CHAPTER 354 Extracranial Vertebral Artery Diseases
Historical Background
As early as 1844, Quain1 described the anatomy and operative surgery of the extracranial vertebral artery in lithographic drawings. Subsequently, in 1853, Maisonneuve successfully ligated the vertebral artery at the transverse foramen of the sixth cervical vertebra for a stab wound to the neck.2 Elective ligation of the vertebral artery was also used to treat aneurysms. In 1888, Matas2 was the first surgeon who fully excised an aneurysm between the occiput and the atlas through a posterior approach. Forty years later, Moniz3 performed the first vertebral angiogram in 1927. Radner4 first reported selective angiography of the vertebral artery in 1947. The role of pathology of the extracranial vessels in relation to cerebral ischemia was emerging,5 and with this revolution in the diagnosis of diseased arteries, revascularization was being performed. In 1958, Crawford and coworkers6 presented their results of surgical treatment of brainstem ischemia by reconstructing the vertebral artery after removing atherosclerotic plaque. The next year, Cate and Scott7 first described the technique of transsubclavian endarterectomy of the subclavian-vertebral artery.
Angiography allowed visualization of other causes of extracranial vertebral artery disease, including extrinsic compression of the vertebral artery by osteophytes,8 constricting bands,9 and rotational obstruction,10 all of which were diagnosed and treated by surgical decompression. Angiography also provided the first extensive cooperative study of the incidence of extracranial arterial stenosis caused by atherosclerotic lesions in patients with cerebrovascular insufficiency. In 1968, stenosis was proposed to be a compromised lumen of more than 50% by the Joint Study of Extracranial Arterial Occlusion.11 Of 4748 patients with cerebral ischemic symptoms, 80% had four-vessel angiograms that were categorized by location of the arterial stenosis. For the first time, this study provided a frequency distribution of sites of stenosis in the extracranial vertebral artery,11 identifying at least some degree of stenosis in 22% and 18% of left and right proximal vertebral arteries, respectively, and 5% to 6% of the distal extracranial vertebral.
Clinical Presentation
The external vertebral arteries provide blood flow to a large distribution through the basilar artery and posterior cerebral arteries. Therefore, symptoms can arise from the occipital or temporal lobes, cerebellum, pons, and brainstem with its cranial nerves, a syndrome referred to as vertebrobasilar insufficiency (VBI) and characterized by intermittent episodes of multiple symptoms that can be sudden or severe (Table 354-1). Eventually, the symptoms either resolve or become permanent. These symptoms are caused not only by embolic or thrombotic sources but also by hemodynamic mechanisms. Changes in the blood flow of the vertebral artery can account for symptoms of VBI,12 even those created in some instances by head turning.13
TABLE 354-1 Symptoms of Vertebrobasilar Insufficiency
| The presence of at least two of these symptoms is required to diagnose vertebrobasilar insufficiency: |
In a review of the literature, Ausman and coworkers14 concluded that the symptoms of VBI have multiple causes and that one can seldom localize pathologic lesions in the posterior circulation by clinical examination alone. Most physicians use the presence of any two of the common symptoms to define the syndrome. The most common symptom that physicians have difficulty relating to VBI is vertigo or dizziness, which is often associated with other diseases; many articles have ruled out the occurrence of isolated vertigo or dizziness as evidence of transient ischemic attack (TIA). In general, vertigo or dizziness alone is not considered a presenting symptom of VBI,15 although some authors still assert that these could be exclusive symptoms of VBI.16,17
Anatomy of the Extracranial Vertebral Artery
The vertebral artery varies in diameter from 0.5 to 5.5 mm. The left vertebral artery is larger than the right in about 75% of cases.18 The vertebral artery flow in normal volunteers, as measured by quantitative magnetic resonance angiography (QMRA), ranges from 7 to 199 mL per minute (mean, 90 ± 32 mL per minute; median, 88 mL per minute) on the right, and 21 to 245 mL per minute (mean, 99 ± 40 mL per minute; median, 100 mL per minute) on the left.19
The extracranial vertebral arteries can be divided into three segments—the first (V1), second (V2) and third (V3), which can alternatively be termed the proximal, middle (intraosseous), and distal segments (Fig. 354-1). The designation is helpful because the associated pathology can differ among the segments.
