Part II 1. Neural therapy according to Huneke is a regulating therapy, i.e., a holistic therapy. The healing stimulus produced by means of a correctly placed neural-therapeutic substance produces a response from the whole of the neurovegetative system whose pathways are those taken by both illness and recovery. 2. Segmental therapy according to Huneke refers to the selective use of procaine or lidocaine in the area of the disease process. Always examine first, then test! The improvement achieved with segmental treatment increases with repetition up to complete cure. If segmental treatment fails to produce an improvement, look for the interference field. 3. Any chronic ailment can be due to an interference field. 4. Any part of the body can become an interference field. 5. The injection of procaine or lidocaine, repeated as necessary, into the responsible interference field will cure the disorder caused by it, as far as this is anatomically still possible, by means of a lightning reaction (Huneke phenomenon). 6. The conditions for a lightning reaction are: a. All disturbances remote-controlled from the interference field must disappear completely, as far as this is anatomically still possible, at the moment of the injection. b. Freedom from all symptoms must continue for at least 20 hours (8 hours in the case of teeth). c. If the disorder recurs, the injection (s) must be repeated, and the period of freedom from symptoms must clearly increase with every subsequent treatment. A Huneke phenomenon has been produced only if this criterion has been met. 7. If injection into the segment produces no substantial improvement or into a suspected interference field does not produce a 100% lightning reaction, further injections at these sites are pointless. 8. Always try simple injections with small quantities of local anesthetic first, with few but well-placed injections. Injections into the sympathetic chain and the ganglia are our last resort. A doctor who wants to help his or her patient must also be familiar with these. Do not stop treatment until you have tried everything. 9. All suspect teeth must be tested in a single session, similarly all scars. All scars in the same segment must always be injected as part of any segmental treatment. 10. NOTE: Intra-arterial injections into a vessel leading to the brain or into the subarachnoid space can have serious consequences. Always protect your patient and yourself by prior aspiration. → denotes that the key word following this sign is listed in the Alphabetical List of Conditions and Indications in the following Part II; → (T) denotes the key word following this sign is listed in alphabetical order in Part III, Techniques, where the technique for the injection may be found. Try everything and keep what proves good. This is and remains the sole aim of all the sciences, and of medicine in particular. Hufeland Neural therapy is an art of healing. The art of healing is a combination of 70% diligence and technique and 30% flair and artistic intuition. It cannot be put in the strait-jacket of dogmas and rigid rules. Rigidity is the greatest enemy of art. But there are basic rules in every form of art, which it is essential to master. At first sight, it will seem presumptuous to claim to cure so many different disorders by means of a single preparation. But ultimately all disorders have one thing in common, namely that they arise in the organism on the ubiquitous pathways of the neurovegetative system, on whose functions our very lives depend. Any persistent disequilibrium in this finely balanced energy system is synonymous with illness. Neural therapy acts at this crucial point as a means of restoring the equilibrium and of regulating the functions. This book is designed primarily for use by the practicing doctor as a work of reference. It includes a small selection from the vast literature on the subject and from my personal experience. It is intended to communicate to my overworked professional colleagues a summary of the collected experience gathered in 65 years by the Huneke brothers and their disciples. It provides brief information on the means recommended by modern neural therapy as effective in treating the various symptoms listed. Obviously the discussion can only contain suggestions. No case is identical with another, for there are as many disorders as there are patients. We are sufficiently self-critical to know that whilst neural therapy is a far-reaching and very effective method it is no panacea. We do not try to smash the head of a tapeworm by injecting it with a carefully aimed hypodermic filled with procaine. For that, we, too, use an antithelmintic preparation. Anyone who leafs through this alphabetical list will quickly recognize the essential elements of what is our attitude to illness and what means are available to us for curing it. Every one of the injections listed and described in greater detail in Part III Techniques, may by itself be enough to enable us to achieve our objective, but often a combination of several injections in the segment is preferable. A single treatment might be sufficient to induce cure. In acute disorders the treatment should as a rule be repeated when the effect wears off. In chronic disorders we normally carry out our tests and/or treatment once a week until they are effective. Unless specifically stated, all types of injection and all quantities given refer to 1–2% procaine preparations or adrenalin-free 0.5–1% lidocaine solutions, in the form in which these are generally available as neural-therapeutic drugs. After each key word the note could be added that if treatment in the area of the disorder and/or its related segment does not produce the desired result, one should search for the interference field. It is only when this has been done thoroughly and conscientiously without avail that we may set our physician’s conscience at rest and discontinue neural therapy on that particular patient. Individual cases—rules—art—individual case. This is the great cycle. Much Scientific skepticism towards miracle-healers and methods whose effective spectrum is suspect is a healthy and essential safety measure against charlatanism. Let us therefore emphasize again: neural therapy with local anesthetics is not even in our eyes an omnipotent means for curing the sick. But it is a substantial enrichment of our diagnostics and therapy as a whole. In our age of specialization we try to exploit every opportunity neural therapy offers with its objectively demonstrable action on cybernetic regulating processes. We do so to the extent that we regard reasonable and responsible and wherever it is possible. In the nature of things, it is frequently possible in the large number of symptoms produced by autonomic dysregulations. In some cases, the emphasis is on pain, in others it is on disturbances of internal and external secretions or of the blood supply, or of disturbances of blood composition or dyskynesia of the striated and smooth musculature. All these neural irritations, from dysregulation to dystrophy, are capable of producing innumerable syndromes and diseases, from abdomen to xiphoidalgia, and to keep them active. Anyone who has read and understood the works of Bergsmann, Heine, Kellner, and Pischinger on the influence of foci and interference fields upon the autonomic system and on that of our regulating therapy on biocybernetic functions will know that there is an important common denominator in all pathological processes. To him or her this alphabetical list of conditions and indications will no longer seem too extensive. Only the critic who is not conversant with such objectively demonstrable facts will continue to assume, when he or she looks at the broad spectrum of indications, that we are blinkered monomaniacs. In essence, the start of any treatment is an experiment. This also applies to neural therapy. In neural therapy, neither the indications nor the successful cure can always be determined beforehand with absolute certainty. Thus, its possibilities and limitations cannot be established a priori. This creates difficulties in trying to fit it into the structure of orthodox medicine. In one case, a single attempt may be enough to produce a surprise cure. In others, which apparently present with the same primary symptoms, the same approach may fail. It all depends on the specific circumstances of each individual case. In pathogenic processes, cause and effect are rarely in a linear cause–effect relationship, but are far more generally dependent on the regulatory processes and thus interact mutually, i.e., based on different pathophysiological circumstances. This is also why the effects of neural therapy cannot be established by conventional statistical and pharmacological studies. Our inability to ascertain the relationships accurately in this case ought not to be used as pretext to reject neural therapy on account of prejudice. To do so would fail to do justice to the physician’s duty to try anything that holds out hope of success and does no harm. Neural therapy cannot wait until the way in which it acts can be determined with absolute certainty. In practice, success is always more important than explanation. In the following Part II, I will describe a number of diseases with advice for their therapeutic treatment. They are listed alphabetically with the name of their common diagnosis. The neural therapist knows that we do not treat statistically useful groups of indications, symptom complexes, or disease patterns, but always suffering individuals with their different constitutions, dispositions, health history, and basic autonomic condition. They all respond differently. We do not think in terms of “rheumatism,” “migraine,” “asthma,” etc., but always of individuals who suffer from comparable disorders with varying origins. Thus, regulation therapy cannot offer template-like treatment suggestions for all the cases with the same “diagnosis.” Each patient follows a different path leading to the outbreak of an ailment. Based on case history and examination, we perpetually have to search amongst all the possibilities for the accurate way that leads to the individual cure. Unfortunately and in spite of all our truthful efforts, it will not always be possible to find that way. Often enough, the selective pinpoint use of local anesthetics will in itself be enough to achieve an improvement in the illness and, ideally, to restore normality. In other cases, such as pneumonia, tuberculosis, cancer, and shock, neural therapy can play an important supporting role side by side with other, conventional methods and the use of “essential” drugs. I have never said that these disorders should be treated solely by neural therapy. The main point where we can help is obviously in functional disorders. However, we know that what may begin as purely functional disturbances, for example, those involving the stomach, gallbladder, and heart, can ultimately escalate and become organic. A process due to a focus or an interference field can result in genuine organic damage to the heart, kidneys, and joints. Of course, we cannot eliminate major pathological organic changes. But we can influence the secondary functional disorders they produce that remain inaccessible to conventional therapy. Pathomorphology can produce a feedback effect and create a vicious circle that makes conventional therapy ineffective. In such a case, the abnormal functional circuits can be normalized to such an extent by neural therapy that other treatment forms can become effective again. As neural therapists, we avoid the temptation to overstate our successes and become too one-sided, by constantly reviewing our position with a critical eye. We must always act in accordance with the precept suprema lex salus aegroti (the supreme law is to heal the sick). Despite our enthusiasm for this method, our conscience as physicians and our sense of responsibility towards our patients always obliges us anew to remain aware of our limitations. The indications listed below have not materialized out of thin air; they are no mere fabrications and inventions. All are based on publications over the years that bear witness to the successful treatment of these disorders by neural therapy. In addition, for most of them, I can offer the testimony of my personal experience of over 45 years in the practice of neural therapy. Abdomen It is no accident that we deal with all disorders affecting the abdominal organs as a single entity: liver, gallbladder, stomach, duodenum, pancreas, spleen, small and large intestines. There are no sharp boundaries in the living organism, merely flowing transitions. The organs listed above demonstrate this particularly clearly, for the functions of each are so dependent on the functions of the others that all of them together also form a single entity in a pathophysiological sense. A healthy digestive system requires that all the organs involved in the digestive processes act harmoniously and in concert with one another. Gallbladder We know from the pathologists that 75% of the entire human race will suffer from some form of gallbladder complaint in the course of a lifetime, but that only 8% will die from it. Eighty percent of all acute gallbladder disease is cured after conservative treatment or will change to a latent state. On average, 15% of all adults have gallstones, 25% being men and the other 75% women. Other sources state that 40% of all women over 40 have gallstones. It is a striking fact that three times as many women who have borne children are affected than those who have remained childless. This is enough to make any experienced neural therapist think immediately of a possible interference field in the pelvic region. Gallbladder disease is primarily a general disorder. It is preponderantly a metabolic disturbance, irrespective of whether it is inflammatory or whether gallstones play the main part. In 35%, a biopsy will show fatty degeneration of the liver, 8% of those suffering from gallstones are also diabetics, and a far greater percentage presents with a latent diabetic metabolic state and adiposity. Incidentally, colic is no proof of gallstones; 10% of those suffering from biliary colics do not have gallstones. Surgeons have for a long time demanded that surgery should be undertaken early, since there is little risk at that stage. To their chagrin, the physicians have given only lukewarm support to this demand and the patients’ response has so far been disappointing. This may well be due to a relatively high mortality rate of up to 8% (above 50 years 10%) and a failure rate of 35%. Unfortunately, gall-bladder disorders generally occur after the age of 40, when mortality following surgery is in any event relatively high. No wonder, therefore, if gallbladder surgery does not stand in high repute: one out of 10 patients dies, three out of 10 will be no better afterwards. For these 30%, the meaningless term “postcholecystectomy syndrome” has been coined. For these surgical failures, faulty diagnosis or newly formed stones are held responsible, together with changes in the pancreas, and hepatitis, cholangitis, and dyskinesia. At the 1971 international Surgeons’ Congress in Moscow, Cowie and Clark reported a significant observation: following vagotomies and cholecystectomies, the biliary ducts become hypotonic and this may lead to the formation of gallstones as a result of stasis or retention of bile. This not only explains why new stones are formed again after surgery to remove gallstones. It also enables one to conclude that any irritation of the vagus may have a lithogenic effect. But we can deal therapeutically with reflex hypotonicity of the biliary ducts, which may be caused by irritation of the vagus, by attacking it via the → (T) (abdominal) sympathetic chain, either before or after surgery. Or instead of surgery! The surgeons’ argument that cholecystectomy is an effective prophylaxis against cancer and that this, according to them, is enough to justify the risk, proves to be no argument at all when looked at a little more closely: only 1% of all gallstone sufferers develop cancer of the gallbladder. Nor does surgery to deal with “adhesions” bring much for the patient: only 2.5% of follow-up operations were found to be indicated (overlooked stones, papillary stenosis). For the other failures, a strenuous search for the culprit continues in every direction: irritable colon, hiatus hernia, duodenal ulcer, achlorhydric gastritis, intestinal allergies, lactose intolerance, cirrhosis of the liver, ulcerative colitis, coronary affections etc. In other words, the search concentrates exclusively on the attendant symptoms and consequences of surgery, instead of facing up squarely to the unpalatable fact that the true cause is an interference field. Out of 100 people with gallstones, 90 never know they have them, or at least they are not aware of them until their doctor tells them that they have them. Only the remaining 10 become gallstone sufferers. Apart from iatrogenic and/or psychogenic causes, the factor that must enter the picture before a gallstone carrier without symptoms becomes someone suffering from gallstones is an interference field. Since Huneke has shown us how to eliminate interference fields, we are now able to turn someone suffering from gallstones back into a healthy carrier of gallstones again. Conservative therapy must therefore start with the interference field, if it wants to be included in the discussion, not by dealing with dyskinesia and bacteria that settle in the gallbladder only secondarily! By the large number of cures achieved even amongst patients who have had unsuccessful gall-bladder surgery, neural therapy has proved that in the clinical picture of gallbladder patients an interference field is particularly frequently the activator of deviant metabolic behavior and of secondary dyskinesia, stone formation, inflammation, adhesions etc. Only disturbances due to segmental factors can be cured by local measures within the segment. Surgery is a form of segmental treatment. But about 30% of all cholecystopathies are not segmental in origin but are due to an interference field, and these form the majority of the cases that cannot be treated successfully by surgery. They have to be treated on an individual basis, in which organ-linked thinking and action yield to a cybernetic approach and a holistic therapy. The specialist in internal medicine ought not to refuse a priori to discuss neural therapy. Instead, he or she might try it once or twice without prejudice (and, of course, competently) before turning over his or her patient to the surgeon. If a woman patient states, as is so often the case, that she started to get fat after her second child and that her biliary colics began about this time (Speransky’s “trigger effect”), he or she must find and eliminate the interference field in the → (T) pelvic region and, if necessary, also treat the → (T) thyroid, in order to allow her biliary ducts to leave her in peace. A gallbladder operation in such a case would be totally mistaken and would merely produce fresh neural interference fields (see Case Histories 12 and 14 in Part I, Section C, Chapter 2). How many women could be helped if only this fact were more generally known amongst doctors? If we state that every gallbladder patient should be treated by neural therapy with procaine, the “surgeon’s bloodless knife,” as early as possible, we base this demand on numerous cures. The deviant metabolic behavior has to be brought back into line first, before the secondary changes become too widespread. Acute indications such as empyema, phlegmons, pericholecystitic abscesses, and occlusion due to stones with persistent icterus, obviously belong in the surgeon’s hands and must not be delayed. Segmental biliary conditions can be cured