Evaluation of the cervical spine in infants, children, and adolescents poses unique challenges to the practitioner. A thorough understanding of the developmental anatomy and features of the growing spine is required to properly evaluate and treat disorders of the immature cervical spine. Disorders present in children are often congenital or developmental in nature and may be seen infrequently in adults. In addition, children (particularly those who are preverbal, nonverbal, frightened, or in pain) may be difficult to examine and unable to describe their symptoms or localize pain. Radiographic standards and techniques used to evaluate the cervical spine primarily have been described in and derived from adult studies and must be interpreted in light of the special features of the growing cervical spine. For these reasons, evaluation of the cervical spine in infant children and adolescents differs from that of adults and requires a thorough understanding of the anatomy, growth, and development of the pediatric cervical spine.
DEVELOPMENTAL ANATOMY
The developmental anatomy of the cervical spine is best understood through its embryology. By the 3rd week of gestation, the notochord is formed from mesenchymal tissue (1). Adjacent and parallel to the notochord lies the paraxial mesoderm, which eventually differentiates into segmented somites (1,2). By week 3, four cranial and eight cervical somites develop from the mesoderm (1, 2, 3 and 4). During the 4th week of gestation, these somites further differentiate into sclerotomes and myodermatomes; sclerotomes are the precursors of the spinal column (1, 2 and 3). The sclerotomes undergo a process known as resegmentation, where each somite divides into a cranial and caudal portion. The cranial half of each somite then fuses with the caudal portion of an adjacent somite, forming a prevertebra (1,2,5). Ventrally, sclerotomal cells form the vertebral bodies, disks, and costal processes. Dorsally, they form the pedicles and lamina of the vertebrae. The apical and alar ligaments of the atlantoaxial articulation as well as the nucleus pulposus of the intervertebral disks form from the notochord. Spinal growth occurs by endochondral ossification that is preceded by mesenchymal chondrification during weeks 5 and 6.
THE ATLAS
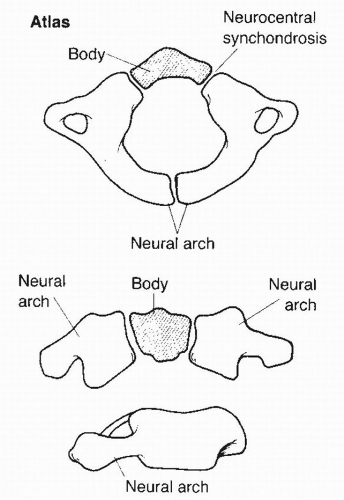
The atlas (Fig. 29.1) develops from three ossification centers: the ventral arch and the two neural arches (6,7). At birth, the two primary ossification centers comprising the neural arches are already ossified. A secondary ossification center that forms the body of the atlas is present about 20% of the time at birth and is usually visible on radiographs by 1 year of age. The neural arches fuse dorsally to each other by 3 to 4 years of age, whereas the neurocentral synchondroses that exist between the lateral masses and the body of C1 fuse by about age 7. As a result, the final internal diameter of the atlas is present by about age 7 years, whereas further growth of the external diameter of the atlas occurs during later growth through the mechanism of appositional bone deposition.
THE AXIS
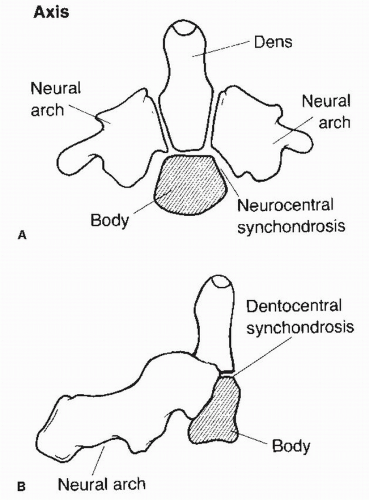
The axis (Fig. 29.2) develops from five primary ossification centers (8,9). The odontoid has two separate ossification centers, which generally fuse in the midline by the 7th month of prenatal development. Persistence of these two halves of the odontoid is known as a dens bicornis. A separate ossification center comprises the body (centrum), and two additional ossification centers form the right and left lateral masses (neural arches). Two secondary ossification centers are also present in the immature axis (8). One forms the tip of the odontoid, which appears at 3 to 6 years of age. This generally fuses with the body of the odontoid by age 12 but may occasionally persist as a separate ossification center. This is termed an ossiculum terminale and is considered a normal anatomic variant (8). The inferior apophyseal ring also contains a secondary ossification center that generally appears at puberty and fuses with the body of the axis by age 25 (8).
