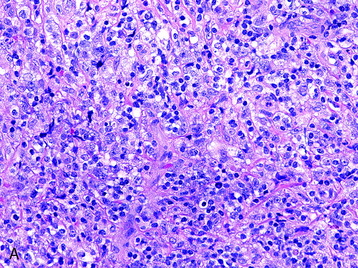
• Ewing sarcoma is one of the “small round blue cell” tumors (Fig. 3-11). The histologic differential is broad, but can usually be clarified through the use of immunohistochemical stains. This differential diagnosis includes, but is not limited to:
• Metastatic lesions (particularly neuroblastoma in the pediatric age group and small cell carcinomas in adults)
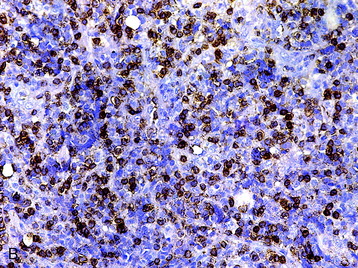
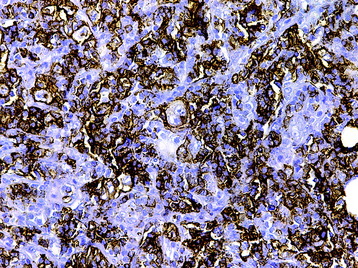
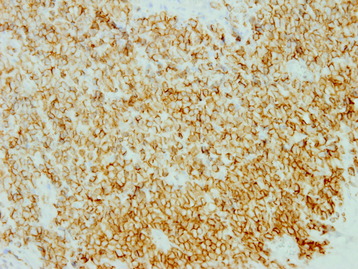
• Ewing sarcoma demonstrates a honeycomb pattern of membranous CD99 immunoreactivity (Fig. 3-12). Definite diagnosis, however, requires cytogenetic or molecular genetic studies for the +(11; 22)(q24; q12) translocation, which is found in more than 95% of cases.5
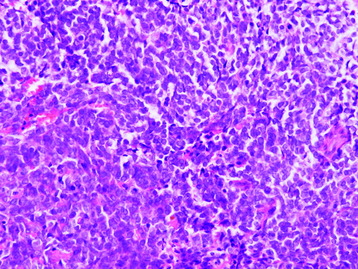
Fig. 3-11 Uniform round cells with uniform round nuclei and scanty cytoplasm (hematoxylin–eosin stain, ×400).
RADIOLOGY
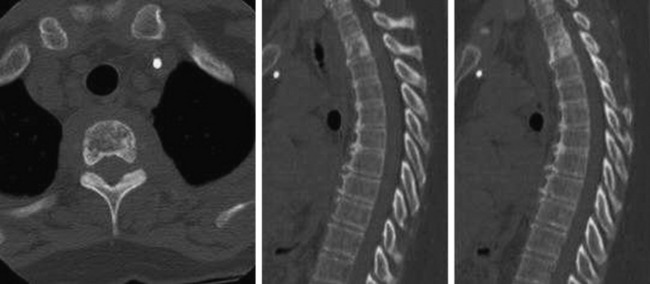
• This tumor shows a moth-eaten bone destruction pattern. It usually starts from the vertebral body or sacrum.
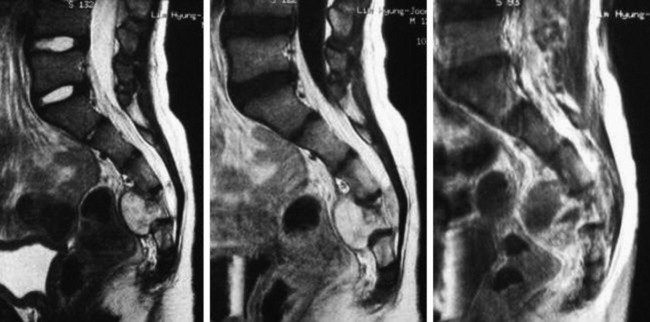
• The vertebral body destruction pattern is not extensive, so tiny perforation of the bony cortex is more common rather than wide loss of the cortical bone. Extraosseous soft tissue mass is often accompanied with the vertebral body mass (Fig. 3-13).
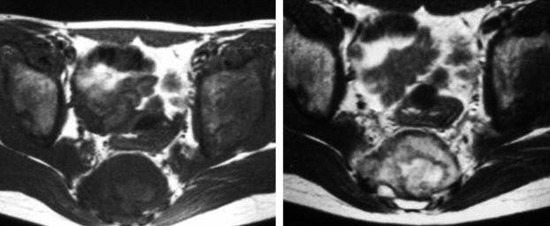
• The signal change in magnetic resonance imaging (MRI) is variable. On T1WI, the signal is intermediate to low, and on T2WI an intermediate to high signal change is a usual finding (Fig. 3-14). A moderate enhancement pattern is common. A necrotic area is commonly seen in the tumor mass.
CHONDROSARCOMA
EPIDEMIOLOGY
• Primary chondrosarcomas of the mobile spine are rare lesions. Two reviews6,7 document 22 and 21 patients for the two institutions (Istituto Rizzoli and University of Texas M. D. Anderson Cancer Center) in 59 and 43 years, respectively.
HISTOLOGY/GRADING
• Grade I chondrosarcomas are mild to moderately cellular neoplasms composed of neoplastic chondrocytes within lacunae in a chondroid matrix (Fig. 3-15).
• With increasing grade, there is greater nuclear atypia and cellularity and often necrosis. If there is a coexistent spindled morphologic pattern, a diagnosis of another more highly malignant tumor (e.g., dedifferentiated chondrosarcoma) is likely.2
• The histologic differential of low-grade chondrosarcomas includes chordoma. Even though the growth patterns of these two lesions are often evident with sufficient sampling, immunohistochemical staining also can differentiate the lesions; chondrosarcomas demonstrate immunoreactivity for S100 protein (Fig. 3-16) but not keratin (Fig. 3-17), whereas chordomas are immunoreactive for both.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


