♦ Preoperative
Imaging
- Anteroposterior, lateral, and open-mouth cervical spine radiographs
- Cervical flexion/extension radiographs if not contraindicated by acute neurologic deficits or acute fractures
- Computed tomography (CT) with f ine cut bone windows and two- dimensional reconstructions; measurements and trajectories must be planned using a stereotactic workstation
- Magnetic resonance imaging when indicated (e.g., myelopathy)
Equipment
- U-loop system for occipital-C2 fusion. May use Avery-Brockmeyer- Thiokol (Medtronic) plate or other occipitocervical plate–rod construct (e.g., DePuy, Synthes)
- C1–2 transarticular screw instrumentation (Aesculap, DePuy, Sofamor-Danek)
- Multistranded titanium cables
- Mayfield head holder with infinity support system (horseshoe adapter)
- Brain stem auditory evoked potential (BAER) and somatosensory evoked potential (SSEP) monitoring when indicated (e.g., myelopathy)
- Bone graft tray for harvesting autograft from iliac crest or rib
- C-arm fluoroscopy
Anesthetic Issues
- Fiberoptic intubation
- Arterial line for blood pressure monitoring
- Intravenous (IV) antibiotics given 30 minutes prior to incision
♦ Intraoperative
Monitoring
- Baseline SSEPs prior to positioning and after final positioning
- Motor evoked potentials (MEPs), BAERs may be monitored intraoperatively
Positioning
- Patient prone with neck in military position and head secured in Mayfield skull clamp (infinity horseshoe adapter may be used for added support in patients less than 2 years of age)
- Confirm desired alignment with lateral fluoroscopy during positioning
Minimal Shave
- Electric razor
- 2-cm wide strip shaved in the midline occipital and cervical regions
Sterile Scrub and Prep
- Prep and drape allowing for the harvest of posterior iliac crest bone graft if age > 3 years or rib graft if age < 3 years
Incision and Subperiosteal Dissection
- Infiltration with local anesthetic
- Linear, midline incision from suboccipital region to spinous process of C3, through dermis only
- Needle-tip monopolar cautery to open subcutaneous tissue and superficial fascia
- Nuchal fascia and posterior cervical muscles are divided in the midline with blunt-tip monopolar cautery for an avascular dissection.
- Midline periosteum of the occipital bone, posterior ring of C1, and the spinous processes of C2 and C3 are incised with monopolar cautery.
- Lightweight periosteal elevator or monopolar cautery is used to sweep the paraspinal muscles laterally off the squamous portion of the occipital bone and the posterior elements of C1 through C3 in the subperiosteal plane, avoiding exposure of the vertebral arteries.
- Angled, self retaining Weitlaner retractors are placed to maintain the exposure.
- Subperiosteal dissection is continued with curettes to dissect soft tissue from the rim of the foramen magnum, the superior and inferior edges of the posterior ring of C1, and the superior and inferior margins of the C2 laminae.
- Expose C1–C2 articular surfaces and C2 pars interarticularis.
C1–C2 Arthrodesis (Transarticular Screw Placement)
- Make percutaneous stab incisions inferolateral to incision based on fluoroscopic guidance using a drill bit to estimate the trajectory that will be required for screw placement.
- The author prefers a 2.9 mm drill bit and a 3.2 mm tap for 3.5 mm screws or a 3.5 mm tap for 4.0 mm screws.
- Identify screw insertion point and define medial/lateral angulation based on preoperative stereotactic planning.
- Prepare pilot hole with drill bit or awl.
- Penfield no. 4 is placed along the exposed surface of the C2 pars into the atlantoaxial facet joint and gently retracted upward to displace the C2 nerve root and venous plexus superiorly. This exposes the C1–C2 articulation and C2 pars. It is also used to guide the drill trajectory up the C2 pars. Make certain the medial and lateral edges of the pars are clearly defined.
- Reduce C1–C2 subluxation if necessary (clamp on C2 spinous process can be helpful).
- Fluoroscopy is essential.
- Drill trajectory will aim toward the anterior C1 arch just ventral to Penfield no. 4 and based on preoperative planning.
- Lateral fluoroscopy is essential.
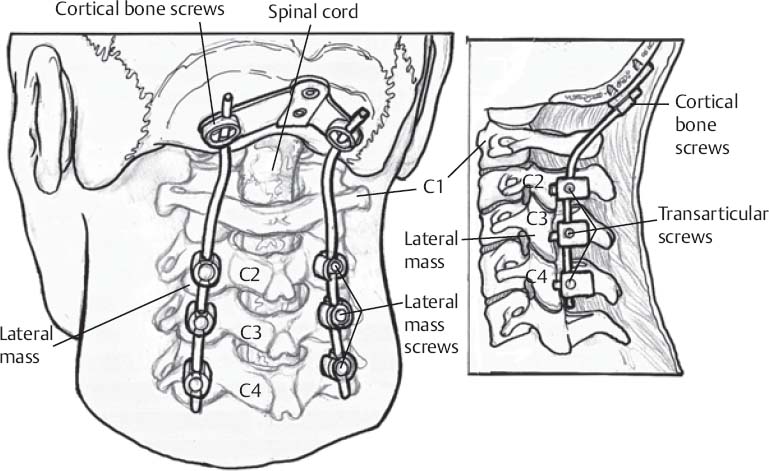
- Screw will be placed through central axis of C2 pars interarticularis (Fig. 162.1).
- Tap along the determined trajectory.
- Insert cortical bone screws.
- Screw diameter based on anatomy (3.5 or 4.0 mm screws most commonly available; Fig. 162.1)
- Cannulated screw with Kirschner wire may be used if desired.
- Penfield no. 4 is placed along the exposed surface of the C2 pars into the atlantoaxial facet joint and gently retracted upward to displace the C2 nerve root and venous plexus superiorly. This exposes the C1–C2 articulation and C2 pars. It is also used to guide the drill trajectory up the C2 pars. Make certain the medial and lateral edges of the pars are clearly defined.
Occiput-C2 Arthrodesis
- If a loop construct is used, it is positioned and affixed to the transarticular screws often via titanium couplers; it is snugly fit against the occiput and screws are then placed to anchor the construct to the midline occipital keel.
- If a rod construct is used, the occipital plate is fitted to the occipital bone and secured as described; rods are then contoured or variable angle rod joints are adjusted to optimally fit the occipital-cervical curve and then secured to both the occipital plate and transarticular screws.
- Bicortical posterior iliac crest or rib bone graft is harvested and gardened to fit with maximal bony contact on the occipital bone and C2.
< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel






Full access? Get Clinical Tree