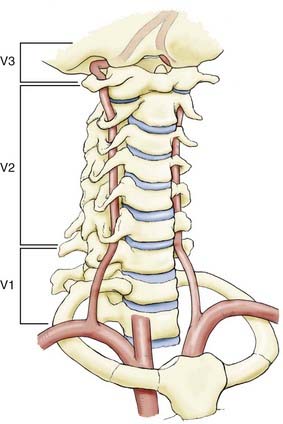
First Vertebral Artery Segment (V1)
The V1 extends from the superior portion of the subclavian artery to enter the transverse foramen of C6. It enters at levels other than C6 10% of the time (C5, 7%; C6, 90%; C7, 3%). Instead of arising from the superior portion of the left subclavian artery, the left vertebral artery can arise from the proximal subclavian trunk. In 5% of cases, it arises separately from the aortic arch. Typically, the right vertebral artery is the first branch of the right subclavian artery, but it can arise from various places: the right common carotid artery (CCA), the right internal carotid artery (ICA), the aortic arch directly, or the right subclavian artery distal to the thyrocervical trunk.20
Pathophysiology of Extracranial Vertebral Artery Disease
Regional hypoperfusion is the predominant stroke mechanism for patients with posterior circulation ischemia. Large or small vessel occlusive disease occurs more commonly in the posterior circulation than thromboembolism.21,22 Stroke secondary to vertebral stenosis can be hemodynamic in the setting of anatomic variations in the other artery, such as a hypoplastic vertebral artery, termination of one artery into the posterior inferior cerebellar artery, or complete occlusion of the contralateral vertebral.20 There also may be associated pathology in the carotid system or an incomplete circle of Willis,18 which affects the collateral circulation. Hemodynamic changes can also result systemically from cardiac insufficiency or postural hypotension.
Atherosclerosis
Atherosclerosis is the most common form of vertebral artery disease. Although it is a potential source of thromboembolic plaque, it can cause significant hypoperfusion by obstructing blood flow. One of the most extensive studies on the incidence of extracranial disease in symptomatic patients was presented by Hass and associates11 from the Joint Study of Extracranial Arterial Occlusion. They found that the most common site of plaque formation in the vertebrobasilar arterial system was the origin of the proximal vertebral artery (right vertebral artery, 18.4%; left vertebral artery, 22.3%). The second most common site was the middle vertebral artery. In this region, it is believed that the blood flow is dampened as it passes through the transverse foramina. Atherosclerosis occurs less frequently intracranially, in the mid basilar artery, and at the entry of the vertebral artery through the dura.
The natural history of extracranial vertebral artery atherosclerotic disease is not well known. Moufarrij and associates reviewed 96 patients with vertebral disease, 89 (93%) of whom had proximal extracranial disease at the vertebral origin.23 Most (75%) of these patients were asymptomatic in relation to their vertebral disease at presentation. Over an average of 4.6 years of follow-up, 19.8% experienced probable VBI symptoms, and another 2% suffered brainstem infarction. Recurrent stroke risks in patients with symptomatic extracranial vertebral atherosclerosis have not been well defined, although estimates of stroke risk in patients with symptomatic intracranial vertebrobasilar disease are 10% to 15% per year.24
Dissection
Spontaneous
The annual incidence of vertebral artery dissection (VAD) is about 1 to 1.5 per 100,25 and VAD is bilateral in 22% of cases.26 Spontaneous VAD is the term used to describe vertebral dissections that do not involve blunt or penetrating trauma as a precipitating factor. However, a history of trivial or minor injury is elicited frequently from patients with so-called spontaneous VAD. The diagnosis of traumatic VAD is reserved for patients with a history of significant trauma, including motor vehicle crashes, falls, or penetrating injuries. Spontaneous dissections are associated with systemic diseases affecting the arterial walls. In both the carotid and vertebral arteries, fibromuscular dysplasia is the most common associated condition in spontaneous dissection. It tends to affect areas where there is significant movement of the cervical spine and therefore occurs in the middle and distal segments of the vertebral artery. The formation of pseudoaneurysms is also quite common, although these lesions are often asymptomatic.18 Other risk factors include spinal manipulation, ceiling painting, nose blowing, oral contraceptive use, hypertension, cystic medial necrosis, migraine headaches, female sex, and recent infection.25 Extracranial vertebral artery dissection is characterized by headache (often occipital) or neck pain and signs of ischemia in the posterior circulation.26,27 Infarcts in the territory of the posterior-inferior cerebral artery (commonly with a lateral medullary syndrome) are seen in 13% of vertebral dissections.28 Intracranial vertebrobasilar dissection may present with symptoms of posterior circulation ischemia (particularly brainstem), subarachnoid hemorrhage (occurs in half of patients), or both.