better and with less risk with procaine than by surgery. The patient whose gallbladder affection is due to an interference field, however, can be helped only via the Huneke phenomenon and, in such cases, the pointless operation (with all its consequences) should be strictly avoided (see Case History 8 in Part I, Section C, Chapter 2). Hence, neural therapy before cholecystectomy, early treatment with procaine instead of early surgery! If segmental treatment fails to be effective and if no interference field can be found as the cause, there is still time to fall back on surgery. Based on my own experience, I would estimate such cases to amount to less than 30%, and these include a large number of psychogenic cases. I should therefore also recommend involving the psychotherapist before the surgeon. “Thou shalt not harm” must be our first commandment, especially in treating gallbladder patients. Liver Over the years, the methods of investigation and treatment of the various organs have become so differentiated and complex that the general practitioner can no longer understand them. So, for example, there are over 170 liver function tests alone! The one thing they all have in common is that they are not absolutely reliable. A divergence between loss of function and anatomical diagnosis is uncontested. Thus, only a liver biopsy can establish with certainty the presence of any of the numerous forms of hepatitis and fatty degeneration of the liver. Fintelmann wrote that “in hardly any other medical specialty is there such a discrepancy between almost perfect diagnostic tools and techniques on the one hand and disappointingly unspecific therapy on the other as there is in hepatology.” As far as the patient is concerned, he or she is far better served if we give him or her a timely injection to the abdominal → (T) sympathetic chain and into the → (T) epigastrium rather than wasting precious time trying to solve the riddles that often conflicting laboratory reports set us. The patient who is treated actively will gratefully notice that our injections have eliminated the pressure he or she has felt in the liver region and that at the same time he or she has stopped feeling ill. We know from experience that the illness disappears when we stop feeling ill, which helps to cure the ailment more rapidly and with less complications. Only an improved blood circulation can help to effectively prevent the development of chronic progressive hepatitis, liver atrophies, and cirrhosis of the liver. Once a cicatrization with excessively destroyed tissue has developed, our injections cannot reverse this condition. A chronically diseased liver is no contraindication for neural therapy. Quite the reverse, for the liver is one of our most successful fields of activity. Based on the success of the anesthesia of the right abdominal sympathetic chain, it is fair to assume that, in addition to its known functions, the liver has an important autonomic regulation function in the corresponding segment and as the origin of an interference field. The local anesthetics with amid structure (lidocaine etc.) are not fit for the treatment of acute hepatitis or chronic liver damage because detoxification takes place in the liver. Cirrhosis of the liver In advanced conditions with excessively damaged functional tissue, positive results from our therapy cannot be expected. However, there is no reason to give up entirely. Stimulation and support of self-healing processes are still indicated. The following case demonstrates that there is a chance for success. Case History 21: A. S., Aged 58 In 1962, A. S., a woman of 58 years from Munich, suffered an infectious hepatitis, which required 8 weeks of hospitalization in 1963. She was diagnosed with an inflammatory episode of chronic hepatosis. The laboratory results indicated a severe damage to the hepatic parenchyma. She was treated with high doses of cortisone and hepatic medication. The hepatic puncture that was done before her discharge led to the conclusion “old and new liver cell damage.” Eleven years later, in the presence of her husband, the senior physician of a Munich clinic told her bluntly that, “according to the diagnosis of the hepatic puncture, she was suffering from advanced liver cirrhosis, which is incurable and her life expectancy was at best another 4–6 years.” He might have been a good physician but was certainly not a good psychologist and definitely a bad prophet! After a successful sciatica treatment, the husband asked me, without his wife present, if there was really nothing that could be done, not even for the constant pressure in the abdomen and the unpleasant eructations. I was willing to try it. After six injections into the right celiac ganglion and the epigastrium preperitoneally the pain improved. The pain had disappeared after 11 treatments. Her general condition and the results of her liver test improved. After 21 treatments (in the course of 15 months), scintiscan and tomography was without pathological findings. At the end of 1976, an ovarian carcinoma was treated with surgery and radiation and cytostatics. In addition, beginning in 1977, peritoneal tuberculosis that she had in childhood had returned and was under treatment. The liver had to deal with another 3 months of tuberculostatics. The liver tests showed temporary worsening of the condition, which became normal again after the strong medication was discontinued. Test results in January of 1978: GOT 22, GPT 34, gamma-GT 27, LDH 272 mu. Between 1978 and 1983, the annual control sonography showed no metastases, merely “the liver measures 11 cm in the medioclavicular line, fat and connective tissue deposits.” Test results in 1984: GOT 21, GPT 22, gamma-GT 31, LDH 3.9 U/l. For the last year, the patient has not taken any medication. 10 years after her “death sentence,” she feels very well for her age. Now, what was that? Was it a wrong diagnosis, suggestion, spontaneous healing, or the success of neural-therapeutic segmental therapy? In 1989, through laboratory tests on rats with (carbon tetrachloride–induced) liver cirrhosis, E. Hanisch and his colleagues tested the influence of splanchnicectomy on the hemodynamics of the liver region. They discovered a 50% increase of the arterial blood flow to the liver with a simultaneous lowering of the pressure in the portal vein! This research was discussed in the East Berliner Zeitschrift fuer klinische Medizin (Magazine for Clinical Medicine). It stated that, “this approach requires further investigation, because it shows the potential for a new therapeutic concept. Supported by sonography, the blockage of the celiac ganglion can be performed in humans as well.” My comment here: “You got there late, but you got there!” Since 1953, the therapeutic “blockage” principle, even without sonography, has been successfully applied thousands of times by neural therapists! Dystrophy (protein deficiency) effects Late effects of malnutrition in prison camps include liver damage, infection → immune deficiency, “vegetative dystonia,” and endocrine insufficiency. Most serious are the affections of the neurovegetative regulating mechanisms. The frequent result is a change of tonus of the sympathetic system. The generally “functional” disorders respond well to systematic procaine therapy. Hepatitis Acute hepatitis accounts for 20% of all notifiable diseases in Germany, around 30 000–40 000 cases a year. The true figure is likely to be substantially higher, since 30–50% of all cases of hepatitis never show the characteristic symptom of jaundice. We may therefore have to assume that the patient has had hepatitis and that his or her liver is acting as an interference field even if he or she cannot tell us that he or she has ever suffered from liver disease. The number of spontaneous cures in acute hepatitis is believed to be about 90%, whilst 1% of those suffering from it die in the early stages of the disease, 1% develop cirrhosis of the liver and the remaining 8% become chronic. Injections as early as possible into the → (T) sympathetic chain, repeated once or twice weekly, make the jaundice disappear surprisingly quickly, and the enlarged liver and the pathological laboratory results return to normal. The period of illness is cut by half and all the subjective symptoms are greatly improved as a result of the better blood supply to the liver. This treatment is the best prophylaxis against liver atrophy and other late effects such as interference-field formation. In the case of post-hepatic effects, such as hypodynamia, which may persist for months, producing fatigue, low energy, hypotonia, collapse tendencies, and could be a sign for adrenal insufficiency, injections to the → (T) celiac ganglion (abdominal sympathetic chain) are an effective treatment that reduces the recovery time considerably. Other practitioners recommend → (T) peridural anesthesia between T8 and T12, but this is technically more difficult and offers no advantages by comparison with our method. Repeated → (T) intravenous procaine injections have proved effective against the distressing itching in jaundice. Segmental therapy can turn aggressive hepatitis, confirmed by histological and laboratory examination, into a persistent form and ultimately cure it. One case that represents several similar cases will demonstrate this in the following. Case History 20: H. K. Factory Worker, Age 39 In January of 1975, at the age of 39, the factory worker H. K., female, from Eching was in a severe car accident: shock, rib fractures on both sides with contusion pneumonia, pelvic ring fracture, and splenic rupture. A splenectomy and eight blood transfusions were required. Six weeks later she suffered an acute viral hepatitis that was treated with cortisone (50 mg going down to 15 mg). In May, a liver biopsy showed a still active progressive hepatitis that was treated with 20 mg Ultralan (fluocortolon) and 100 mg Imurek (azathioprine) per day. After the transaminases returned to normal, the patient was released in June to the care of her family physician, with the recommendation to continue the daily treatment with 100 mg Imurek and 5 mg Ultralan. In spite of the medication, the condition of the patient deteriorated and 7 weeks later she had to be admitted to the clinic again. GOT had increased to 900, GPT to 1900, gamma-GT was 120 mu and gamma-globulin 25%. Once more she received intense treatment with corticosteroids and immunosuppressives, which normalized the test results within a month. Another month later she came to me, because she was told that she had to expect these episodes for the rest of her life. I treated her with injections to the right abdominal sympathetic chain, in the epigastrium, and the pelvis. As I found out later, she had discontinued all the medication on her own. After 3 months and 12 treatments, the diagnosis of the control puncture was not aggressive hepatitis but merely persistent chronic hepatitis. The laboratory results did not give any indication for an impending episode and Ultralan and Imurek were officially discontinued. The central clinic of the LVA Oberbayern (insurance company) concludes from the final examination: “Due to the initially adverse progression of the hepatitis, an immunosuppressive therapy was decided on, which was discontinued in March of 1976. In the course of the healing process, repeated examinations did not show any indications of humoral activity. Antibodies that indicate chronic hepatitis were not detected. There was a confirmation of Australia antigen antibodies. This leads to the conclusion that hepatitis B was present during the past year. The condition appears to be cured.” Follow-up period of 8 years: no relapse, all regular control examinations showed normal results. Ever since and without missing work, Mrs. K. has done piecework 8 hours a day for the metal industry. Pancreatic disorders In addition to the well-known dyspeptic disorders, there is pain in the left upper abdominal quadrant, which radiates towards the heart and left kidney. Occasionally, there is also a boring pain in the xiphoid angle, which can extend as far as the area between the shoulder blades, and fibrositic nodules may form in the left trapezius muscle. The corresponding Head’s zone is centered at the left of T8. Apart from giving a fermentation substitute and the injections listed under → abdomen, we also inject to the → (T) sympathetic chain, especially on the left but occasionally also on the right, since the stomach and duodenum are inevitably co-involved. In acute pancreatitis, → (T) intravenous procaine injections have proved effective, together with segmental treatment of the hyperalgetic tissues; also → (T) paravertebral anesthesia to T8 to T10 left and injections to the → (T) sympathetic chain at the left upper renal pole. If this proves inadequate, the lumbar → (T) sympathetic chain should also be injected when the treatment is repeated. Makocha treated 119 patients with acute pancreatitis by administering procaine injections bilaterally to the upper renal poles. He described these as a “lumbo-retroperitoneal Novocaine block” (150 mL of 0.25% Novocaine solution). With this, he gave 500 000 units Monomycin and 10 000 units Trasylol, after having ascertained that there would be no allergic reaction. In 84% of these patients, the pain improved within 20–30 minutes following the procaine injection and vomiting stopped. An emergency operation was indicated only if this conservative form of treatment failed to produce a response within 6–12 hours. In the normal course of events, patients could be discharged from hospital within 10–12 days. Peptic ulcers As far as we are concerned, peptic ulcers are merely another symptomatic form of → neurovegetative dystonia. Excessive physical, chemical, bacterial, mechanical, mental, or other forms of irritation can lead to changes in the neurovegetative system. The next irritative stimulus that can no longer be absorbed by the regulating mechanisms then acts as Speransky’s trigger factor and will lead to “neurocirculatory dystonia” and thus to organic damage. Which organ will be damaged depends on the exogenous noxious stimuli and on the hereditary or acquired point of least resistance. Depending on the circumstances, we shall be able to produce a response from the disturbed autonomic system either by neural therapy or by psychotherapy. This is of far more primary importance to us than knowing whether the patient is hypoacid or hyperacid. Hydrochloric acid can be produced only by involvement of the nervous system, and this is precisely what we have to try and restore to normality. The regulating effect of procaine on the autonomic controls that govern the secretion of the gastric juices is demonstrated by the fact that normal mean values are quickly restored to the extent that this is still anatomically possible, irrespective of whether the patient is hypoacid or hyperacid at the start. Due to our success with gastric ulcers, it seems that our injections have a considerable damaging impact on the environment for the Helicobacter pylori bacterium. See → appendicitis. Dumping syndrome In the case of dumping syndrome, after two-thirds of the stomach secretion, the emptying of the stomach causes overdistension of the efferent intestinal loop and a pull on the mesentery. The vagal stimulus causes the secretion of vaso-active substances, such as serotonin and kallikrein. We can often help in the elimination of these functional disturbances. Fig. 2.1 Segmental therapy in disorders of the liver and gallbladder, anterior aspect. Segmental Therapy in Abdominal Disorders 1. → (T) Intravenous procaine injections have a reversant, analgesic, anti-allergic, vasodilator effect. At the same time they also reduce the permeability of the vascular walls. In the intestine and the biliary ducts, procaine has proved to have a musculotropic and spasmolytic action, which manifests itself especially clearly when there is a high initial tonicity of the vagus. On the other hand, intestinal function can also be restored in hypotonicity, e.g., in post-operative atony (Zipf). The action of these local anesthetics on the nerve centers is so extensive that a gastric ulcer will often heal completely without dieting or bed rest after treatment with a series of about 10 intravenous injections given once or twice weekly. Fig. 2.2 Segmental therapy in disorders of liver and gallbladder, posterior aspect. 2. → (T) Quaddles with a neural-therapeutic product over the epigastrium, gallbladder, or pancreas, i.e., over the painful organ and in the associated Head’s zones on the back and shoulders. We need to remember that the reflex zones of the abdominal organs extend into the dorsal area. For example, pain in the case of a gallbladder ailment can be removed by setting quaddles in the dermatomes C3 and C4, T6 through T10. This disables the corresponding segmental nociceptors in the skin. In the case of non-specific intestinal disorders and disorders of the abdominal cavity that cannot be clarified with regular diagnostics, we palpate the abdominal wall carefully and place the quaddles over the affected areas indicated by the patient as being pressure-sensitive. After that, we proceed with → (T) preperitoneal infiltration. These injections should be given at about weekly intervals until the symptoms disappear. In addition, in such cases it is always desirable to restore the intestinal flora by supportive treatment with drugs and diet. In acupuncture, there is a “key point of the stomach” (BL-21), which is used for all gastric disorders including pylorospasm, hiccoughs, and gastric colics. It lies between the lateral processes of T12 and LI, two fingers’ breadths from the dorsal median line and is set bilaterally. We place a quaddle over both points and then penetrate through the quaddles to infiltrate to a depth of a few millimeters. → (T) Scars in these referral areas need to be given special attention. One to three (painful!) quaddles with double-distilled water into the areas of maximum pain cause colics to disappear at once, whilst pain due to inflammation will persist. This is especially useful in providing a differential diagnosis between colic pains and an “acute abdomen.” 3. Injections → (T) preperitoneal into the → (T) epigastrium. 4. An injection into the → (T) nerve-exit point of the right → (T) supraorbital nerve is also recommended in all liver and gallbladder disorders, especially if it is pressure-sensitive, as will be the case in about a third of all right-sided abdominal disorders. Procaine injected to this point can often stop a biliary colic. The corresponding point on the left more rarely plays a similar part in gastric disorders. Fig. 2.3 Segmental therapy in gastric disorders, anterior aspect. 5. If we find deeper-seated hyperalgetic points when palpating the patient, e.g., in the musculature of the spine, we first set an intracutaneous → (T) quaddle over the site and probe through this in depth until he or she indicates a sharp pain. At this point we then infiltrate a small quantity of procaine intramuscularly (→ (T) intramuscular infiltrations). If the vertebrae themselves are sensitive to pressure or tapping, we inject to the periosteum. In gastric disorders, Vogler, with his periosteal massage, found that there is a palpable dip in the periosteum on the left costal arch (lying approximately on the nipple line), and that, by massaging this, it is possible to cure gastric ulcers. For the gallbladder, this hyperalgetic point (indicating a hyperalgetic change in the periosteum) is often found on the right costal arch. We make use of these observations and inject the local anesthetic into these sites to obtain the same results as with Vogler massage, but more easily. 