The neurocentral synchondrosis between the body of the axis and odontoid generally fuses between 3 and 6 years of age. A remnant of this may be radiographically visible up to age 12. This synchondrosis is positioned caudal to the level of the superior articular facets of C2 and contributes to the height of the odontoid process. Its appearance on an anteroposterior (AP) radiograph has been described as being similar to a “cork in a bottle” and may be present in 50% of children 5 years of age. Its presence can be misinterpreted as a fracture. The synchondrosis is absent in most children by 6 years of age (2,6,8). The synchondroses connecting the neural arches and the body and odontoid generally fuse at 3 to 6 years of age, whereas the synchondroses between the spinous process usually fuse by 3 years of age (8).
Figure 29.1. Diagrammatic drawings of the atlas (C1) showing bird’s eye, anterior, and lateral views. (From Copley LA, Dormans JP. Cervical spine disorders in infants and children. J Am Acad Orthop Surg 1998;6:205.)
LOWER CERVICAL VERTEBRAE (C3-C7)
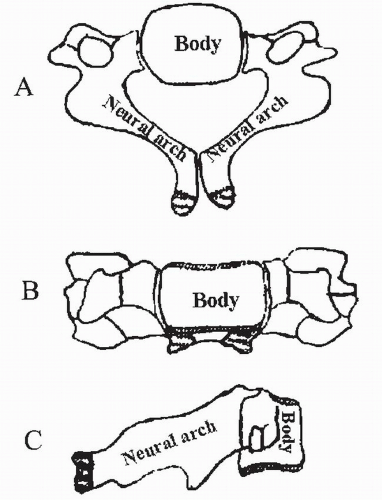
The vertebrae of the lower cervical spine (Fig. 29.3) each ossify from three ossification centers: one ossification center for the body and two for the neural arches (10). There are two secondary ossification centers present: the superior and inferior ring apophyses. These apophyses ossify during late childhood and contribute to vertebral body height and then fuse with the vertebral bodies by 25 years of age (10). The neurocentral synchondroses between the body and neural arches generally fuse between 3 and 6 years of age, while the spinous process synchondrosis located between the two neural arches generally fuse by 3 years of age (10).
Figure 29.2. Diagrammatic drawings of the axis (C2) showing (A) anterior and (B) lateral views. (From Copley LA, Dormans JP. Cervical spine disorders in infants and children. J Am Acad Orthop Surg 1998;6:205.)
THE IMMATURE CERVICAL SPINE: HOW IS THE CHILD DIFFERENT?
Anatomic and developmental factors result in many of the unique characteristics of the immature cervical spine (Fig. 29.4). These differences generally occur in children younger than 8 years of age, at which time the cervical spine approaches adult morphology and size (11). Children younger than 8 years of age have increased neck motion compared to adults for several reasons (12,13). The facet joints in the immature cervical spine are horizontally oriented and become more vertical with growth. The facet orientation from C5-C7 increases from approximately 55 to 70 degrees during growth, whereas the facets in the upper cervical spine increase vertical orientation from 30 to 70 degrees during growth (12, 13 and 14). Younger children and infants have generalized ligament laxity and weaker neck muscles compared with older children, and the head accounts for a greater proportion of body weight in young children than adults (13). Thus, for flexion and extension, the center of rotation of the cervical spine is C2C3 in children less than 8 years of age and C5-C6 in older children, adolescents, and adults (15). Incomplete ossification of the cervical spine, particularly in the subaxial region, may give the vertebral bodies a wedge-shaped appearance on plain radiographs (8,11,14). In addition, incomplete ossification accounts for differences between children and adults in radiographic measurements that are commonly used to evaluate the cervical spine.
Figure 29.3. Diagrammatic drawings of vertebrae of the lower cervical spine showing (A) bird’s eye, (B) anterior, and (C) lateral views.
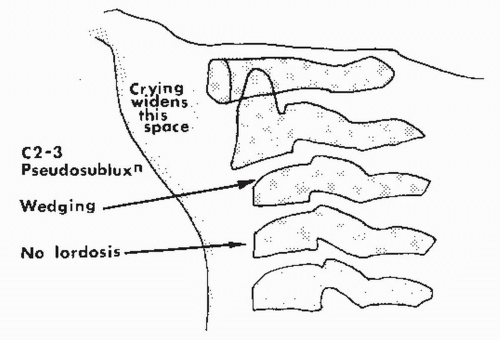
Figure 29.4. Unique features of the child’s spinal column. (From Rang M. Spine and spinal cord in children’s fractures, 2nd ed. Philadelphia: JB Lippincott, 1983.)
These unique anatomic and developmental factors allow for injuries and injury patterns in children not seen in adults. Similar to fractures elsewhere in the body, cervical spine fractures in children tend to occur through areas containing growth cartilage (15). Spinal cord injury without radiographic abnormality (SCIWORA) occurs in children because of a relative mismatch between the elasticity of the vertebral column and spinal cord (6,16, 17 and 18). In the cervical spine, the spinal column in children can be stretched as much as 2 inches before failure, whereas the spinal cord itself only tolerates about 0.25 inches of stretching before injury (17,19). Ligamentous laxity is thought to account for the high incidence of multilevel spinal injuries seen in children when compared with adults (20). The disproportionate weight of the head compared to the body mass in young children also accounts for the difference in spinal cord injury patterns seen in children younger than 8 years compared to older children. Children in the younger age group are more likely to have injuries of the third cervical vertebrae or higher and have an increased risk of death from their spinal cord injury. Children older than 8 years of age have an adult-type injury pattern, with most injuries occurring caudal to the fourth cervical vertebrae (21).