Traumatic
Trauma is the third most common cause of vertebral artery disease. Both blunt and penetrating trauma can dissect the vertebral artery. Blunt injury occurs from cervical spine fractures and dislocations that may result in occlusion, pseudoaneurysm, or arteriovenous fistula (AVF) of the vertebral artery, especially in the middle portion. This type of injury can also be created iatrogenically from chiropractic manipulation. The most frequent site of thrombosis is at the level of C2 in the distal vertebral artery. This tendency may reflect the posterior placement of the vertebral foramina with respect to the vertebral body. The vertebral artery has an increased vulnerability to compression by subluxation of the cervical apophyseal joints. Blunt injury to the vertebral artery may be more common than has been quoted in the literature because these patients seldom undergo angiography unless they show symptoms of VBI. However, computed tomography (CT) can readily identify the patterns of cervical spine injuries, such as transverse foramen fractures and facet joint dislocations,29,30 which have been most frequently associated with vertebral artery injury, and CT angiography can provide a less invasive method for diagnosis of an underlying vertebral dissection.31 Penetrating trauma to the vertebral artery is less common than blunt trauma.
Compression
Compression of the vertebral artery can cause VBI. The anterior scalene muscle has been found to compress the vertebral artery at the level of C6. Osteophytes and disk spurs, found between levels C6 and C2, can encroach on and compress the middle vertebral artery, causing vascular symptoms. Usually, rotation or extension of the neck triggers symptoms. Such symptoms have been referred to as bow hunter’s syndrome, an uncommon condition in which the vertebral artery becomes symptomatically occluded during neck rotation.32 Typically, this has been described in relation to compression at the C1-2 level33,34 but can occur at other levels.35 Dynamic angiography has been recommended for patients who show vertebral artery symptoms on flexion, extension, or rotation of the neck.18
Subclavian Steal Syndrome
Subclavian steal syndrome was first described by Reivich and colleagues36 in 1961 when they discovered reversed flow in the vertebral artery. It is a disease not affecting the extracranial vertebral artery directly but leading to symptoms of VBI due to hemodynamic alterations in the vertebrobasilar system. It is caused by stenosis or occlusion in the subclavian or innominate artery proximal to the vertebral artery. If the pressure in the subclavian artery distal to the obstruction is low enough, it acts as a “sink” for the flow of blood from the vertebral artery and drains blood from the contralateral vertebral artery and even as far as the circle of Willis (Fig. 354-2). Hence, patients can experience VBI. Most of these symptoms are caused by use of the extremities when the demand for blood flow is increased and the pressure sink becomes more pronounced. In many cases, patients rarely experience symptoms at rest. The symptoms can be provoked by an arm challenge test. This has been further evaluated recently with flow measurements using QMRA before and after the arm challenge test,37 in which a basilar flow index (basilar artery flow to total intracranial flow) was calculated during the challenge test and compared with the baseline. A low basilar flow index correlated with VBI symptoms from steal.

Diagnostic Evaluation
Audiometric and Vestibular Tests
Occasionally, the presentation of vertigo or dizziness with no other findings requires consultation with an otolaryngologist to rule out labyrinthitis or vestibular causes. Noninvasive audiometric and vestibular tests can be performed. Audiometric tests include a pure-tone audiogram and a speech discrimination test to indicate hearing loss. A vestibular test can indicate decruitment and hyperactivity, which can be strong indicators of a centrally located lesion (sensitivity, 92%).17
Noninvasive Anatomic Imaging Techniques
Anatomic imaging of the brain and the posterior fossa is required as part of the evaluation. CT is an excellent imaging technique for ruling out mass lesions or hemorrhages and, in the setting of trauma, for evaluation of cervical spine fractures associated with vertebral injury. Magnetic resonance imaging (MRI) is highly sensitive and can detect demyelinating disease, stroke, and mass lesions. Diffusion-weighted imaging (DWI) is used in the evaluation of acute ischemic stroke38 and will provide early information about the location of acute focal ischemic brain injury.