6. The most elegant treatment for biliary colic is by → (T) paravertebral anesthesia of the right intercostal nerves from T9 through T11. For gastric colic, the corresponding intercostal nerves are those on the left from T6 through T8. Intercostal anesthesia to T5 through T11 is also the best way to relieve post-operative pain after abdominal surgery. It prevents a lowering of the patient’s vital capacity and of his or her arterial oxygen level far better than giving him or her analgesics, and cuts down the risk of pneumonia and atelectases. 7. In any segmental abdominal disorders, including chronic constipation, the injection to the splanchnic nerve and the celiac plexus and its → (T) ganglia on the affected side (e.g., on the left in mucous or ulcerative colitis) or alternately left and right has proved to be particularly effective. It improves the blood flow to the liver and choleresis, which in turn, lowers the bilirubin level. 8. From acupuncture we have also learned to give our attention to the inner aspect of the thigh, at the dorsal edge of the sartorius, to set → (T) quaddles there and to penetrate through these to a depth of 40– 80 mm. Fig. 2.4 Segmental therapy in gastric disorders, posterior aspect Every one of the injections given under (1) to (8) can help on its own, but we generally combine two or more, depending on the circumstances. In chronic abdominal disorders we can hardly ever avoid resorting to some sort of polypragmatism. In addition to the injection to the abdominal → (T) celiac plexus, → (T) epigastrium, a series of → (T) quaddles on the upper abdomen—a few of these down to the peritoneum—we also like to go into the points found by Vogler on the periosteum of the lowest rib. All this should be done at a single session. Some neural therapists inject the right abdominal and left lumbar sympathetic chains together in one session and change sides the next time, top right and bottom left. F. Huneke almost always injected only the right abdominal sympathetic chain, with no more than 2 mL Impletol. As a rule this is enough if the needle is in the right place. As always, if there is a recurrence of the disorder, these injections have to be repeated. Experience shows that the effect increases on repetition. By means of these injections we can generally cure or at least greatly improve any segmentally caused abdominal disorders, which could otherwise be improved or cured only by local medical or surgical means. These generally involve greater risk and take longer. Bed rest and other measures apart from these injections have only a supporting role to play in neural therapy. Even severe gastric hemorrhages can, as a rule, be controlled by repeated procaine injections to the → (T) sympathetic chain, intravenously (→ (T) intravenous procaine injections), into the → (T) epigastrium, and into Head’s zones. Mortality from operative treatment of hematemasis has always been greater than from conservative treatment. In indurated gastric ulcers (and to relieve pain in gastric cancer), Bricis used a fiber-optics gastroscope to help him inject a 1% procaine solution into the pylorus and into three or four sites around the ulcer or tumor. This resulted in cures of 89.6% of all ulcer cases, 60% of them being cured in 2– 3 weeks! Daily practice has taught us that there is an “abdominal area interference field” that can turn into the source of pathogenic impulses and misinformation for regions outside of itself. This field forms following abdominal surgeries and inflammations of all sorts, for example, hepatitis, pancreatitis, amebic dysentery, or as a result of → dystrophy (protein deficiency) in prison camps or famine-stricken areas. In these cases, our splanchnic and celiac anesthesia (celiac plexus) are also able to clarify the situation and remove remote disturbances. The “nervous stomach,” which does not respond to the → (T) intravenous injection or to an injection into the → (T) epigastrium is, as far as we are concerned, quite often merely one of the guises of what is known as → neurovegetative dystonia. In these cases, a series of injections, for example, into the → (T) thyroid, can often produce rapid relief and enable other links to be more clearly recognized. In the case of ulcers, the frequent interference field caused by chronic appendicitis needs to be remembered! In infants and toddlers who suffer from pylorospasm, dyspepsia, intestinal spasms in the umbilical region, and such, the → (T) scar of the navel can be the interference field. Abdominal glands tuberculosis of: → tuberculous peritonitis. Abdominal surgery post-operative pain following: → adhesions, → post-operative pain. Abortion (threatened, habitual, febrile): Only 70% of all inseminated eggs result in a healthy birth. Within the first 4 months of the pregnancy, 25% of the 30% miscarriages are due to defects in chromosome structure, which is often not even recognized as an abortion. The remaining miscarriages are caused by exogenous, endogenous, psychogenous, or immunobiological factors. The hormonal changes and stresses due to pregnancy can cause adaptive difficulties and dysregulation in balancing the hormonal output and the neurovegetative excitatory level (pituitary, ovarian, and thyroid hormones). Hormonal disorders of the ovaries and thyroid, whether they result from hypofunction or hyperactivity, may produce psychic or somatic states of tension and lead to miscarriages. Neural therapy can help restore equilibrium, irrespective of the initial autonomic condition, produce eutonia of the uterus and vascular system, and induce the necessary mental relaxation. We can, in this way, provide a harmless alternative to the risky use of hormones in early pregnancy. The German Society for Endocrinology has issued warnings against the use of estrogens and gestagens in cases of threatened or habitual abortion. In girls whose mothers were treated with Stilbestrol in early pregnancy, a high incidence of vaginal cancer was found to occur, with a correspondingly high incidence of testicular disturbances in boys (Jung). Here are the treatments for three types of abortion: 1. Febrile abortion. Becke administers 1 mL of procaine intravenously and infiltrates the → (T) pelvic region and → the (T) Frankenhauser’s plexus before dilatation and curettage. He rejects the administration of sulfonamides and antibiotics, since these would merely produce free endotoxins. Under procaine cover, the patients are afebrile within a few hours, they feel much better, and renal function remains intact. If required, the injections are repeated after 4–5 hours. This will prevent the occurrence of the ShwartzmanSanarelli phenomenon (Huebschen). 2. Habitual abortion. Treatment before and during pregnancy: → pelvis. The uterus of women who are subject to autonomic hyperexcitation may be ready for labor during the entire period of the pregnancy. For this reason, Mink also recommends neural-therapeutic injections into the → (T) thyroid at about weekly intervals until the sixth month of pregnancy, in order to relax the autonomic nervous system. I first published this observation in 1960. Twenty years passed before a clinician checked and was able to confirm my statement. Zahn uses the injection into the thyroid in premature labor from the 20th week of pregnancy, “if the conventional use of beta sympathomimetics and prostaglandin inhibitors is not enough to inhibit labor.” Slender women with a nervous constitution and with or without a slightly enlarged thyroid are particularly grateful patients for this method. 3. Threatened abortion: In addition to the usual measures, segmental treatment will help to reduce the irritability of the uterine musculature: → pelvis. The depolarizing processes that occur in the cell membranes of the myometrium, which can cause premature and excessive labor pains because of raised tonicity, can thus be reversed. But since anxiety and the fear of abortion will increase the tone of the pregnant uterus, neural-therapeutic injections are also given into the → (T) thyroid, in order to achieve emotional and autonomic relaxation. Abscess Inject around and under the abscess, if possible as soon as it starts. The → inflammation will then rapidly resolve and the abscess will heal. The question is still contested whether local anesthesia may be administered in the inflamed area around an abscess that has softened and needs to be incised. Killian regards this as wrong and recommends the use of a nerve block (conduction anesthesia) away from the site of inflammation. Eriksson takes the view that “the injection of a very small quantity of a local anesthetic by means of a fine needle over the point of the abscess is not only without risk but is often the simplest and best form of anesthetic.” Achalasia Cardiospasm due to disturbed innervation of the mesenteric plexus, hence of the opening function of the distal esophagus. Therapy upper abdominal → (T) celiac ganglion bilaterally, → (T) epigastrium, → (T) quaddles to abdomen, lower sternum, and back (T7–9 left). Due to disorders of the esophagus, peristaltic injections to the → (T) stellate ganglion. See → abdomen. Achillodynia, Achillotendinitis The areas around the pressure-sensitive, painful parts of the Achilles tendon are infiltrated and injected with a thin cannula. A firm bandage is applied → tendovaginitis. A partial or complete tear of the Achilles tendon requires surgery! Acne → skin. Acrocyanosis → neurocirculatory disturbances, → carpal tunnel syndrome. Acrodermatitis → skin, → neurocirculatory disturbances. Acromelalgia → erythromelalgia. Acroparesthesia → neurocirculatory disturbances, → carpal tunnel syndrome. Adhesions Post-operative adhesions following appendectomy, cholecystectomy, gastric surgery, gynecological operations etc., are relatively rare and are probably diagnosed far more often than they actually occur. When a disorder persists or recurs after technically perfect surgery, this means all too often that local surgical intervention in the segment was not indicated at all, since an interference field somewhere totally different was in fact responsible for the disturbance at the remote site concerned. Obviously, further surgery at the same site cannot cure such complaints, said to be “due to adhesions”; these can be cured only by removing the cause via a lightning reaction: → post-operative pain. Adhesions following abdominal surgery are formed because of bacterial or abacterial fibrinous inflammation of the peritoneum when it has been allowed to become dry, or of mechanical, thermal, bacterial, or chemical irritation during surgery. Some people seem to have a tendency to develop adhesions, and there is doubtless a difference in the predisposition as between different individuals in their sensitivity to adhesions and the degree to which they suffer from them. Severe adhesion symptoms may occur with no adhesions present, whilst in other cases quite severe adhesions may be present without producing any symptoms. Siegen has shown that procaine can reverse the pre-morbid stasis in the terminal capillary network (Ricker), which causes exudation of fibrin due to irritation of the peritoneum. For this purpose, it does not matter whether procaine is given locally, or by intravascular, perivascular, or periganglionic injections. When fibrinous adhesions are present, the pain will disappear, the signs of inflammation regress, and the prestasis will change to fibrinolytic hyperemia, which assists the healing process, always provided that this happens before the fibrinous layers have changed into avascular, shrinking scar tissue, which will be much less responsive. Through the early use of procaine treatment in new surgery scars and possibly through the use of → (T) preperitoneal infiltration, we see the chance not only to prevent the formation of interference fields but also keloids and adhesions. When post-operative symptoms are present, we first infiltrate the → (T) scar and through this down to the peritoneum. Or we set a → (T) quaddle in the area of the dermatome that the patient indicates as being painful or tender and then probe in depth for the painful point, which may be extremely localized, on the parietal peritoneum, and treat it with → (T) preperitoneal infiltration. After several such injections into the painful segment, we can often feel the regression of deep adhesions and cords, even if they have been present for prolonged periods. The patient feels the reactive hyperemia following the injection as a pleasant warmth. Occasionally there may be a transient increase of pain, but this will normally disappear after a day or two and yield to a noticeable improvement in the abdomen or even in the whole of the body. If this should not suffice, segmental therapy will often produce the required result, with injections to the splanchnic nerves (abdominal → (T) celiac ganglion) or the → (T) pelvic region or → (T) Frankenhauser’s ganglia. If our efforts in the segment prove ineffective, we must test every possible interference field before considering further surgery! Adipositas dolorosa, adiposity → obesity. Adnexitis → pelvis. Adrenal insufficiency injections to the splanchnic nerves (→ (T) celiac ganglion) at the upper renal pole. See → (joints) → rheumatism → hormonal disturbances. Aerophagy It is frequently based on autonomic dysregulation. Treatment alternating injections to the→ (T) stellate ganglion, → (T) celiac ganglion (see p.173) and the → (T) epigastrium. Air embolism Immediate injection of procaine intravenously (→ (T) intravenous procaine injections) and to the → (T) stellate ganglion, → vascular occlusion. Alcoholism Alcoholism is one of the most important sociomedical and sociopolitical problems of our time. In our environment, 200 out of 10 000 people live with a serious alcohol problem. We do not have enough money and properly trained care takers to look after people with this disorder. According to my own observations, psychiatry (regardless of the method applied) fails to produce satisfying results. B. Dietz found a way to offer successful outpatient care with neural therapy. The treatment is safe, inexpensive, and requires little time investment. Dietz combined → (T) intravenous and → (T) thyroid injections that have a relaxing and reversing effect on the autonomic system. This also decreases the neuro and psychovegetative side-effects of detoxification. In the course of 4 years, 52 patients (nine of them women) received outpatient treatment. The patients were between 20 and 54 years of age and their alcohol habits had lasted between 2 and 20 years. They all expressed the desire to end their alcohol consumption but were not willing to be hospitalized. The psychological guidance by a physician who has experience with the injection techniques is mandatory. Treatment took place once a week. A conscious effort was made to suggest to the patients that this helps to break the compulsive habit, calms them, and strengthens their willpower. Tranquilizing drugs such as diazepam (Valium) and chlormethiazol were given only when symptoms of incipient delirium were present. In this situation, procaine was injected into the thyroid every other day. Within a few weeks, the autonomic symptoms receded in all patients: first insomnia, followed by tremor, and finally hyperhidrosis. The psychological lability lasted for several months. In-patient treatment takes generally 4 months. This period served as the rule and 4 months of sobriety was required. Thirty-two patients reached this goal (61.5%). This result is comparable to the results of common treatment at a specialized psychiatric institution. Now, 10 patients have been “dry” for 1 year, eight patients for more than 2 years. Fifteen had at least one relapse. After verbal encouragement, the treatment started all over again once a week. If the patients felt strong enough to go without injections, the injection intervals were extended. Thirteen patients had been institutionalized once or twice before without success (25%). Of the 20 patients who were unable to achieve the required 4 abstinent months, 12 relapsed after 1 to 15 months, eight were unable to be abstinent, and 10 discontinued treatment. There were no complications due to the treatment. Allergies Allergy means to “work differently” or in this specific case to “respond incorrectly.” Allergens are a dime a dozen. They are only able to cause an allergic reaction if the regulation ability of the organism is compromised through excessive amounts of chemicals or other first insults. This allows for a sensitization to allergens. We have to try to remove the first insult from the organism’s memory at the location of the stimulation. This enables us to normalize the responses of the regulating system and the allergens no longer have an effect on the organism. The daily practice of neural therapy shows proof that this is possible. There is experimental proof for the antihistamine effect of procaine. The first phase of sensitization is in the main specifically humoral in character, though the autonomic nervous system is also involved. But the “allergic reaction” itself is without doubt largely governed by the nervous system, and the disturbance in the neurovegetative system can be reversed by a neural-therapeutic thrust into the system at the correct point. H. Siegen has demonstrated this in extremely instructive animal experiments. He injected rabbits intracutaneously with 0.5 mL of a filtrate of certain bacterial strains (E. coli). The result was merely a transient local reaction. An injection of the same filtrate given 24 hours later into the auricular vein produced a violent response at the site of the primary injection, followed by necrosis. Within a few hours whole sections of skin and subcutaneous tissue were sloughed off (Shwartzman-Sanarelli phenomenon). Hirsch, Keil, Muschaweck, Rade-macher, and Siegen demonstrated that this deleterious allergic tissue shock can be prevented by infiltration of the primary injection site with procaine, even if this is done only a few seconds before the second intravenous injection of the filtrate, which would normally produce the shock reaction. This complete blocking of any allergic reaction in animal experiments is not possible with any other method and seems to prove that the true trigger factor causing allergic shock does not rely on an antigen–antibody reaction but that, in this case, processes are at work that are controlled by the nervous system and that we can regulate by injecting a repolarizing substance such as procaine. Treatment In patients with allergies, particularly if diagnosed with paragroup allergy, conjunctiva and intracutaneous tests have to be done (mainly for liability reasons) before every procaine treatment. This precaution rules out (extremely rare!) procaine intolerance. If both tests are clearly positive, lidocaine (Xylocaine), prilocaine (Xylonest), or mepivacaine (Scandicaine) have to be used instead. Enclosed in ampuls, these substances could also contain preservatives with a paragroup. Ampoules with these additives need to be avoided or pre-testing should be done (see Chapter 5, Part III on procaine hypersensitivity). For immediate relief and a reversant effect, → (T) intravenous injections are given. For serum exanthema, the site of the serum injection and the adjacent musculature should be infiltrated (→ (T) intramuscular infiltration). Injections to the → (T) sympathetic chain and the → (T) ganglia are particularly effective. In chronic cases, search for the interference field, → asthma, → skin, → nose (hay fever). See also Case History 10, Part I, Section C, Chapter 2. In the section on the teeth as an interference field in Part I, a case of trigeminal neuralgia is reported as an “alcohol allergy.” In this, correction of a false bite eliminated not only the neuralgia but also the abnormal reactive state of the patient that had produced the symptoms of an “allergy.” Hormonal allergy → mastodynia, food allergy: → colitis. Alopecia (alopecia areata et diffusa) The loss of hair is often a sign of a secondary disorder or an accessory symptom of some other disease. The point of departure is frequently provided by a detailed case history. There can be little doubt that there are also hereditary, racial, and hormonal factors that play their part in baldness, but the fact that father and son are bald is not in itself proof of a hereditary disorder. Practice shows that loss of hair is in most cases caused by an interference field. Why should not a tendency to tonsillitis or dental granuloma be due to hereditary factors? Why then should not the scalp be affected, if only secondarily but all the more easily, if it represents a point of maximum reaction? We know of families where a weak stomach, an easily irritated gallbladder, or migraine occurs remarkably frequently, not as a hereditary disorder but due to a hereditary organic weakness. An attempt to treat this condition is always justified. Age plays no part in the decision. The results obtained by Dr. Aslan showed that elderly people treated with procaine often grew new hair, and dark hair at that! We know that one of the products into which procaine breaks down is p-aminobenzoic acid and that this acts as a substance that promotes hair growth and contains a factor that prevents hair turning gray. Aslan demonstrated that unsplit procaine is even more effective in this sense. The treatment demands patience and endurance and should start at the beginning of the disease Therapy Procaine injections about once a week intravenously (→ (T) intravenous procaine injections) and under the affected scalp and, in the event of total baldness, the injections should be distributed over the whole of the head. They may be supplemented by injections into the → (T) stellate ganglion. If the thyroid is enlarged or where hyperfunction is suspected, try injections into the → (T) thyroid. A few treatments can stop the increased hair loss that is caused by stress-based nervousness and shows signs of autonomic hyperexcitability. If these fail to produce results, find the interference field. In searching for this, the tonsils, paranasal sinuses, and teeth should always be regarded as prime suspects. An intelligent patient can state, by comparing the effects of various test injections, when the correct site has been found. Amaurosis → blindness. Amenorrhea If of diencephalic or pituitary origin, → (T) intravenous injections, in addition to injections under the → (T) scalp, into the adenoids (→ (T) pharyngeal tonsil) and the → (T) stellate ganglion. All other types: → pelvis. Amenorrhea may also be due to hypofunction of the → thyroid. Amputation-stump pains Injections into the → (T) scar and the site of the former drain. If these do not suffice, try further injections to the bone stump and especially into the nerve stumps. For this treatment, an assistant must fix the amputation stump. In arm amputations, also inject the homolateral → (T) stellate ganglion and the brachial plexus (→ (T) nerves [afferent]) and into the → (T) subclavian or brachial artery. The intra- and para-arterial injections produce a pleasant sense of warmth in the patient. In leg amputations, also inject to the lumbar → (T) sympathetic chain or into the → (T) sciatic plexus and into and around the → (T) femoral artery and the → (T) femoral nerve laterally of this (see Fig. 3.17). If segmental treatment fails, the search for an interference field may produce the culprit: it is perfectly possible that the pain will disappear after an injection into the → (T) tonsils or into a scar, though it could not be influenced from the segment. In such cases, the amputation has had a trigger effect and has allowed a latent interference field to manifest itself. See → phantom-limb pains. Amyotrophic lateral sclerosis → lateral sclerosis, amyotrophic. Anal disorders Includes anal eczema, cracks, fissures, and itching, proctitis, deep-seated lumbago. Treatment with intracutaneous and subcutaneous injections of a local anesthetic is painful but extremely effective. Before injection, the external sphincter should be palpated thoroughly with the well-lubricated forefinger. Old cracks, fissures, and internal or external hemorrhoids can show as locally circumscribed painful or tender areas when pressed or stretched. Only these points are then located and anesthetized with a fine needle to a depth of 20– 30 mm. The treatment is repeated if there is a recurrence of the complaint. If the condition has persisted for some time, several treatment sessions will be necessary, and treatment should not be stopped too soon! In fresh fissures, dilate the sphincter under light anesthesia and infiltrate with a very fine needle under the fissures. If necessary, injections to the → pudendal nerve or → (T) epidural anesthesia and infiltration of the region around the tip of the coccyx (ganglion impar) may also be necessary. Anaphylactic shock → shock, → allergies, → Table 3.2, Chapter 6, Part III. Anemia → blood picture changes. Angiitis obliterans → neurocirculatory disturbances. Angina pectoris → heart, → migraine, cervical. Angioneurosis → neurocirculatory disturbances Angioneurotic edema This disorder is of vasomotor origin. First try a few → (T) intravenous injections. If these are ineffective, inject the → (T) stellate ganglion. If after several treatments the disorder is not cured, find the interference field. See → edema, → mastodynia (in hormonal allergy). Angiospastic dysbasia → neurocirculatory disturbances, → sciatica (post-sciatic circulatory disturbances). Ankle edema → edema. Anorgasmy Preperitoneal infiltrations of l mL procaine or lidocaine bilaterally halfway between symphysis and upper anterior iliac spine (Mink). See →, gynecological dysfunction, autonomic, → sexual disturbances, → (T) femoral artery, → (T) pudendal nerve. Anosmia → nose. Anoxia, anoxemia (e.g., CO poisoning): 1 mL procaine or equivalent intravenously (→ (T) intravenous procaine injections) and injections to the → (T) carotid artery every half-hour, in life-threatening emergencies carefully at shorter intervals. Anterior tibial compartment syndrome The tibialis anterior muscle can swell after overexertion (“march gangrene”) and compress the anterior tibial artery in the narrow anterior tibialis compartment. The acute arterial circulation disorder causes intense pain, ischemia, edema, and necroses, which increase the pain. An induration of the muscle tissue takes place and the deep peroneal nerve suffers a secondary paralysis. The symptoms are: pain in the area of the lower leg extensors and the top of the foot, redness, swelling, and hypoesthesia of the first and second toe. Therapy Infiltration at the back of the knee and the painful areas. Injections in and to the tibial, femoral, and anterior tibial → (T) artery, which travels distally on the anterior crural interosseal membrane (between the tibialis anterior and the extensor digitorum muscles). See also → vascular occlusion, → edema. Anuria, anuresis In addition to → (T) intravenous injections, also inject 2–5 mL of procaine to the abdominal → (T) celiac ganglion. The constriction of the glomerular vessels that causes anuria is relaxed. If a calculus is causing the constriction, the mucosal swelling will regress. See also → kidneys, → eclampsia (in eclamptic anuria), → urine, retention of. Anxiety, state of: Try injections intravenously (→ (T) intravenous procaine injections) and into the → (T) thyroid. Aorta Treatment as → heart. As a rule, syphilitic aortitis responds very well to standard treatment with l mL procaine intravenously (→ (T) intravenous procaine injections) and a few → (T) quaddles bilaterally of the edges of the sternum. The scar, of course, remains but the accompanying inflammation causing the painful symptoms heals. Aphasia → stroke. Apoplexy → stroke. Appendicitis Inflammation of the vermiform appendix is due to changes in the terminal capillary vessels of the appendix, for which the stimulus generally lies outside the appendix itself. In our view, therefore, appendicitis is merely another locally circumscribed partial manifestation of a pathological disturbance of the whole of the autonomic system. According to statistics, the percentage of patients who undergo appendectomy in Germany is three times greater than in the United States, and twice that of Sweden and Great Britain. This suggests very different attitudes from country to country as to when surgery is indicated. If reports are to be believed, Chinese traditional medicine successfully treats even an acute appendix by acupuncture and the oral administration of a plant extract. In normal circumstances, when a patient presents with an acute appendix or when one cannot be absolutely certain that he or she is not suffering from acute appendicitis, one ought to leave the surgeon to deal with it and refrain from using neural therapy for diagnosis or treatment. But I must nevertheless refer to the potential of our therapy, for the sake of comprehensiveness and for use in exceptional circumstances when lives could be saved, for example, at sea, during expeditions, in remote ski lodges, and such. Neural therapists always carry disposable syringes, cannulas, and procaine because, in emergency situations, it frequently proves to be extremely valuable. Therapy In chronic and subacute appendicitis, we inject into the right abdominal → (T) celiac plexus and set one to three → (T) quaddles over McBurney’s point, passing through these whilst slowly infiltrating from 1–2 mL procaine down to the peritoneum. In such cases, the peritoneum is always irritated and painful. In addition, we also set a quaddle to the right and left of the appendix point known to acupuncture. This is inferior to the knee on the anterior tibial muscle, about two to three fingers’ breadths caudally from the angle formed by tibia and fibula (Bischko). This point is then always clearly palpable as a hyperalgetic point and is a useful diagnostic indicator. It is more accurate to locate this point with an instrument that measures skin resistance and set a quaddle exactly to the right and left of the point. After that, each quaddle should be infiltrated to a depth of 0.5–1 cm. In the hands of an experienced neural therapist, this method, in combination with fasting and colonic irrigation, has proved effective in patients who refused surgery and especially in appendicitis in the elderly, where the prognosis is so often unfavorable. A warning must, however, be given here against random injections by the inexperienced and the irresponsible. Our injections support the self-healing process. In a chronic or subacute appendicitis, we can cause the inflammation to regress. But if there is a suppurative focus with incipient necrotic softening already present, a spontaneous cure would consist in perforation of the appendix. We have to consider, therefore, how long we may continue with conservative treatment and when, particularly in the acute stage, we must refer the patient to the surgeon. The following rule of thumb applies: wherever the application of heat is contraindicated (acute appendicitis, gallbladder empyema), we refrain from segmental treatment. Chronically recurrent appendicitis occasionally proves to be an interference field for other disorders. Tests for this are made at McBurney’s point as described above. If this produces a lightning reaction in accordance with the rules, we ask a surgeon to remove the interference field (see Case History 11, Part I, Section C, Chapter 2). Bykow and Kurzin have pointed out the intimate link between gastric ulcer and appendix, and this is significant for us: “According to the results obtained by I. I. Grekov in 1923, appendicitis was found in all the cases of gastric ulcer seen” (Bykow, Kurzin). We might add: “or an appendectomy scar acting as an interference field.” This tells us that whenever we are presented with a gastric ulcer, the region of the appendix and the appendectomy scar should always be tested at the same time. Arm pain → neuralgia, → neurocirculatory disturbances, → phantom-limb pain, → scalene syndrome. Arrhythmia, cardiac → heart. During pre-operative preparation, the administration of a prophylactic dose of 1 mL procaine solution intravenously has proved extremely valuable in preventing the risk of cardiac arrhythmia! Arteriosclerosis The salts of p-aminobenzoic acid, one of the two breakdown products of procaine, can help to dissolve certain compounds that are normally difficult to dissolve, including cholesterol. This may help to explain the beneficial effect of procaine in the treatment of→ geriatric disorders. We also know that procaine given intravenously (→ (T) intravenous procaine injections) increases capillary wall impermeability and dilates the blood vessels. Arteritis, temporal Characteristic symptoms are severe headaches in the evening and at night, accompanied by fever, debility, and visual disturbances. The temporal arteries are thickened unilaterally or bilaterally, and the skin over them is discolored bluish-red and swollen. Treatment Usually, careful infiltration of procaine is beneficial, possibly injection to the stellate ganglion. In the head and neck region, hasty injection of large amounts and with great pressure has to be avoided at all times! The superficial temporal → (T) artery is merely a marginal branch of the carotid artery. However, large amounts that are injected with great pressure can end up in the carotid system due to a backlog in the vessel. This can result in complications, which is also the case with the facial and occipital artery. Arthralgia, arthritis, arthropathy (acute or chronic; of rheumatic, infectious or of other origin): → joints. Arthrosis of the shoulder → joints. Articular rheumatism → rheumatism. Ascites If due to cardiac insufficiency: → heart. In cirrhosis of the liver, try injections to the abdominal → (T) celiac ganglion. Asthma, bronchial → lungs. Asthma, cardiac → heart. Athlete’s foot → mycosis, → skin. Atony, intestinal → intestinal atony. Atrophic rhinitis → nose. Atrophy due to disuse → disuse atrophy. Autologuous blood → Derived from organism of the same individual. Auriculotemporal nerve → neuralgia. Autonomic dysregulation → neurovegetative dystonia. Autonomic gynecological dysfunction → gynecological dysfunction, autonomic. Backache → (Baastrup’s) kissing spine syndrome, → lumbago, → spondylolisthesis. According to Martius, backache in women is a “universal gynecological symptom.” In disorders of the pubic region we often find a painful dorsal zone above the upper sacrum, with pain extending as far as the area of the dorsal iliac crest. Painful adnexitis can radiate into the area of the dorsal iliac crest. Symptoms that are detected through palpation, such as pain on moving the cervix, or pressure sensitivity of the posterior symphysis and lateral pelvic wall, are not necessarily caused by inflammation. More likely they are the result of autonomic dysregulation (→ gynecological dysfunction, autonomic) with circulatory problems and hyperalgesia. In this case, the uterosacral ligaments can also be contracted and cause backache (pelvic congestion). We can practically guarantee that we can relieve backache of pelvic origin at once by an injection into the → (T) pelvic region and by this means solve the problem quickly and permanently. Not every pain in the back needs to be a spondylosis or even damage to an → intervertebral disk, despite the fact that an x-ray, that snapshot recording a single moment of the living organism, may permit such a diagnostic interpretation. Only the function matters, and far more important than any diagnosis with the fatal rider “incurable” is the cure that we can generally provide, especially in the case of a backache, irrespective of its origin and cause (except for cancer and advanced tuberculosis), either via the segment or by means of the lightning reaction. For unilateral backache, see → sciatica, → psoas syndrome. Balance, loss of → disequilibrium, → vertigo. Baldness → alopecia. Basedow disease → thyrotoxicosis. Bechterew disease → spondylitis, rheumatoid. Bedwetting → enuresis nocturna. Bell palsy → paralysis, facial. Bing–Horton syndrome → erythroprosopalgia. Bladder, disorders of → cystitis. In urinary incontinence in women, parametrial hypertonus, benign ulceration of the bladder, use procaine injections into the → (T) pelvic region, → (T) Frankenhauser’s ganglia, also intravesically. See also → prostate, → bladder, irritable, posterior → (T) sacral foramina, → (T) presacral infiltration. Bladder, irritable This is generally seen in women about the time of the menopause, usually in conjunction with other autonomic disorders, such as hyperhidrosis, dermographism etc. At night and during the period there are usually no symptoms. In the morning, there is distressing urgency and dysuria with a terminal burning sensation, which can become exacerbated during the day. Sometimes, in addition, there is also relative bladder incontinence. Urinalysis is negative and cystoscopy also yields no result, except for a slightly more prominent vascular pattern in the trigone. When taking the case history, the practitioner has to ask about stressors, gynecologic surgeries, resections of the prostate, hormonal disorders, the intake of psycho-pharmaca, laxatives, spasmolytics, oral contraceptives, etc. All these factors may effect the motility of the muscular portion in the urinary tract. Treatment There is objective proof that the prostate capsule and, in the case of women, the vesicoureteral orifice are sources of afferent noxious stimuli leading to bladder function disorders. The physiological interplay between bladder filling and bladder emptying is disturbed. Through anesthesia of the proper receptors, the function can be normalized. We first try the injections to → (T) Frankenhauser’s ganglia, described in → pelvis, because these affect the hormonal processes. Further, anesthesia of the neck of the bladder may also be useful. For this, we insert a vaginal speculum to visualize the anterior vaginal wall and, using a thin 60 mm-long needle, we insert this about 20 mm behind the urethral opening and infiltrate the loose connective tissue between bladder and vagina fanwise with 3–5 mL. To stop bleeding on the way home, a tampon is inserted in the anterior third of the vagina. Objective proof by urodynamic methods of the success of this para-urethral infiltration has been provided by Spernol and Riss. The neck of the bladder can also be reached by entering from above through the abdominal wall behind the symphysis. To reduce hypertonicity of the sympathetic system and the spasms due to the nervous hyperexcitability of the bladder, injections into the → (T) thyroid may also help. → (T) Quaddles over the bladder and the sacrum as far as L1 are also indicated, priority always being given to hyperalgetic points. In the case of irritable bladder in men: injections to or into the → (T) prostate capsule in addition to the above-mentioned quaddles. → (T) Presacral or → (T) epidural infiltration will be necessary only in stubborn cases. See also → enuresis → kidneys, → cystitis, → (T) sacral foramina. Blindness Transitory or toxic amaurosis, e.g., after the administration of streptomycin or arsenic and following convulsions (→ eclampsia), is treated as follows. For immediate relief and as basic treatment, l mL procaine intravenously (→ (T) intravenous procaine injections) to eliminate the vascular spasms, repeated half-hourly if necessary, plus injections into the stellate or → (T) ciliary ganglion, or injections to (not into!) the→ (T) carotid artery. See also → eye disease. Blood picture changes The sites where blood is formed and their regulating centers are non-autonomous parts of the whole and like any other organ can be inhibited by interference