Chapter 27 Full-Endoscopic Interlaminar Lumbar Discectomy and Spinal Decompression
Minimally invasive techniques can reduce damage to tissues and limit the consequences of necessary tissue damage [1,2]. Endoscopic operations possess advantages that raise these procedures to the standard in many areas. Working with lens optics under lavage provides excellent visual conditions, and bleeding can be reduced. Also, the use of the laser or high-frequency bipolar current is possible in the immediate vicinity of neural structures [3]. The prerequisite for any minimally invasive technique is that the technical possibilities of such operations guarantee attainment of the operative goal [4].
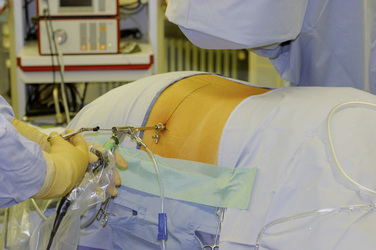
The most common fully endoscopic uniportal procedure is the transforaminal or extraforaminal operation with posterolateral access (Fig. 27-1) [5–8]. It is seldom technically possible to perform retrograde resection of disorders within the spinal canal intradiscally. For this reason, the newly developed lateral access is necessary within the transforaminal technique to reach such structures because of the bony boundaries of the intervertebral foramen and the access pathway through the soft tissue (Fig. 27-2) [9]. At the caudal levels, this access may be hindered by the pelvis. Additionally, the boundaries of the foramen hamper mobility during the procedure and limit the available room to work in the spinal canal.

The fully endoscopic uniportal interlaminar technique can be used for transforaminal lumbar problems that are technically inoperable. The spinal canal is reached through the interlaminar window and enables working comparable to that with conventional techniques but in a minimally invasive procedure (Fig. 27-3) [1,10,11]. The known problems of open, microscopic, and endoscopically assisted techniques can be reduced [1,2].

At the same time, technical problems have been solved by the development of new lens endoscopes with intra-endoscopic 4.2-mm working canals and corresponding new instruments, shavers, and burs (Fig. 27-4). This development also enables the resection of bones as in arthroscopic surgery [10,11].

Advantages
Conventional open operating procedures are indispensable today and will remain so in the future. The possible complications of and injuries from such procedures are known [12–19]. At the least, new techniques must be as capable of attaining the operative goals as the established procedures [4].














Indications
The indications for the operation correspond to today’s valid standards [20]. Most experience has been gained in the therapy of disc herniations and lateral spinal canal stenosis. Extensive central spinal canal stenosis has been operated on for only a short time, and the procedure is still under development. Existing concurrent pathologies, such as instabilities, must be treated at the same time as appropriate. The following indications are currently clearly defined:
 Sequestered or nonsequestered disc herniations within the spinal canal: In the case of extensive dislocation to the next level, a two-level procedure may be performed; in the case of a herniation in combination with intraforaminal-extraforaminal prolapses, an additional fully endoscopic transforaminal operation may be performed.
Sequestered or nonsequestered disc herniations within the spinal canal: In the case of extensive dislocation to the next level, a two-level procedure may be performed; in the case of a herniation in combination with intraforaminal-extraforaminal prolapses, an additional fully endoscopic transforaminal operation may be performed.



Contraindications
 Compressing intraforminal or extraforaminal pathologies: In this case a fully endoscopic transforaminal or extraforaminal procedure with posterolateral to lateral access is indicated.
Compressing intraforminal or extraforaminal pathologies: In this case a fully endoscopic transforaminal or extraforaminal procedure with posterolateral to lateral access is indicated.



Preoperative preparation
Examination
 The decision for surgery must be made according to today’s standard on the basis of radicular pain symptoms and existing neurologic deficits [20]. Isolated back pains cannot usually be improved by decompressing operations.
The decision for surgery must be made according to today’s standard on the basis of radicular pain symptoms and existing neurologic deficits [20]. Isolated back pains cannot usually be improved by decompressing operations.

Informed Consent
 Patients must be informed about their disease and its possible long-term course and consequences. Despite the minimal invasiveness and attendant advantages of the surgical procedure, all known side effects, complications, and therapeutic possibilities must be explained, as would be done for conventional procedures [21].
Patients must be informed about their disease and its possible long-term course and consequences. Despite the minimal invasiveness and attendant advantages of the surgical procedure, all known side effects, complications, and therapeutic possibilities must be explained, as would be done for conventional procedures [21].

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