A commonly seen consequence of the increased mobility of the cervical spine in young children compared to adults or older children is the presence of physiologic cervical spine subluxation (pseudosubluxation) on lateral spine radiographs. This finding is termed pseudosubluxation when it is noted without true subluxation or pathology (Fig. 29.4) (11,14,22). This is a normal physiologic variation and does not need treatment (Table 29.1). Pseudosubluxation occurs most commonly between the second and third cervical vertebrae and between the third and fourth cervical vertebrae (11,14,22). This is seen in up to 40% of children under age 8 and may account for as much as 4 mm of anterior-posterior incongruity between the second and third cervical vertebrae with the spine in flexion (12,14). The posterior spinolaminar line of Swischuk (Fig. 29.5) can help differentiate between pseudosubluxation and true subluxation. This line is drawn along the posterior arch from the first cervical vertebrae to the third and should pass within 2 mm of the dorsal arch of the second cervical vertebrae. If this line passes more than 2 mm posterior to the ventral cortex of the dorsal arch of C2, the line is disrupted and true subluxation is present (14).
There are several unique radiographic features of the immature spine. One such feature is a lack of the normal cervical lordosis (Fig. 29.4) seen in adults. This cervical kyphosis or straightening can occur normally in up to 14% of children less than 16 years of age. In children without an injury, cervical lordosis is restored with neck extension (12). The C3 vertebral body also may be wedged (Fig. 29.4) in about 7% of young children (1,11). Computed tomography (CT) or magnetic resonance imaging (MRI) can help differentiate this normal variant from a compression fracture. Second, in children <7, the lateral masses of C1 may appear lateral to the masses of C2 on an open-mouth AP radiograph or reformatted coronal CT scan. This “pseudospread” may mimic a fracture and results from a growth differential between the atlas and the axis (15). The cervical vertebral bodies may also appear wedged, particularly C3, in children <7 years of age. However, this is a normal variant and should not be confused with a fracture. Finally, the retropharyngeal soft tissues in children may exhibit marked variability in thickness, particularly if the radiograph is taken in flexion or in expiration (15). A repeat radiograph in neutral or during inhalation should demonstrate this phenomenon.
TABLE 29.1 Cervical Spine Mobility According to Age
Total (1-16 y)
Total(1-7 y)
Age (y)
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
(n)
(%)
(n)
(%)
Anterior displacement C2-C3 (marked)
4
1
3
1
2
2
0
0
1
1
0
0
0
0
0
0
15
9
13
19
Anterior displacement C2-C3 (moderate)
1
2
1
3
2
2
4
1
1
2
3
1
1
0
0
0
24
15
15
21
Anterior displacement C2-C3 (total)
5
3
4
4
4
4
4
1
2
3
3
1
1
0
0
0
39
24
28
40
Measured AP movement, 3 mm and over
5
4
5
2
5
6
5
2
4
5
4
6
7
4
4
3
71
44
32
46
Number of children with measured AP movement over 3 mm and observed anterior displacement at C2-C3
Overriding of anterior arch of atlas relative to odontoid (extension views)b
2+
4++
3++
1
1+
3
0
1
0
0
0
0
0
0
0
0
14
9
14
20
Wide space between anterior arch of atlas and odontoid (flexion views)
2
2
3
2
2
2
1
0
0
0
0
0
0
0
0
0
14
9
14
20
Total (5-11 y)
Presence of apical odontoid epiphysis
0
0
0
0
3
2
3
1
4
1
4
0
0
0
0
0
15
9
18
26
Total (1-5 y)
Presence of basilar odontoid cartilage plate
10
9
9
6
4
0
0
0
0
0
0
0
0
0
0
0
48
30
38
76
Angulation at single level
1
4
1
1
3
3
2
0
1
2
1
2
2
1
2
0
25
16
Absent lordosis in neutral position
3
0
0
0
0
0
0
1
2
1
3
2
2
5
1
2
22
14
Absent flexion curvature C2-C7 in flexion view
1
2
1
6
4
1
0
0
2
3
1
1
1
1
2
0
26
16
a Twenty of twenty two children with anterior displacement at C3-C4 also had displacement at C2-C3. b Presence of wide atlantoodontoid space in same child (each + represents one child).
From Cattell HS, Filtzer DL. Pseudosubluxation and other normal variations in the cervical spine in children: a study of one hundred and sixty children. J Bone Joint Surg 1965;47:1295-1309.
Only gold members can continue reading. Log In or Register to continue