fields from functioning properly. As a result they can become inefficient. Pischinger was the first to provide objective evidence of the Huneke phenomenon by proving that all changes in the blood picture caused by interference fields rapidly return to normal as soon as the interference field is eliminated, since the cause acting as trigger within the basic autonomic system is eliminated at the same time. Fleischhacker also reported on the surprising success of neural therapy according to Huneke in disorders of the myeloid system. Anemia with a reduced serum iron level, which does not respond to the oral administration of iron, is as a rule due to an interference field. Stacher was able to show that erythropoiesis can be inhibited by interference-field influence in aplastic anemia and panmyelopathy. As a rule, a substantial improvement or complete cure is quickly obtained as soon as the interference field has been found and eliminated. Elsewhere, Stacher states that the elimination of the interference field responsible produced normalization of the blood picture in more than 70% of all cases of granulocytopenia of unknown origin. Of 12 cases of panmyelopathy, dental treatment alone produced complete normalization in six of the patients. According to Boehnel, many cases of anemia and leukopenia can be cured by the elimination of interference fields. Some cases of leukemia also respond favorably. When the interference field was eliminated, anti-leukemic therapy became effective although there had been no improvement before. In leukemia, where the spleen is substantially affected by tumor or where it is infarcted etc., splanchnic or → (T) celiac ganglion anesthesia on the left side brings pain relief. Boehnel states “All this again suggests that a focus or an interference field is producing an environmental change that substantially influences the pathological process and the way the disease will respond to therapy.” Stacher reports the following case. When treatment of a panmyelopathy with blood transfusions, corticosteroids etc. had failed to produce results, bone-marrow damage due to an interference field was suspected and it was decided to carry out a focus provocation. In addition to a reaction in two teeth, there was a temporary deterioration in the blood picture. Following extraction of the two teeth, there was at first a substantial temporary drop in the leukocyte count. This was followed by a sharp and excessive rise and finally by a return to a normal blood and bone-marrow picture. This has now persisted over 3 years. After subcutaneous and intramuscular (but less so after intravenous) administration of procaine, Joachimovits found an increase of monocytes, histiocytes, and mast cells, as an expression of its stimulating effect on basic tissue. In acupuncture, point BL-39 is known as the “principal point for erythropoiesis.” It is said that when a needle is inserted at this point there is a rapid increase in the erythrocyte count by as much as a million (Bischko). On account of the risk of collapse, the patient must always be lying down when the needle is inserted. He or she bends his or her back with the shoulders held forward, so that the scapula clears the entry point where the shoulder blade and the upper edge of the fourth rib intersect. The Bucarest Institute for Geriatrics, which propagates Novocaine therapy according to Aslan, found the following improvement in the blood picture to be a regularly repeatable result of this treatment: reduction in the increased leukocyte count, increase in granulocytes and monocytes, increased globulin values. However, one ought not to lose sight of the fact that, generally, after parenteral procaine treatment, the leukocyte count increases by 1000–3000 for 2–3 days. Blood pressure (high) → hypertension. Blood supply, disturbed → neurocirculatory disturbances. Boils → furuncles. Bone fractures → fractures. Brachialgia → neuritis of the brachial plexus. Brain injury → cerebral injury. Brain tumor → cerebral tumor. Breathlessness → heart, → lungs (depending on origin). Bronchial asthma, bronchiectasis, bronchitis → asthma, bronchial, → lungs. Bruises → hematoma, → injuries. Bullous eruptions → skin. Bunion, inflammation of → hallux valgus. Burns Prophylactic measures against → shock by repeated → (T) intravenous injections. These also act to relieve pain, reduce vascular permeability, and help to lower the patient’s temperature. Small areas are infiltrated around and under the burn. In severe cases, we treat shock and the reactive inflammatory symptoms such as → edema, lymphorrhea, and hemoconcentration by injections to the abdominal → (T) celiac ganglion and/or the → (T) stellate ganglion. The healing process is visibly hastened when this treatment is repeated. Bursitis In prepatellar or olecranon bursitis, replace about a fifth of the quantity of fluid removed by paracentesis with physiological saline solution and 1 mL procaine into the bursa. This will at first produce a small irritant effusion, but with hardly any pain. On repetition, a soft pad is formed that assumes the protective function of the mucous bursa. In subdeltoid or subacromial bursitis, insert the needle medially through the deltoid muscle from the center of a line running from the tip of the acromion to the greater tuberosity of the humerus, using a 35 mm-long 0.7 mm diameter needle. If effusion fluid is aspirated, the needle is correctly placed. Aspirate the liquid and inject 1 mL procaine solution. Calcaneal apophysitis Exostosis of the calcaneus at the Achilles tendon attachment with painful swelling of the soft tissue. Therapy Repeated infiltration of the painful tissue every 2–3 days. Calcaneal spur Infiltrate the local hyperalgetic points on both sides of the calcaneus and through them into the vicinity of the calcaneal spur (not through the sole of the foot!). In stubborn cases, inject into the homolateral → (T) sacroiliac joint. If these are not effective, find the interference field. See also → periosteum. Calf, pains in → sciatica. In case of cramp, → (T) quaddles over the center of the calf and injections to a depth of 30–40 mm, and laterally of the tibia over the anterior tibial muscle (→ anterior tibial compartment syndrome). Try → (T) epidural (caudal) anesthesias, → (T) presacral infiltration or injections to and into the → (T) femoral artery. Callus formation, inadequate Normal callus formation depends on a correctly functioning nervous system. Animal experiments have proved that a → fracture heals more quickly if procaine is injected as closely as possible to or into the fracture site. Evidently, the repolarization effected by the procaine eliminates any dysregulation that would delay normal callus formation. An injection into the → (T) afferent arteries and nerves will generally be adequate to normalize the disturbed neural and blood supply. If this fails, injections to the relevant → (T) sympathetic chain and its → (T) ganglia may be necessary. Cancer In English, we speak of cancer. The French, more accurately, use the plural form “les cancers,” to show that a number of similar diseases are grouped under this collective term. Cancer is not curable by neural therapy alone! But the fight against the pain produced by cancer is a grateful field for our form of treatment, which enables us to cut down on opiates and sometimes even to replace them altogether (Krecke). We can reduce every form of → inflammation by means of procaine. We believe that the same means makes it possible to eliminate the inflammatory protective wall with which the organism surrounds any malignant tumor. This surrounding inflammation is reduced by injection to and even into the tumor and the → (T) nerves (afferent) and → (T) afferent arteries, the pain abates, and the tumor not infrequently becomes noticeably smaller, for example, with → ileus. Consequently, the pressure exerted on nerves, and on blood and lymphatic vessels, with its resulting congestion and pain, is eliminated or at least reduced. Unfortunately we are unable to stop the inevitable progress of the disease, but we can at least slow it down and provide relief. Treatment will depend on the site of the tumor. It is given within the relevant segment, in accordance with the usual methods of segmental therapy, i.e., in cancer of the stomach the injections are given into the → (T) celiac ganglion at the upper pole of the kidney and into the → (T) epigastrium; in lower abdominal cancer they will be administered into the → (T) pelvic region and intramurally (→ (T) intramural) into the uterus; in bone metastases to the adjacent periosteum; in inoperable genital carcinoma we treat the patient by → (T) epidural anesthesia etc. On account of the sensitivity of cancer patients to irritative stimuli, Schlitter recommends increasing their resistance by the subcutaneous—probably, better still, intracutaneous—administration of minute quantities of procaine (0.1 mL, 0.5 mL, l mL) into the left dorsal dermatome of the spleen (L6 through L8) and to keep strictly to intervals of 4 weeks between treatments, in order to allow the irritation to abate and prevent it from becoming too intensive by summation. The effect can be shown objectively by an increase in the absolute lymphocyte count and is explained by an immunobiological stimulation of the spleen. The view that the conclusions on interference fields, as taught in neural therapy according to Huneke, have a useful contribution to make to the theory on the causes of cancer and, in particular, to cancer therapy is briefly sketched below. In our era of industrial civilization, science and technology have placed humankind in an unnatural environment, which acts as an overstimulation and thus endangers life. Humankind has to adapt to this whether it likes it or not. If it fails to do so, it becomes liable to the so-called civilization disorders, one of which is cancer. Cancer only manifests itself to us as a local disorder. But there can now be little doubt that it is merely the end result of an illness that affects the whole organism. Cancer begins in a cell with non-specific genetic function, which is not recognized, destroyed, or otherwise eliminated by a weakened immune system. It may have become blocked and reacts too slowly due to organic or psychological interference fields. In our view, an illness occurs only when the entire organism or, more precisely, the basic autonomic system permits it, and this applies to this disease above all others. Cancer, like any other illness, becomes manifest only when the regulating mechanisms, the body’s defensive system and its spontaneous healing powers become overloaded and are blocked by too many and excessive noxious stimuli, which the basic autonomic system can no longer cope with, for which it is no longer able to maintain the supply of the bioelectrical power needed by the many different vital functions in order to operate smoothly. Statistics show that one out of eight smokers and only one out of 220 non-smokers dies of lung cancer. There is no question about the carcinogenic effect of smoking on the lungs. But the mere search for ever more substances that might cause cancer does not help us to solve the problem. We need to find an answer to the question why the other seven smokers do not die and the 220th non-smoker does die of lung cancer. The search for the cause of cancer has to include the question why does a cancer patient respond to smoking the way he or she does? This would inevitably lead to the issue of the cancer-promoting effects of interference fields, which enable risk factors to turn pathogenic. In 1938, at the Robert Koch Institute in Berlin, P. G. Seeger discovered that a disease, including cancer, takes place in a cell only if the enzyme cytochrome c oxidase (cytochrome a3) has lost its tension. Every stimulus causes the electrical cell potential to drop, and the amount and duration of this reduced potential will vary according to the strength and duration of the irritative stimulus causing this reduction. The cell’s electrical potential is maintained at its proper level by normal cellular respiration. Any unphysiological stimulus that is too strong or persists too long causes depolarization or lowers the resting membrane potential over a fairly lengthy period and becomes pathogenic. The cell is thus left unprotected and at risk. Cell metabolism depends on the permeability of the cell membrane. This is selective and varies constantly with the bio-electrical charge in the membrane. The absorption of oxygen is linked to a certain level of this electrical potential. All carcinogenic substances and these other factors inhibit cellular respiration. Consequently, the electrical potential drops further and permeability is further reduced. Once the effect of this interactive process exceeds the limits of tolerance, cell fermentation begins in the anoxic cell and prepares the way for cancer formation. H. Lamers pointed out that the cytochrome c oxidase and procaine share the same redox potential of 290 mV. He also indicated that procaine is able to repolarize and stabilize the enzyme that plays such an important part in the development of cancer. As cellular respiration (and the electrical potential) is reduced even more, the cancer cells become more virulent (Seeger). With progressive lowering of electric potential the cell respiration worsens. It is ultimately no longer monitored by the autonomic control system and absconds from the totality of information. According to this, therefore, the problem of cancer is one of microbiological energy! Cell electrophoresis shows that cancer cells do, in fact, have a reduced membrane potential. Cancer cells migrate faster than normal cells, and the speed of their migration increases as the cell’s electrical potential decreases. Thus, the charge level of the cell membrane of a cancer cell is actually less than that of a healthy cell. Cone, Jr. stated that the constant proliferation of tumor cells could be due to permanent electrical depolarization. In cell cultures, maximum mitosis occurs when the cell-membrane potential drops below –10 mV. When the potential is at –70 mV or more, pathological mitosis does not occur. Measurements made on rapidly dividing myosarcoma cells showed them to have a cell-membrane potential of only –10 mV, whilst that of the neighboring healthy muscle cells with normal mitotic activity was found to be –90 mV. As the cause for the reduced electrical potential of the membrane in malignancy, Cone mentions a basic functional change in the molecular structure and in the specific characteristics of the cell surface, which, in turn, is due to a functional disturbance of the metabolic processes whose task is the synthesis and the stereochemical structure of the cell-surface polymers. These observations confirm in practical terms what has been stated up to this point. This is how matters look from the viewpoint of the cell. But the cell does not exist in isolation; its life is as much for the sake of the entire organism as it is made possible by it. The neurovegetative system links every cell to the same living organism, which it is, in the final analysis, the cell’s sole function to serve. Via the basic autonomic system, the cell receives and sends out its directing and informative impulses. In our view, the cell is the reacting organ of the autonomic fibril. Provided there is an adequate oxygen supply, cell respiration is assured only if the neurovegetative monitoring and control system is intact, and the cell remains safe from cancerous degeneration into destructive autonomy only as long as these conditions are fulfilled. Consequently, cancer therapy has to eliminate the interference fields or the excessive segmental irritative stimuli that are blocking the organ responsible for the transmission of information, namely the neurovegetative system, and to make it capable once again of functioning efficiently. This is the only way in which the blockage, present in every tumor patient, of the body’s regulating and defensive functions can be broken or eliminated! To date, the significance of the interference field as an important factor favoring tumor formation and growth has been left practically disregarded. Yet, it is easy enough to imagine that (and to what extent) an interference constantly and negatively influences the cell environment (Pischinger). This includes a pH shift in the extracellular space towards the acid side, whilst alkalosis occurs in the blood. This process finally reaches the point where the previously damaged and cancer-susceptible cell escapes from neurovegetative control, and now the “oncogenic agent” can modify the molecules of nucleic acid and transform the out-of-control cell into a proliferating tumor cell. If this theory (Dosch, Seeger, Varro) is correct or at least possible, it would lead to the following conclusions. Today, the battle against cancer is largely based on surgery, irradiation, and cytostatic drugs. But these cannot break the blockage of the neurovegetative system. On the contrary, they reinforce it all the more! Surgery, radiation treatment, chemotherapy, and immunobiological aftercare make sense only if they also substantially reactivate the body’s own defenses. Of the biological methods now available to us, the reversal and normalization of the basic autonomic functions by skilled neural therapy according to Huneke must, therefore, have first priority. This therapy can normalize the entire electrical power grid by recharging the cells up to their normal electrical potential and protecting the cell membrane against renewed loss of this potential. This happens when neural interference fields and segmental blocks are eliminated by correctly sited injections of procaine. Only when this vital energy balance has been restored in every part of the whole, can the system as a whole again regulate itself and remain at the correct state of dynamic equilibrium for maintaining the dynamic flow that the overall information system has specified. At that point, the problem of reintegrating the cancer cell in the general energy-supply network and of providing it with vital oxygen is no longer insoluble. Varro has demonstrated with striking early results that a combination of neural therapy, by which disturbances in the neurovegetative system are eliminated and normality restored, with ozone therapy is in many cases perfectly capable of arresting the pathological processes involved in the formation of cancer and of making them largely reversible. Other general measures, such as detoxication of the system by changing to a healthier diet, restoring the intestinal flora to a healthy state, desensitization, and other means of activating the body’s defensive capabilities have a supporting part to play in this. Werkmeister has reported that irradiated tissue remains disturbed in its function to the end of the patient’s life. Under local procaine → (T) quaddle therapy, radiation treatment was found to be more effective in dealing with tumors, at lower radiation doses, whilst the adjacent areas that were also irradiated were more effectively shielded. Further, the other unpleasant side-effects of radiation therapy were reduced or completely absent. Telangiectasis did not occur to the same extent in areas protected by quaddles, and any that was already present regressed considerably when the treatment was repeated a sufficient number of times. Effective prophylaxis against ulceration was thus achieved. Werkmeister also confirmed that interference fields have an unfavorable effect on the pathological processes of cancer. This report is supported by Singh who found that procaine (and iodine compounds) stops the DNS repair activity within the cell nucleus and that this effect probably also increases the sensitivity of malignant tumors to radiation therapy. Whilst cancer