Magnetic resonance angiography (MRA) or computed tomographic angiography (CTA) is a good noninvasive screening technique for evaluating the intracranial and extracranial arteries. Its ability to accurately and definitively identify stenosis is limited, however. The use of contrast enhancement may increase the utility of MRA.39 Transcranial Doppler (TCD) is another screening modality for vertebral disease but also lacks the sensitivity and specificity provided by other techniques.
Cerebral Angiography
Cerebral angiography is considered the gold standard for evaluating the intracranial and extracranial vessels of the brain. Unlike MRA, it is an invasive procedure and carries a low risk for stroke (1% overall incidence of neurological deficit, and 0.5% incidence of persistent deficit).40
In cases of extracranial vertebral artery disease, the aortic arch must be visualized, as well as the four major intracranial arteries. VBI symptoms can be caused by primary intracranial disease, and good visualization of the intracranial vessels is essential, including collateral supply, such as patent posterior communicating artery into the basilar top. Similarly, subclavian steal would be identified by reversal of flow in the vertebral artery ipsilateral to the subclavian artery stenosis or occlusion. Dynamic angiography can also be used to monitor vascular changes associated with head position, caused by soft tissue (ligament or muscle), neuronal tissue, or bone.18
Hemodynamic Evaluation
After an obstructive lesion has been identified, it is important to determine whether the VBI symptoms are from poor perfusion caused by the obstruction or by emboli. Cerebral angiography can give some sense of the cause, but it is far from reliable. Several methods have been used to evaluate the hemodynamics. Ultrasonography of the vertebral arteries has been used, but insonation is difficult, and its sensitivity is questionable. Variability in equipment, institutions, and technicians makes this method unsatisfactory.41 Intracranial hemodynamic changes have also been monitored with transcranial Doppler ultrasonography, but this technique is difficult to use in the posterior fossa. Imaging techniques used to assess tissue level perfusion, such as positron emission tomography (PET), single-photon emission computed tomography (SPECT), and xenon CT are of limited use in the posterior fossa because of imaging difficulties related to skull base artifacts and imaging resolution.
Since the 1980s, flow quantification using phase-contrast QMRA of the blood vessels has been studied.42–44 Although static MRI or conventional angiography is useful for determining the anatomy of the vessel, QMRA provides actual flow rates of blood in the vessel (in milliliters per minute). Both in vitro and in vivo flow studies have shown that velocities and volumetric flow rates can be estimated accurately for the carotid, vertebral, and major cerebral arteries. Normal values for flow rates in these vessels have been estimated.19 QMRA provides a noninvasive method for analyzing patients with VBI. Patients with VBI in the setting of steno-occlusive vertebrobasilar disease stratified by QMRA to have a normal flow in their distal intracranial vasculature had a recurrent stroke–free survival rate of 100% at 2 years, compared with those with low distal flow, who had a 71% stroke-free survival rate.45 Based on knowledge of the normal range of flow rates in these vessels, it can be determined whether obstructive lesions are significant enough to cause hypoperfusion of the vertebral artery. This knowledge may be helpful in selecting candidates for surgical or endovascular treatment.
Medical Management
Atherosclerotic Disease
Antiplatelet Therapy
Several antiplatelet trials have shown that aspirin reduces the relative risks for stroke, myocardial infarction, and vascular death by about 25%.46 Ticlopidine is more effective than aspirin but has important side effects. Clopidogrel is as effective as ticlopidine, with fewer side effects. In 1996, the European Stroke Prevention Study showed that dipyridamole effectively prevents stroke and, when combined with aspirin, is equivalent to ticlopidine or clopidogrel.47 These results can be applied to the medical treatment of extracranial vertebral artery disease. Recently, the American Heart Association/American Stroke Association Committee published their recommendation for the prevention of stroke in patients with noncardioembolic ischemic stroke or TIA.48 They concluded that aspirin monotherapy, clopidogrel monotherapy, and aspirin combined with extended-release dipyridamole all remain accepted options for initial therapy in patients with noncardioembolic ischemic stroke and TIA.
