9 Free Functioning Muscle Transfers for Upper Extremity Reconstruction of Plexus Palsy A 16-year-old right-hand-dominant student was referred for right upper extremity paralysis reconstruction. At age 14, he was struck by a car while riding his bike. The initial right upper extremity injuries included (1) scapulothoracic dissociation, (2) devascularization of the arm due to complete subclavian artery disruption, (3) closed brachial plexus lesion with a flail arm, and (4) closed fracture of the humerus and scapula. He required revascularization of the right upper extremity. The brachial plexus was found to be incontinuity at the time of exploration. He was followed clinically and made a partial recovery from the brachial plexus lesion. Recovery plateaued at 2 years posttrauma. He presented with partial active use of the arm. Significant limitations included decreased active use of the shoulder and no active elbow flexion. He had partial strength of his hand and was starting to use it for assistance in some functional tasks. On examination, the right upper extremity was well perfused with normal capillary refill. There was marked atrophy of the deltoid, biceps, and intrinsic hand muscles. There was no thrill or bruit in the subclavicular fossa. The rhomboids, trapezius, serratus anterior, and latissimus dorsi had motor strength graded M4; deltoid M2; biceps M0; supra- and infraspinatus M3; pectoralis major M4; triceps, wrist, and finger extensors were M4, as were pronator, wrist, and finger flexors; and all intrinsic hand muscles were graded M0. Table 9–1 lists the passive and active range of motion measured for the right shoulder, elbow, and wrist. Grip strength on the right measured 0 kg and on the left 20 kg. Key pinch on the right measured 0 kg and on the left 4.5 kg. Dynamic two-point discrimination was greater than 8 mm in all digits. Light touch was assessed with Semmes-Weinstein monofilaments and was found to be 4.08 in the thumb, 4.17 on the ulnar side of the ring finger (Smith and Nephew Rolyan, Menomonee Falls, WI), and 3.22 in the small finger of the affected hand.
 Case Presentation
Case Presentation
| Passive Range of Motion (degrees) | Active Range of Motion (degrees) | |
|---|---|---|
| Shoulder | ||
| Abduction | 105 | 35 |
| Flexion | 140 | 40 |
| Extension | Full | 50 |
| External rotation | 20 | 0 |
| Internal rotation | Full | 90 |
| Elbow | ||
| Flexion | 140 | 0 |
| Extension | 0 | 180 |
| Pronation | Full | 90 |
| Supination | 45 | 45 |
| Wrist | ||
| Flexion | 45 | 60 |
| Extension | 60 | 40 |
| Radial ulnar deviation | Full | 0 |
X-rays of the right humerus showed anatomical alignment of a humeral fracture with internal fixation across the midhumerus. The underlying fracture was not visible. A chest x-ray showed no parenchymal lung disease. The right hemidiaphragm was normally positioned. Arteriography revealed patent right brachiocephalic, subclavian, axillary, and brachial arteries. There was fusiform dilatation of the right axillary artery, likely related to previous surgical patch angioplasty. A large branch of the circumflex humeral artery was noted. Electromyographic studies showed complete denervation of the right biceps. The motor units in the right pectoralis major muscle showed changes of rein-nervation. The activity in the latissimus dorsi was normal.

Figure 9–1 (A, B) At 1 year postop, the patient had 80 degrees of active elbow flexion. (A: Anterior view, B: Lateral view.)
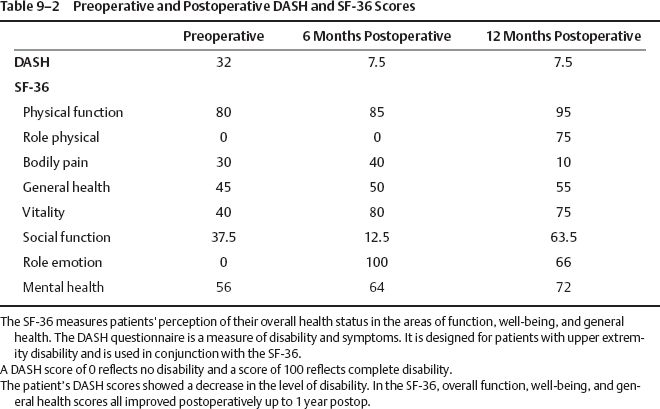
Elbow flexion function was restored with microneurovascular muscle transfer using the left gracilis muscle (as detailed following here). At 1-year postop, this patient had 100 degrees of active elbow flexion. Muscle motor strength has been graded M4 (Fig. 9–1). He is currently working on increasing biceps muscle strength and endurance. There were no respiratory complications following harvesting of the intercostal nerves. Comparison of pre- and postoperative Disabilities Arm, Shoulder, and Hand (DASH) and Short Form (SF)-36 scores confirm a significant reduction in disability and overall improvement in quality of life following this procedure (Table 9–2)
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