cannot be cured by neural therapy alone, it is therefore probable that a significant road to its cure leads via a restoration to health of the entire regulating mechanism, including the basic autonomic system, by means of the Huneke therapy. See also → radiation damage. Capsular arthritis → joints. Carbon monoxide poisoning → anoxemia. Carbuncles Infiltrate generously around as early as possible to provide rapid freedom from pain, localize necrotic areas, and promote speedy healing. As carbuncle scars are often found to act as interference fields, this is also the best prophylactic treatment against their becoming interference fields. See also →abscess, → furuncles. Carcinoma → cancer. Cardiac disorders, asthma, edema → heart. Cardiac rhythm, disturbances of → heart. Cardiospasm → abdomen, → achalasia. Carotodynia → neuralgia of the carotid plexus. Carpal tunnel syndrome The median nerve can be disturbed in its sensory and its motor and trophic functions by exostoses, tumors, and inflammation. One of the leading symptoms can be nocturnal brachial paresthesia. Primarily women complain that their hands fall asleep at night and it feels as if their fingers were extremely swollen. Only the pinky finger is spared. Hyperalgesias indicate a pseudoradicular condition and hypoalgesias a radicular lesion. In diffuse sensation disorders, polyneuropathy should be considered. The bilateral carpal tunnel syndrome in the elderly is called “idiopathic” carpal tunnel syndrome. Before attempting surgery, it is worthwhile trying to cure this condition by repeated procaine injections into the carpal tunnel under the transverse carpal ligament where the → (T) median nerve passes through it. For this we use only minute quantities of anesthetic (0.1–0.3 mL), since greater amounts might further damage the compressed nerve by additional pressure. It is even better to inject into the nerve about three fingers’ breadths above the interarticular space, before it enters the carpal tunnel. Injections into the → (T) stellate ganglion and the → (T) brachial plexus nerves may also be indicated. If this neural-therapeutic treatment fails to produce results, the carpal tunnel will have to be decompressed surgically. Cataract → eye disease. Catarrh of the mucous membranes → mucous membranes, catarrh of. Catarrh of the upper respiratory tract → (T) nasal spray with an anesthetic for the mucosa. Causalgia The sharp burning pain, which occurs especially after gunshot wounds with partially severed nerves, is probably due to the transmission of efferent sympathetic activity to afferent nociceptors. As a result, the irritation threshold of the sympathetic system is greatly reduced, first producing vasomotor and later trophic disturbances, which can be triggered by acoustic, optical, or psychological stimuli. The tibial and median nerves and their related segmental tissues are affected particularly frequently. The damp cloth worn by the patient to cover the affected extremity is characteristic of the clinical picture for this affliction, since dampness relieves the pain and dry skin exacerbates it. Therapy Complete temporary blocking of the sympathetic chain and of the peripheral nerves by means of procaine can progressively reduce the irritation of the sympathetic chain causing the symptoms, each time the treatment is repeated. Our “surgeon’s bloodless knife” generally saves the patient from having to undergo sympathectomy or suffering the ravages of chemical nerve destruction. Neurolysis, nerve resection, even mutilating amputation of the extremities, chordotomy, and leukotomy have all proved as ineffective as psychotherapy. Procaine injections, on the other hand, are generally more effective if repeated a sufficient number of times. They cannot harm and are repeatable at any time. In conservative causalgia treatment, the physician’s patience and perseverance should not be less than that of the suffering patient. In all cases of pain syndromes after damage to peripheral nerves, neural therapy with local anesthesia has proven to be the most successful and recognized treatment method. In gunshot wounds, we infiltrate entry and exit scars and all surgical scars as far as the point of nerve contact in the old projectile path. Where the bone has also been injured, we go as far as the periosteum on the bone scar itself and, if possible, also to and into the adjacent → (T) arteries. Nerve contact with the needle produces a defensive reflex movement by the patient, for which both he or she and the physician should be prepared, and an assistant must always fix the extremity: 1. Upper extremity: To and into the → (T) brachial artery and plexus (→ (T) nerves), or directly into the radial, ulnar, and especially the → (T) median nerves along their course, and always also into the → (T) stellate ganglion. 2. Lower extremity: Injections intra- and periarterially to the → (T) femoral artery and the adjacent → (T) femoral nerve or to the tibial nerve that can be deactivated at the center of the upper thigh or back of the knee. Also → (T) presacral and → (T) epidural infiltrations and always to the → (T) celiac ganglion at the level of L1 through L4, preferably bilaterally on account of the interconnected right and left lumbar splanchnic nerves in the abdominal plexus. If these combined injections within the segment fail to bring results, we must also remember, even when we treat a causalgia patient, that an interference field may be affecting our chances of success. If an interference field has previously damaged the sympathetic system, it may now be keeping up a constant irritation from beyond the segment. See also → amputation-stump pains, → neurocirculatory disturbances, →phantom-limb pains, → post-traumatic osteoporosis. Cerebral concussion → concussion, cerebral. Cerebral edema Every edema has its origin in a dysregulation. Dehydration of the brain and the reduction of intracranial pressure can begin only when the autonomic system resumes its regulating functions. To achieve this, we inject a 2% procaine solution intravenously (→ (T) intravenous procaine injections) (possibly together with 40% glucose and a diuretic) and under the → (T) scalp. Anesthesia of the → (T) stellate ganglion normalizes the endothelial barrier and allows the cerebral edema to drain. See → concussion, cerebral. Cerebral embolism → stroke, → vascular occlusion. Cerebral hemorrhage → stroke. Cerebral injury If the injury is new, procaine intravenously (→ (T) intravenous procaine injections) and under the → (T) scalp will help regulate body temperature and circulation. See also → shock. Cerebral lues → syphilis, cerebral. Cerebral sclerosis → geriatric disorders. Cerebral tumor In inoperable tumors or post-operative headache etc., procaine is injected intravenously (→ (T) intravenous procaine injections), under the → (T) scalp, possibly also to the → (T) stellate ganglion. Cerebrovascular accident → stroke. Cervical erosion The condition is generally the result of cervical hypersecretion and is treated with paracervical injections to → (T) Frankenhauser’s plexus. The autonomic dysfunction as the origin of the condition can be addressed with injections into the → (T) thyroid. See also → pelvis. Cervical migraine → migraine, cervical. Cervical syndrome The cervical spine is the most flexible part of the spine. This makes it prone to degenerative changes and intervertebral lesions. The pathological symptoms that center on the cervical region and that are summarized under the term of “cervical syndrome” are generally based on mechanisms that differ from one another as regards both their etiology and their pathogenesis. Thus, changes in the joints, tendons, and ligaments, muscles, nerves, and vessels, either singly or, more frequently, in combination, can cause similar disorders or symptoms and, further, produce dysfunctions in other systems. Psychological, autonomic, neural, and hormonal components often combine to produce a complex clinical picture in which it is no longer possible to distinguish between cause and effect. More importance is generally attached to the x-ray as a provider of significant information than it really deserves. It merely allows us to exclude from our list of likely causes such disorders as cannot be treated by neural therapy, or at least not by neural therapy alone: vertebral caries, traumatic changes, tumors, hereditary abnormalities, and the like. Evidence of degenerative changes that may have occurred does not mean very much. Morphological changes, even if they are extensive, are no conclusive proof that they are the cause of the symptoms of which the patient complains. The x-ray is merely a diagnostic aid, a tool that must not mislead us or stop us from trying to help the patient with our therapy. Cervical spondylosis and → osteochondrosis can lead to irritation of the cervical sympathetic system and, by compression of the nerve roots, to radicular neuritis. In addition, the → (T) vertebral artery with its periarterial autonomic fibers is often also irritated. One of the results of this is that perceptible → muscle spasm occurs at some depth in the musculature of the neck and shoulders. Acute disk prolapse in this region is much less frequent. The upper cervical syndrome produces the following symptoms: pressure pain at the spinous processes of the upper cervical vertebrae and exit point of the → (T) occipital nerves, reflex muscle tension, pain in the neck and the back of the head, occipital neuralgia, cervical migraine, tinnitus, and dizziness (→ vertebral artery compression syndrome). The middle cervical syndrome causes shoulder pain and may be accompanied by paroxysmal tachycardia and motor dysfunction of the diaphragm. If the pain is not exacerbated when the head is moved, for example, in bending or stretching the neck, inclining the head sideways or rotation, the cervical column can be dismissed from the list of possible causes (periarthritis of the humeroscapular →joint). The lower cervical syndrome presents the symptoms of pain and fibrositic nodules in the region of neck and shoulders, and of brachialgia or epicondylitis. Pain usually begins in the neck and extends primarily into the lateral part of the shoulders and arms (→ joints, shoulder-arm syndrome). Reflex muscle tension in the shoulder and neck area limits the mobility of the cervical spine. Pain, paresthesias, and even hand muscle atrophies may occur in the hands. Differential diagnosis of neuralgia or fibrositis Bend the patient’s head forward and to the side of the pain. Nerve pain will be exacerbated by the additional compression, whilst pain due to fibrositic nodules will be attenuated because of the relaxation produced by this movement. The contrary effect is produced when the head is bent forward and to the opposite side: the nerve pain is attenuated by the relief given to the compressed nerve roots, whilst stretching exacerbates the pain due to fibrositis. Treatment Procaine intravenously (→ (T) intravenous procaine injections), plus → (T) quaddles over the fibrositic nodules found by palpation and over the hyperalgetic points in neck and shoulders. Take the tense muscle between the fingers of the left hand, raise it and infiltrate intramuscularly (→ (T) intramuscular infiltrations) to a depth of 30–40 mm through an intracutaneous → (T) quaddle (beware of intrapulmonary and intra-arterial injections!), then distribute the local anesthetic by circular massaging movements. In addition, inject to the atlas process and the periosteum of percussion-sensitive spinous and lateral processes of the cervical vertebrae. Even more effective are injections to the → (T) nerves (afferent), especially to the → (T) occipital nerves and into the cervical and brachial plexus, and to the → (T) stellate ganglion. The latter will eliminate not only the irritation to the cervical sympathetic system but also one of the factors that may cause osteochondrosis. However, this injection may have to be repeated anything up to 10 times in order to have a genuinely permanent effect. First aid can also be given by blocking the accessory nerve: insert the needle 20 mm below the mastoid process on the dorsal edge of the sternocleidomastoid muscle and infiltrate about 5 mL by slowly advancing the point of the needle into the muscle. As the sternocleidomastoid muscle relaxes, the pain in neck and shoulder disappears. Also try injections into the posterior third of the lower → (T) nasal concha or use a → (T) nasal spray. In therapy-resistant cases, find the interference field. When faced with these symptoms, I always start my search with the tonsils. Any injury that remains painful longer than would have been expected from the severity of the trauma suggests that in addition to the psyche there may also be an interference field involved. See also → intervertebral disk, damage to. Cervicalrib syndrome → scalene syndrome. Cervicitis → pelvis. Chapped skin → rhagades. Charlin syndrome → neuralgia of the nasociliar nerve. Chilblains Infiltrate locally. Chin If → (T) quaddles over the chin do not suffice, an x-ray of the lower incisors is advisable. Also try injections to the → (T) teeth, especially into the gingival pockets. See also→ (T) mental nerve. Cholangiolitis, cholangitis, cholecystitis, cholelithiasis → abdomen. Chorea minor I have cured two cases of this disorder by the Huneke phenomenon via the tonsils. This proves that the cerebral irritation can be due to an interference field. An 11-year old girl was convulsed by spasms to such an extent that she could no longer walk, feed herself, or speak. After a positive tonsil test, she got up perfectly normally, said goodbye quite distinctly and went out through the door without assistance, as though she had never been ill. Parents, doctor, and assistant looked at each other speechlessly, until their surprise found relief in laughter. Such dramatic cures can, of course, be experienced only by someone who can believe that they are possible and who will try to set them in motion. Someone who does not regard him or herself as competent to cure recondite symptoms will never be able to cure them, simply for want of trying. In the case of this girl, incidentally, the same treatment was repeated a fortnight later to eliminate the remainder of the minor spasms that had recurred. Choreoretinitis, disseminated → eye disease. Choroidal disorders → eye disease. Ciliary neuralgia → headache, → neuralgia. Cillosis → (T) nerve-exit points of the supraorbital nerve. Circulatory disturbances → neurocirculatory disturbances. Civilization disorders → neurovegetative dystonia, → cancer. Claudication, intermittent → neurocirculatory disturbances, → sciatica (post-sciatic circulatory disturbances). Clouding of the lens → cataract, → eye disease. Cluster headache (Bing–Horton syndrome) Primarily in the evening or at night, lasting 20–120 minutes, intense unilateral headache with burning pain of the eyes, forehead, temples, and back of the head. Redness and swelling of the affected side of the head with associated strong pulsation of the temporal artery. Redness of the conjunctiva with lacrimation and rhinorrhea, possibly ptosis and miosis as incomplete Horner syndrome. Intervals often lasting months. Therapy An attack can be brought on by histamine, which slackens the walls of the vessels and increases the permeability of the capillaries. Procaine is a histamine antagonist and seals the vessels. We administer it intravenously (→ (T) intravenous procaine injections) on the affected side, around and under the → (T) temporal artery, and into all pressure points. In addition, also to the pterygopalatine and → (T) stellate ganglion. For the case of an attack, → (T) nasal spray should be prescribed for the patient, or a superficial anesthetic (2% pantocaine or 4% lidocaine solution), which can be applied with a cotton swab into the nostril of the affected side. See also → migraine, → neuralgia. Coccygodynia A circumscribed pain and pressure sensitivity in the coccygeal region, which increases after prolonged sitting, when bending down and during defecation. It can be caused by trauma, dislocation of the coccyx, neuralgia of the sacral plexus, prostatitis, or inflammation of the rectum. Treatment Injections to the periosteum of the coccyx and laterally to the nerve branches and to the ventral area of the coccyx (to the ganglion impar, where the ends of the two sympathetic trunks unite) have proved effective, also into the second to fourth posterior → (T) sacral foramina, → (T) epidural or → (T) presacral infiltrations. If the results are not satisfying, injections to the → (T) pudendal nerve or the → (T) sacral plexus (→ (T) sciatic nerve). Further, injections into the → (T) pelvic region, the → (T) prostate and perianal infiltrations should also be tried, since coccygodynia can also be kept in being by an interference field in the adjacent areas. Old, more or less still painful contusions of the coccyx can act as interference fields and cause remote disturbances years later. Coccyx, contusion of If one strikes the bottom of a corked bottle sharply with the flat of the hand, the cork may be ejected with some force from the neck of the bottle. In exactly the same manner the sudden surge of fluid in the liquor space provoked by severe contusion of the coccyx can produce → concussion with all its usual consequences, although no direct force has been applied to the head as such. Cold, common → coryza. Cold feet → feet, cold. Cold injury → frostbite, → neurocirculatory disturbances. Colic → abdomen, → kidneys. Colitis → abdomen. Ulcerative or mucous colitis (with blood and mucous secretions from the intestines, tenesmus, obstipation, and meteorism) are frequently caused by food → allergies (primarily lactic protein). Therapy → abdomen. Often, the patient accurately localizes the site of inflammation of his or her intestine or where the spasms occur. He or she should be asked to dig his or her fingernail into the point where they feel the maximum pain inside. The mark left by their fingernail is the site for setting our → (T) quaddle. We then go through this to probe further down to the peritoneum, which is always very pain-sensitive in these cases. If we cannot find an “ouch point” in the place indicated by the patient, we have to use the point of the needle to look for the hyperalgetic peritoneal area (→ (T) preperitoneal infiltration). Without an ouch point there can be no healing reaction! As is always the case with segmental therapy, this treatment should be repeated when the condition recurs. There is absolutely no reason to have any doubts or misgivings about this treatment. With the patient in the recumbent position, the (insensitive) intestine is not normally reached if the correct procedure is followed. Collapse Procaine intravenously (→ (T) intravenous procaine injections) will reliably regulate circulation and reduce vascular permeability. In animal experiments it is possible to bring about a collapse artificially (Bezold-Jarisch reflex). When procaine is given intravenously, collapse does not occur (Hirsch, Keil, Muschaweck). In sympathicotonic collapse, anesthesia of the → (T) stellate ganglion or the carotid glomus (→ (T) carotid artery) has been found to have a tonic effect on the circulation. See also → shock. Colon Firstly, exclude carcinoma as a possible cause, then → (T) quaddles over the lower abdomen and coccyx. If this is inadequate, → (T) epidural or → (T) presacral infiltrations, combined with injections at the ventral side of the coccyx. Possibly also injections into the → (T) prostate or the posterior → (T) sacral foramina. See also → anal disorders. Colon, congenital dilatation of → megacolon. Colonic spasms → colitis. Colonopathy → intestinal dysfunctions, → colitis, → abdomen. Colpitis → pelvis. Coma, hepatic → abdomen. Commotio cerebris → concussion, cerebral. Concentration, lack