♦ Preoperative
Evaluation
- Detailed CN examination
- Computed tomography with 1-mm cuts and reconstruction in sagittal and coronal plane
- Assess anatomic relationship between bone and lesion
- Assess behavior of lesion with respect to bone (i.e., osteodestruction, hyperostosis, etc.)
- Assess anatomic relationship between bone and lesion
- Magnetic resonance imaging with and without gadolinium
- Assess soft tissue characteristics, including lesion, brain, vessels, CNs
- Magnetic resonance angiography/magnetic resonance venography if indicated for vertebral artery involvement/dominance, sinus dominance/patency, jugular bulb anatomy
- Consider cerebral angiography for embolization of vascular lesions, assessment of arteriovenous anatomy in region of lesion
- Headlight/loupes
- Mayfield head clamp
- High-speed drill
- Microscope
- Neurophysiologic monitoring: somatosensory evoked potential, motor evoked potentials, brain stem auditory evoked responses, pharyngeal leads, tongue/facial electromyographies
- Facial nerve stimulator (Kartush)
- Ultrasonic aspirator
- Consider lumbar drain for postoperative control of cerebrospinal fluid (CSF)
Operating Room Set-up
- Anesthesia apparatus should be placed at the foot of the table.
Anesthetic Issues
- Allow for neurophysiologic monitoring
- Arterial line
- Central venous access
- Sequential compression devices (SCDs)/thromboembolism deterrent stockings (TEDS)
- Dexamethasone 10 mg intravenous (IV) for intradural lesions
- Mannitol 0.5 to 1 g/kg IV bolus for intradural lesions
- Antibiotics
- Normocapnia
♦ Intraoperative (Fig. 15.1)
Positioning
- Supine with head turned parallel to floor and tilted toward the dependent shoulder to open up the surgical approach
- Avoid neck flexion to avoid further brain stem compromise
- With larger patients, a shoulder roll or lateral positioning may be necessary for adequate neck rotation
- Mayfield head pins: single pin on ipsilateral frontal bone lateral and posterior to supraorbital nerve, double pin on contralateral occipital bone
- Secure patients firmly with straps to allow intraoperative rotation
- Tape ipsilateral shoulder to foot of table, avoiding excess tension on brachial plexus
- All pressure points must be well padded to avoid decubiti
- Prepare and drape abdomen for free fat graft
Incision
- For bony tumors, transdural processes, or when full temporal bone resection is anticipated:
- C-shaped incision: begin two fingerbreadths superior to pinna, extend from level of external auditory meatus in coronal plane and curve posteroinfe riorly approximately two fingerbreadths medial to mastoid process, then extend anteroinferiorly into neck fold along anterior border of sternocleidomastoid muscle
< div class='tao-gold-member'>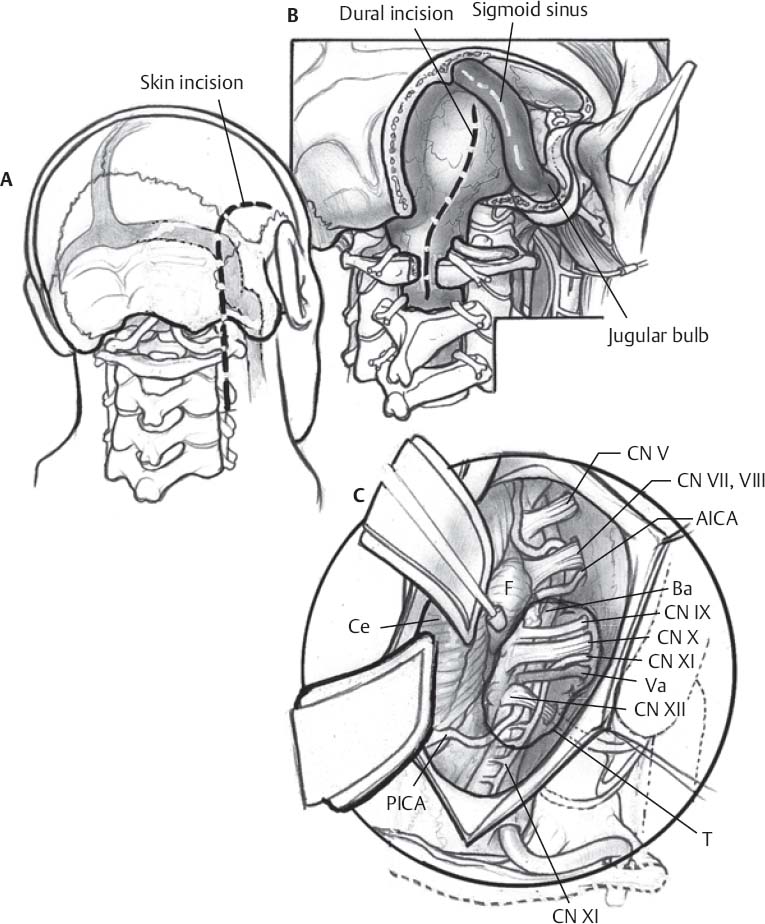 Only gold members can continue reading. Log In or Register to continue
Only gold members can continue reading. Log In or Register to continue
- C-shaped incision: begin two fingerbreadths superior to pinna, extend from level of external auditory meatus in coronal plane and curve posteroinfe riorly approximately two fingerbreadths medial to mastoid process, then extend anteroinferiorly into neck fold along anterior border of sternocleidomastoid muscle