Two studies have reported outcomes from medical therapy for extracranial vertebral artery disease. Millikan and colleagues49 showed a decline in the mortality rate from 43% to 14% when heparin was used systemically to treat extracranial vertebral artery disease. Twenty years later in a 4-year follow-up, Whisnant and coworkers50 reported that the incidence of brainstem stroke decreased from 35% to 15% when oral anticoagulants were used. In neither study were the patients chosen randomly, nor did most of the patients undergo angiography. Meanwhile, outcome studies on the use of aspirin compared with warfarin for intracranial symptomatic atherosclerosis24 in the posterior circulation disease failed to show any benefit of warfarin over aspirin. The findings can be extrapolated with caution to the extracranial vertebral arteries.
Statin Therapy
The use of 3-hydroxy-3-methyglutaryl coenzyme-A reductase inhibitors (statins) has been evaluated for the prevention of ischemic stroke. The Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) trial51 demonstrated an 18% relative reduction in the risk for recurrent stroke in patients randomized to atorvastatin 80 mg per day versus placebo. Based on this clinical trial, the American Heart Association/American Stroke Association Committee recommended statin therapy with intensive lipid-lowering effects for patients with atherosclerotic ischemic stroke or TIA even without known coronary artery disease to reduce the risk for stroke and cardiovascular disease.48 Furthermore, recent data indicate that high-intensity statin therapy might regress plaque burden over time in patients with coronary disease.52 No such studies have looked specifically at extracranial vertebral artery disease.
Dissection
Anticoagulation Therapy
The treatment of vertebral artery dissection is based on rather incomplete evidence. Anticoagulation with heparin followed by oral anticoagulation therapy remains popular in most centers and is supported by demonstration of emboli as the most common cause of stroke in these patients.53 Anticoagulation with a target international normalized ratio between 2 and 3 is generally recommended for 3 to 6 months. This practice is supported by several small case series demonstrating good outcome with low complication rates in patients receiving anticoagulation.54,55 After 3 months, a follow-up angiogram or MRI is recommended. If the pathology persists, oral anticoagulation is continued for another 3 months. If reevaluation after 3 months (6 months after dissection) shows persistence of the pathology, oral anticoagulation is stopped, and the patient is kept on antiplatelet therapy for life. The rationales behind this approach are the high recanalization rate within the first 2 to 3 months after the dissection and the observation that, after discontinuation of anticoagulation, recurrence of symptoms occasionally may occur between 3 and 6 months after the onset of dissection but rarely after 6 months. Oral anticoagulation is contraindicated in intracranial dissections complicated by subarachnoid hemorrhage and in presence of a large infarct with associated mass effect or intracranial extension of the dissection.54 Antiplatelet therapy is an alternative to anticoagualtion53,54; however, there are no clinical trials available to determine whether antiplatelet therapy is equal or superior to anticoagulation owing to the low rate of recurrent ischemic events in patients with dissection. Furthermore, in a meta-analysis of 26 studies including 327 patients, Lyrer and Engelter found no significant difference between the two treatment options in the odds of death and in the odds of being alive but disabled.56
Thrombolysis
The role of thrombolysis in patients with acute infarction secondary to dissection has been explored.57,58 Thrombolysis treatment (intravenous and intra-arterial) has been successful in some patients with arterial occlusion caused by dissection if performed within several hours of onset.59,60 The thrombolytic agent acts on clots in both the true lumen and the false lumen of the dissecting vessel, resulting in reduced stenosis. However, in cases with associated subarachnoid hemorrhage, thrombolytic therapy has the potential to aggravate the risk for subarachnoid hemorrhage and should be avoided.61,62
Compression
After a diagnosis of rotational vertebral artery compression is established by dynamic vertebral imaging, surgical treatment is recommended. Conservative medical therapy consists of anticoagulation or neck immobilization, either by instructing the patient to refrain from head turning or by the use of a collar. In one review series of those treated conservatively, however, nearly 50% went on to infarct or had residual neurological deficits.63






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