of → geriatric disorders, → arteriosclerosis, → neurodystonia. Concussion, cerebral Every cerebral concussion acts like a → shock and causes a pathologic state of excitation in the brain. It is responsible for vessel spasms and paralysis and for increased permeability of the vessel walls, which causes → cerebral edema. The swelling of the brain is the reason for sudden changes in all areas of consciousness, including dizziness, fainting or coma, headache, vertigo, vomiting, sleep disorders, or retrograde amnesia. Usually the symptoms are temporary and go down within 4 days (first degree) or within 3 weeks (second degree). At this point, most patients are able to work again. Cerebral concussion is the more or less extensive tissue damage of the brain substance, which is anatomically perceivable. In addition to the cerebral concussion symptoms (which can be missing), neural failures of different degrees can be noted. These disorders ease after 3 weeks or later (third degree) and take forms from hyperexcitation to paralysis, aphasia, apraxia, and traumatic → epilepsy. After 10 or more years, late-onset disorders due to slowly progressing degenerative processes may appear, such as severe → headache, cerebral angiopathy, epileptic seizures, or psychological changes resulting in personality changes. The latter can produce lack of motivation, irritability, ethic or moral deficiencies, and even lapse into crime. The affected people notice these changes and if they cannot get help they might choose suicide to end their suffering. Therapy Drug therapy of brain trauma is costly, has side-effects, and is not very successful. Neural therapy should be the treatment of choice. Brain function depends primarily on the condition of the vascular system. Non-reversible symptoms such as, headache, vertigo, insomnia, lack of concentration, nervousness, and psychological changes are generally caused by vascular spasms of the arterioles (Riechert). The → (T) intravenous use of procaine (but not lidocaine and mepivacaine) and its injection under the → (T) scalp (at the level of the temples and the parietal bone, the location of the trauma and the opposite side) produces vascular dilatation and reduces vascular permeability either directly or through dermatovisceral and osteovisceral reflex pathways. It normalizes the intracranial vascular tone and the disturbed peripheral blood circulation, reduces central excitation, and suspends pathogenic reflexes. In the case of craniocerebral trauma an increased amount of acetylcholine is secreted. Procaine inhibits the secretion at the synapses of the central nervous system and protects the brain cells. Our strongest means against cerebral edema and the results of brain damage, even in older cases, is anesthesia of the → (T) stellate ganglion. The removal of the dangerous brain swelling in the acute state is as imperative as it is difficult. The spacial constriction caused by the skull causes irritation and compression damage that can be fatal. The approach that utilizes drug-induced dehydration has more side-effects than therapeutic results. Dehydration depends on the restoration of the regulating activities of the autonomic system. Anesthesia of the stellate ganglion normalizes the autonomic regulation of the corresponding upper body quadrant. It stops the edema formation through normalization of the endothelial barrier and draining of the edema. The suspension of the cervical sympathetic trunk leads to further dilatation of the vessels. Between the destroyed brain tissue and the healthy brain tissue there is always a damage zone. In this zone, vascular spasms inhibit the removal of detritus and metabolic roughage and the distribution of proper amounts of oxygen and nutrition. By removing the vascular spasms we can save whatever is salvageable and restore the function of parts of the tissue that would otherwise be doomed. What is destroyed remains destroyed. Even in older cases, with sufficient repetition of the injections, considerable improvement of mental and physical mobility can be achieved. Injections into the → (T) thyroid can lessen persistent autonomic hyperexcitability due to shock. With proper indication, → (T) cisternal procaine injection should be considered in the case of interference field formation in the brain. If our efforts are without success, we have to search for an interference field that has weakened the system previously via first insult (Speransky) and prevents positive results from the generally helpful injections. Neural therapy deserves more consideration in the treatment of cerebral concussion and its consequences because it has proven successful, particularly when used at an early stage to act prophylactically. Cerebral concussion can occur without trauma to the head; see → coccyx, contusion of. Case History 22: F. S. Clerk, Aged 48 In a motorcycle accident, F.S., a 48-year-old clerk from Beelitz, suffered a jaw fracture, several lacerations on the head, and a basal skull fracture with cerebral concussion. Due to the danger of suffocation a tracheotomy was performed. Horner syndrome on the left was indicative of damage to the cervical sympathetic trunk. Clinical diagnosis: severe cerebral concussion (craniocerebral trauma III). His health history included: bullet lodged in lung, shell splinter damage to the popliteal area. His main complaint was an imbalance disorder that had remained unchanged in spite of intensive specialized treatment for 1 year. The last diagnosis from a specialist that was made 9 months after the accident and 3 months before I began treatment: ptosis left, pupillar light reflex weak on the left, good on the right, and idiomuscular abdominal reflex slightly weaker on the left than on the right. Finger-nose test: great deviation on the left with poor correction. Knee-heel test: exaggerated motion on the left. Romberg’s test: staggering, adiadochokinesis on the left. Walking a straight line with eyes closed very shaky. After the first intravenous procaine treatment under the scalp, infiltration of all head, neck, and chest scars as well as the left stellate ganglion, the imbalance disorder improved immediately. He was able to dance, ride his bicycle and motorcycle, which was previously out of the question. One week after my treatment, the laconic diagnosis of his specialist, who was also the head of a district hospital, read: “In-depth neurological examination shows, in addition to ptosis on the left, only an idiomuscular abdominal reflex favoring the right, otherwise no particularities.” Two follow-up treatments, 1 and 3 months later, removed all other complaints entirely. Congenital dilatation of the colon → megacolon. Conjunctiva, conjunctivitis → eye disease. Constipation In chronic, spastic, or hypotonic constipation, injections to the left (occasionally also to the right) abdominal → (T) celiac ganglion and into the → (T) epigastrium produce a striking, sudden improvement in over half the cases. If we want to involve the cutaneovisceral reflex pathways, we have to set → (T) quaddles in the Head’s zones related to the intestine: • Small intestine: T9 to T11 with focus on the umbilicus and the area to the left and right of it; also dorsal. • Large intestine: T11 to L1, particularly a strip three fingers’ breadths below the umbilicus to three fingers’ breadths above the symphysis. Do not forget the dorsal Head’s zones. If we find any hyperalgetic points by palpation of the abdomen we administer → (T) peritoneal infiltration. The area of McBurney’s point and the corresponding area on the left abdomen should also be included. If there is an appendectomy scar, this must always be treated at the same time as a → (T) scar in the segment. If there is hypotonia in the rectum, a → (T) presacral infiltration is indicated in addition to quaddles in the dermatome T10 through L3 ventrally and dorsally. If this is ineffective, search for the interference field. In this, all scars, the pelvis, and paranasal sinuses should be borne in mind. Hypotonic constipation occurs more frequently in women than in men. Thus, women should also receive injections into the → (T) pelvic region. In hypotonic forms, treatment of the nasal reflex zone of the middle → (T) nasal concha or merely a → (T) nasal spray may yield results. There should be no premenstrual nasal treatment, to avoid provoking premature and painful menstrual bleeding! Acupuncture recommends injections of the sole of the foot at a depth of 5–10 mm, where the ball of the big toe joins that of the small toes. The use of laxatives must be cut down and replaced by lactose, linseed oil, and by recommendations for a low-carbohydrate high-protein diet. Psychogenic cases cannot be cured by neural therapy. A depressed patient is often constipated, and the chronically constipated are often grumpy and prone to depression. See also → abdomen. Contracture In contracture, ligaments and muscles are subjected to neuroreflectory pathological tonus changes with greatly increased tone and may lead to shrinkage of capsules and ligaments, and ultimately to ankylosis. → (T) Quaddles around the joint and → (T) intramuscular infiltrations into the affected areas of tissue block these reflexes and restore the possibility of regression, since normal tonus returns because of the break made in the pain cycle. If these and further injections into the → (T) joints, the → (T) afferent arteries and nerves, and into the lumbar → (T) sympathetic chain or the → (T) stellate ganglion produce no substantial change, we must ascertain whether an interference field is not preventing the restoration of normal conditions. Contusions → injuries. Convulsions in pregnancy → eclampsia, pre-eclampsia. Coracoiditis In the case of painful inflammation of the coracoid process at the shoulder level, 1 mL 1% or 2% procaine solution is given intravenously (→ (T) intravenous procaine injections) on the side of the inflammation, and about l mL to the painful → periosteum; in stubborn cases, injections also into the homolateral → (T) stellate ganglion. Otherwise, look for the interference field. See also → cervical syndrome. Corneal herpes → eye disease. Corneal ulcer → eye disease. If neural therapy is started early enough, opacities can be prevented. Even severe clouding can still be reduced by neural-therapeutic treatment. Corns Infiltrate down to the periosteum and lift out the corn. As a curiosity, I once found a painful corn to be the interference field responsible for a headache. One really needs to think of everything! Coronary disease coronary insufficiency, sclerosis, spasms: → heart. Coryza A → (T) nasal spray repeated several times will stop incipient coryza and relieves a cold that has already taken hold. Chronic rhinitis: → nose. Costoclavicular syndrome If the nerves and vessels in the area between the first rib and the clavicle are compressed, symptoms may present that generally correspond to the → scalene (cervical rib) syndrome. This disorder is common amongst asthenics with severely sloping shoulders. Cough reflex To reduce an irritating cough during intubation or surgery and to cough up bronchial secretions painlessly after surgery, Zipf recommends procaine given intravenously (→ (T) intravenous procaine injections). See also → pharyngitis. Coxarthritis, coxarthrosis, coxitis → joints. Cracked skin → rhagades. Cradle cap (crusta lactea) → skin. Very often, injection into the → (T) tonsils, repeated if necessary, will be effective. This injection can also be administered to infants. CVA → stroke. Cystic fibrosis This is a hereditary pancreatic disease with fibrous changes and cyst formation combined with a disturbance of all mucous-secreting glands. Particularly the bronchial glands produce only viscous mucous. Even in infants it is possible to try to alleviate the secondary symptoms with anesthesia as a complementary means by injecting the left → (T) celiac ganglion and the → (T) stellate ganglion (alternating between right and left 1 to 2 times a week) (Mora, Werthmann, Wischnewski). Cystitis We set → (T) quaddles in the segment, i.e., over the region of sacrum, coccyx, and symphysis (dermatomes T12 through L3, S2). In stubborn cases, → (T) epidural or → (T) presacral infiltration. It is also possible to instill 5–10 mL of 2% procaine solution into the empty bladder and then have the patient change position as in roll therapy. This improves tenesmus quickly and removes the complaints. See also → kidneys, → bladder, irritable. Dacryocystitis → eye disease. Deafness, defective hearing → ears. Degenerative diseases See Chapter 3 on Rejuvenation Through Procaine?, Part I, Section C; → geriatric disorders. Degenerative hip arthrosis → joints. Delivery → obstetrics. Dental extractions, after-pains Inject about 0.3 mL into the buccal and palatine aspects of the gums (→ (T) teeth). Apart from eliminating local pain, this will also dispose of all extradental side-effects and symptoms such as headache, neuralgia, or backache. Dento-alveolitis → periodontosis. Depression Depression is not necessarily an illness as such. It often accompanies as a secondary symptom some other deep-seated disorder caused by an interference field, and, in such cases, it can be eliminated via a lightning reaction. For premenstrual depression: → dysmenorrhea. Therapy Test injection into the → (T) thyroid, for women also into the → (T) pelvic region. Also test thoracic area with → (T) quaddles above the chest and paravertebrally. Procaine preparations, even when administered at random, have some anti-depressive effect. This is probably due to MAO (mono-amino oxidase) inhibition in the brain and a raised irritation threshold for the impulse transfer by the nerve tissues (Ostfeld). Dercum disease → obesity. Dermatitis In acute dermatitis, give procaine or lidocaine intravenously (→ (T) intravenous procaine injections). Dermatitis herpetiformis → Duhring disease. In infantile seborrheic dermatitis, search for the interference field (umbilicus, tonsils, ears?). See also → skin. Diabetes insipidus Procaine intravenously (→ (T) intravenous procaine injections) and bilaterally under the → (T) scalp. Diabetes mellitus Infections, toxins, mental and physical trauma can stress an incompetent pancreas to the point of total exhaustion. In this, irritations are transmitted via the autonomic system to the higher-order diencephalo-hypophyseal system. The nutritional disturbance and the exhaustion of the functioning portion of the pancreatic apparatus can be temporary and reversible, especially at the beginning. In such cases the attempt to restore the regulating mechanisms to normality (in addition to diet and carefully dosed amounts of insulin or oral anti-diabetic preparations) can often achieve the object. There is still no practicable means available to the general practitioner for determining whether the disease may be due to a disturbance in the autonomic command-transmission system, whilst the glandular apparatus remains largely intact. In other words, in this type of situation the body is producing adequate quantities of insulin, but the response of the chemical receptors to the signals they receive is faulty. This is especially the case in overweight diabetics. We assume that in these cases the normal transmission of information can be restored by the repolarization and restitution of the cells. But this is worthwhile only if the treatment is started early and is carried through consistently. When too many regulating systems have become involved in the pathological processes, the disease can become irreversible. A pancreas whose insulin-producing cells have been destroyed cannot, of course, be made to function again. Even if the percentage of cures is not very high, the cures achieved within the segment by injections alternately left and right into the abdominal → (T) celiac ganglion and into the → (T) epigastric region, and via an interference field, prove that it is worth the attempt. This has a positive effect on diabetic enteropathy (diarrhea, stearrhea, reduced acid production, and disturbed stomach emptying). Diabetic gangrene → neurocirculatory disturbances. Diabetic polyneuritis → neuritis, → neurocirculatory disturbances. Diaphragmatic hernia → hiatus hernia. Diarrhea → abdomen. Digestive disorders → abdomen. Dilatation of the colon, congenital → megacolon. Discharge, vaginal Exclude gonorrhea or trichomoniasis. See also → pelvis, → gynecological dysfunction. Disequilibrium Exclude the possibility of a → cerebral tumor! Inject procaine intravenously (→ (T) intravenous procaine injections) and under the → (T) scalp, or to the → (T) stellate ganglion (see Case History 22). In cases of vestibular vertigo, see → ears, → vertebral artery compression syndrome. If of no avail, find the interference field (see Case History 5, Part I, Section C, Chapter 2). See also → vertigo. Dislocated shoulder → joints. Dislocation To reduce a fresh dislocation simply, the periarticular infiltration (→ (T) joints) of procaine is in many cases perfectly adequate! It also suppresses the formation of → hematomas. If the dislocation is not recent, also inject into the affected → (T) joint and intramuscularly (→ (T) intramuscular infiltrations) into the muscle spasm, followed by reduction under anesthetic. This ensures rapid healing and prevents → contractures. If necessary, follow-up treatment with accurately sited → (T) quaddles and deeper injections to any hyperalgetic points found by palpation, also to the sensitive periosteum of the points of attachment of tendons and ligaments. See also → joints → dislocated shoulder. Disuse atrophy Atrophy of the muscles due to inactivity is often the result of pain following → injuries or → inflammation. These causes are easily eliminated by injections into the tissue affected by pain, to restore mobility within a short time. Dizziness → disequilibrium, → vertigo. Dropsy, cardiac → heart. Dry pharyngitis → pharyngitis sicca. Duhring disease dermatitis herpetiformis. Infiltrate around and under the blisters. Duodenal ulcer → abdomen. Duplay disease → joints (humeroscapular periarthritis). Dupuytren’s contracture The etiology of the shrinking of the palmar aponeurosis, the tendon sheaths of the fingers, and the skin is unknown. In addition to a hereditary disposition, irritation of the spinal root, cervical sympathetic trunk, and ulnar nerve have to be considered. Before choosing the surgical approach, injections to the → (T) stellate ganglion and the → (T) ulnar nerve are indicated. Repeated procaine injections of about 5 mL into the chronically inflamed contracting scar tissue soften it noticeably. If the treatment is repeated a sufficient number of times, the contracture will improve. Post-operative fibrosis can also be substantially improved by this treatment. If the disease is due to lack of vitamin E, this missing building block must be given in addition. Like any other pathologically changed tissue, Dupuytren’s contracture can also become an interference field for other disorders, as has been proved by lightning-reaction cures (see Case History 25). Dysbasia, angiospastic → neurocirculatory disturbances, → (T) sciatic nerve (post-sciatic circulatory disturbances). Dyshidrosis, dysidrosis → hyperhidrosis. Tendency to sweating of hands and feet, in → rheumatism; → thyrotoxicosis, → menopausal disorders, → neurodystonia. Dysmenorrhea and premenstrual syndrome including depression and aggressive irritability Exclude organic causes such as inflammation, fixed retro-version, endometriosis, adhesions, myomas, etc. Generally, however, the cause is functional or psychological. In functional dysmenorrhea, neural therapy is reliable in helping the patient. If the pain abates when bleeding begins, there may be a spastic or organic obstruction at the cervix uteri. In such cases, → (T) quaddles over the sacrum and the symphysis pubis will help, through which we can infiltrate down to the peritoneum. Still better are injections into the → (T) pelvic region or to → (T) Frankenhauser’s ganglia (before the onset of the period). If there is severe backache, also inject into the → (T) sacroiliac joints. These injections will result in painless periods and the flow will become normal. If pain continues beyond the onset of the period, the patient may be suffering from “nasal dysmenorrhea.” A correctly sited injection of local anesthetic into the inferior → (T) nasal concha will, in such cases, eliminate the hypogastric pain, and injection of the septal tubercles will eliminate the backache. A → (T) nasal spray with 2% pantocaine solution is much simpler and will generally suffice. Dysosmia → nose. Dyspepsia in infants → gastroenteritis, infantile. Dysphagia → (T) vertebral artery, → (T) stellate ganglion, → (T) superior laryngeal nerve, → (T) glossopharyngeal nerve, → (T) tonsils. Dyspnea Depending on origin: → heart, → lungs. Dystonia, neurovegetative → neurovegetative dystonia. Dystonia, pulmonary intravenously (→ (T) intravenous procaine injections) with → (T) quaddles above the chest and back. If that does not suffice: → (T) stellate ganglion. Dystrophy → malnutrition, → abdomen. Ears The hearing apparatus of the inner ear is an arterial end organ, i.e., one that is not secured by a collateral circulation. For this reason it reacts especially sensitively to circulatory disturbances that can produce such symptoms as partial deafness, tinnitus, or vertigo. If the symptoms vary and tend to appear as recurrent attacks, a vertebral genesis must be suspected. Any irritation of the cervical sympathetic chain and of the sympathetic fibers can produce a response in the form of vascular spasms with their serious consequences. Any therapy capable of eliminating this irritation of the nerves and of normalizing the blood supply is bound to offer a hope of success. In certain cases this may be achieved by manipulative therapy of the cervical spine. But neural therapy is generally successful, by means of accurately placed injections. For segmental treatment of all disorders affecting the ears, including labyrinthine vertigo, we have the following means at our disposal: 1. → (T) Intravenous injections on the affected side and, if both sides are involved, alternately left and right. This dilates the afferent vessels and seals them. In small children, we obtain the same results by periarterial injections to the → (T) brachial artery. This injection can instantly and by itself eliminate all pain and any inflammation that may be present. 2. In addition to the intravenous injection we also inject behind the earlobe to the anterior edge of the → (T) mastoid process. This point corresponds to TB-17 in acupuncture. In disorders of the ear we also make use of the “gate of the ear” (TB-23) in the dimple between tragus and upper attachment of the external ear, and of TB-18, which lies a fingers’ breadth behind the middle of the ear (above the supra-mastoid ridge), where it is usually palpable as a dimple. Another helpful point in the case of tinnitus is located at the posterior ramus of the mandible, approximately 1 cm superior to the mandibular angle. A small dimple can be palpated at this point. The direction of injection is toward the corner of the mouth. If this caused toothache, the tip of the needle has to be adjusted cranially. 3. → (T) Quaddles can also help in disorders affecting the ear. These act both directly and indirectly upon the inner ear via cutaneovisceral pathways. We set four to six quaddles in the region of the cervical segments C2 through C3 on both sides of the spinous processes, starting two fingers’ breadths below the inferior border of the occipital bone. We also set quaddles over the ends of the lateral processes of the first cervical vertebra (atlas), over the depressions behind the ear lobes and, if the periosteum is pressure-sensitive, we also go down to the periosteum itself. 4. An injection to the → (T) stellate ganglion can still be effective where the injections described in (1) to (3) above are not enough. The previously pale eardrum turns as red as a beet and the dilatation of the labyrinthine vessels has also been demonstrated. Because the labyrinth is supplied by the → (T) vertebral artery we can affect the inner ear through injections to its periarterial plexus. 5. We can expect a similar effect from para-arterial injections to (but never into!) the → (T) carotid artery. 6. Injection to the medial pterygoid nerve. As soon as the mandibular nerve leaves the cranial cavity by way of the foramen ovale, it devides into its branches (Gasserian [otic] → (T) ganglion). The medial pterygoid nerve is the most central of those banches and supplies not only the muscle of the same name and the tensor veli palatini muscle but also the tensor tympani muscle. In that way the objective tinnitus can be affected. 7. For the injection into and to the eustachian tube, the needle is inserted 10 mm cranially from the upper tonsillar pole (→ (T) tonsils) and is then pushed about 10–20 mm in the direction of the external auditory canal. The patient will indicate when he or she feels the liquid in the ear. See also under → (T) glossopharyngeal nerve. Indication: acute and chronic tubal catarrh. 8. Where there is pain in the external auditory canal, we anesthetize the posterior branch of the greater auricular nerve. This surfaces about 20 mm caudally from the mastoid process, at the posterior edge of the sternocleidomastoid muscle and runs from there to the base of the auricle. In the case of → neuralgia: → (e) intermedial nerve and (u) tympanic plexus. 9. In cases of vertigo, severe tinnitus, the sudden onset of deafness, and Ménière disease, which do not respond to intravenous injections and to anesthesia of the mastoid and of the stellate ganglion, anesthesia of the eardrum (labyrinth) may be effective. This should be carried out by a specialist, as follows. Anesthetize the eardrum by instilling 2% panto-caine or 4% lidocaine (Xylocaine) solution mixed with the contents of an ampul of dried kinetin (hyaluronidase). Introduce a tubal catheter through the nose and insert a thin wire mandrin with lubricated cottonwool. This prevents the liquid from flowing out of the tympanic cavity. The patient lies flat on his or her sound side. Using a fine needle, 0.7 mL of the mixture of anesthetic and kinetin is injected through the posterior lower quadrant of the drum. After 20 minutes to half an hour the local anesthetic will have diffused into the labyrinth. Nystagmus to the opposite side will occur and be accompanied by severe vertigo and possibly by vomiting. The dizziness will persist for 2–3 hours and can be relieved by the administration of an anti-emetic. One injection will generally suffice, but occasionally two or three may be required. In about a third of the patients, hearing may be impaired, but the majority accepts this as the lesser evil. If necessary, segmental injections should be repeated once or twice weekly. If they are ineffective, we need once again look for an interference field. In this context, Kretzschmar (United States) reported a number of cures by lightning reaction following injections into the epigastrium. In some of these cases, the patients were suffering from advanced inner-ear deafness. Their deafness thus proved to be the remote effect caused by an abdominal interference field. Acute and chronic otitis media Procaine deals with inflammation by attacking it in its essence, whilst antibiotics attack the pathogenic agents. A local anesthetic can ordinarily cause both acute and chronic otitis media to heal quickly and without complications. Initially, increased secretion should be regarded as a favorable reaction in these cases. In scarlet-fever otitis we additionally give injections to the → (T) tonsils. We do not treat cholestea-tomata or severe destruction of the inner ear. These must be referred to a specialist! Defective hearing Treatment as stated. If inner-ear deafness occurs suddenly and is unilateral even without any vestibular symptoms, an autonomic vascular etiology should always be borne in mind. Mechanical constriction of the intervertebral foramina and compression of the afferent arteries due to changes in the cervical spine are less important in producing the disorder than the part played by sympathetic interference impulses, which produce labyrinthine hydrops, with oxygen deficiency and pressure on the nerve cells. Neural therapy can eliminate the neural irritation that is the cause. Earache can also be caused by the teeth! A diseased second upper molar and the sixth and seventh tooth of the lower jaw can radiate pain to the ears. Otosclerosis Investigations have shown that about half the cases of clinical otosclerosis are accompanied by an autonomic inner-ear disturbance and that otosclerosis is frequently the result of such a disturbance. Combined treatment of the → (T) sympathetic chain and spine is recommended at the start of this disorder. Post-auricular scars following total mastoidectomy We often encounter these as causes of remote disturbances. Care must be exercised in testing deeply in-drawn scars. Only a superficial → (T) quaddle should be set at the bottom of the funnel-shaped scar. Because of the proximity of the meninges, deeper injections can produce unpleasant reactions such as vertigo and vomiting. Here (and only here!) it is therefore better to infiltrate around the scar and to go to the adjacent periosteum, whilst we normally inject in depth directly into the scar itself. Sudden deafness Occlusion or constriction of the internal auditory artery can cause loss of hearing. Reversible intravascular clotting of red blood cells (blood sludge) is discussed as another cause. There is little hope of curing or even partly restoring this loss unless the blood supply to the inner ear can be improved within the first week to fortnight. The same is true in the case of blood sludge. The use of procaine can inhibit the clotting of red blood cells through vessel dilation and acceleration of the microcirculation. Apart from giving the patient preparations to dilate the end-arterial system, daily injections to anesthetize the → (T) stellate ganglion should be administered during the crucial fortnight. If treatment is started at once, the chances of a complete cure or at least of partial recovery of hearing are better than 90%. If treatment is begun 4 days after the sudden onset of deafness, the success rate drops below 65%. If treatment is started only 2–3 weeks after loss of hearing has occurred, there is little hope of substantial improvement. Tinnitus Tinnitus can often be successfully treated by injections intravenously (→ (T) intravenous procaine injections) and to the acupuncture points TB-17 (mastoid process), TB-22 (“gate of the ear”) and TB-18 behind the middle of the ear. Brand treated 96 patients by neural therapy to these three points, after 3 weeks of vasodilator and vitamin A treatment had produced no improvement. He used segmental treatment only, injecting the acupuncture points described in (2) above but leaving out the important injection to the stellate ganglion, the intravenous injection, and any treatment of the cervical spine or interference fields. In one to six sessions he achieved 7.9% complete freedom from symptoms, 32.9% substantial improvement, 34.2% some improvement and only 25% showed no change. These three points are therefore recommended as the basic treatment for tinnitus. If this proves inadequate, a number of other possibilities remain available to us. One form of tinnitus is often described as being like the ticking of a clock. This is caused by nystagmuslike muscular twitching of the tensor palati muscle and occurs at the same rhythm as the ticking that the patient hears and which is macroscopically visible. It closes the walls of the eustachian tubes. Treatment 0.5 mL procaine to the → (T) nerve-exit points at the greater palatine foramen, to the → (T) stellate ganglion or to the Gasserian (otic) ganglion (→ (T) mandibular nerve). Through the latter we also reach the branch of the pterygoid nerve that contains fibers for the tensor tympani muscle. That has nothing to do with the Gasserian (otic) ganglion directly. There is also a vertebragenic form of tinnitus. This originates in the cervical spine and is a symptom of the → vertebral artery compression syndrome. There is also such a thing as neurovascular tinnitus. This is vertebragenic, originates in the cervical spine and is associated with the → vertebral artery compression syndrome. Vertigo In otogenic vertigo, in addition to the injections described in (1) and (2) above, we also try an anesthetic of the greater auricular nerve. This is found below the mastoid process, where it reaches the surface about the middle of the lateral edge of the sternocleidomastoid muscle. It is often palpable there as a hyperalgetic point. Eclampsia, pre-eclampsia According to Knaus, eclampsia is the result of a neurovegetative circulatory disturbance provoked by overdistension of the uterus, producing ischemia of the renal cortex and of the cerebral vessels by reflexes via the autonomic nervous system. These disturbances occurring as spastic vascular impulses are treated by injections into the → (T) stellate ganglion and splanchnic anesthesia → (T) celiac ganglion. Headaches, dizziness, and impaired vision, especially in pre-eclampsia before breakdown, disappear very strikingly and blood pressure is definitely lowered. Where eclampsia has already occurred, → (T) peridural anesthesia given in addition is even better able to set diuresis in motion. In the light of Knaus’s theory, injections into the → (T) pelvic region and → (T) Frankenhauser’s ganglia should also be borne in mind. Ecthyma Local infiltrations, possibly also intra- and periarterial injections into and around the → (T) femoral artery. See also → skin. Eczema If the treatment suggested under → skin is not effective, try naturopathic methods such as fasting, Kneipp’s therapy, baths, bloodletting, autohemotherapy, normalization of intestinal flora, → (T) Ponndorf’s and Baunscheidt’s vaccinations etc. Once the regulatory block has been removed by these means, neural therapy can be more successful. In infantile eczema, only an interference field can provide the answer: umbilicus, ears, tonsils? Edema Any edema is always a visible sign of disturbed neural regulation with increased capillary permeability. Procaine (but not lidocaine) seals the capillaries. If it is not caused by a cardiac or renal condition or due to an interference field, it generally responds well to local procaine treatment with → (T) quaddles. Muschaweck confirmed the anti-phlogistic and capillary sealing effect of procaine, which he believes stems from its fission products p-aminobenzoic acid and p-aminosalicylic acid. Encouraged by the example of acupuncture we set these quaddles also in the lower third of the leg over the posterior → (T) tibial artery (→ Fig. 3.6, Part III). Deeper injections intra- and para-arterially can increase the effect. In the case of post-traumatic edemas of the upper extremities we anesthetize the → (T) stellate ganglion. Ankle edema in women often disappears following repeated injections into the → (T) pelvic region. Post-thrombotic edema → thrombophlebitis. See also under → heart, → cerebral edema, → kidneys. Edema, angioneurotic → angioneurotic edema. Edema, cardiac → heart. Edema, cerebral → cerebral edema. Edema, facial, persisting after erysipelas → (T) stellate ganglion. Ejaculation, premature (ejaculatio praecox) If, as is often the case, the prostate is enlarged and pressure-sensitive, inject to or into the → (T) prostate and the → (T) pudendal nerve. With nervous predisposition showing signs of autonomic hypersensibility additional injections into the → (T) thyroid are indicated. See also → sexual disturbances. Elbow → joints, → periosteum, → epicondylitis. Elephantiasis → lymphedema. Embolism → vascular occlusion. Emphysema → lungs. Encephalitis In addition to antibiotics, procaine intravenously (→ (T) intravenous procaine injections) and under the → (T) scalp will help to eliminate the attendant symptoms and act as a prophylaxis against consequential damage. In severe cases and with later sequelae, inject into the → (T) stellate ganglion or superior cervical → (T) ganglion. Encephalomalacia Procaine intravenously (→ (T) intravenous procaine injections), under the → (T) scalp and injections into the → (T) stellate ganglion or the superior cervical → (T) ganglion. Encopresis Unintentional bowel movement can be reduced by a series of→ (T) epidural infiltrations. Endangiitis, endarteritis obliterans → neurocirculatory disturbances. Endocarditis → heart. Endometritis → pelvis. Enteritis, necrotizing Procaine intravenously (→ (T) intravenous procaine injections) and into the abdominal → (T) celiac ganglion and → (T) preperitoneal infiltrations at pressure-sensitive points. Enuresis nocturna Incontinence of organic etiology, e.g., due to epilepsy, mongolism, and idiocy must be excluded from treatment. Primary enuresis is caused by instability and hyperactivity of the muscles that are responsible for urination. The function of the Barrington reflex arc is not completely developed. Centrally and segmentally caused innervation disturbances of the bladder’s sphincter mechanism can generally be eliminated with ease and striking success by neural therapy. We set four to six → (T) quaddles into the Head’s zones over the sacrococcygeal region. The old-style pediatrician believed that to cure this disorder anything that impressed the child sufficiently would help. Perhaps the fear of pain in our treatment is, on purely psychological grounds, at least partly responsible for its success. It must be repeated immediately as soon as its effect begins to wear off. If the parents reject injections, we set some → (T) Ponndorf’s vaccinations over the sacrum. If these are not successful, at least in the case of older children, an → (T) epidural injection into the sacral hiatus is a promising approach. When searching for an interference field, the infiltration of the navel (the first → (T) scar of every human being) can show its causal involvement in the urination disorder. In addition, the tonsils may play a causal part. A combination of this therapy with time-tested tricks taken from child psychology can never do any harm. For example, the child is given a candy, not in the evening before going to bed but in the morning if the bed is dry. The calendar is then marked with a colored circle instead of the black mark, which indicates failure. Such bookkeeping must be shown from time to time to all the visiting people that the child respects, particularly to “uncle doctor.” Praise encourages. The suggestion should be made constantly to the child that it will in future wake automatically when his or her bladder is full. Capitulation and simply letting matters drift are as mistaken as severe punishment. Deep sleep must be interrupted by the waking reflex when the bladder is full, and this reflex must first be produced by conditioning the subconscious. Epicondylitis In addition to the procedure described in → periosteum for dealing with the diseased periosteum itself, it is always necessary to find any fibrositic nodules by palpation of the adjacent musculature and to infiltrate these. The most painful point is located above the head of the radius. Lateral humeral epicondylitis or “tennis elbow” is a tendopathy at the insertion of the carpi radialis and extensor digiti communis muscles. If the tendon insertions of the medial side are effected, it is called “golfer’s elbow.” Epicondylitis may be the result of → ostechondrosis or → cervical syndrome. Irritation of the cervical sympathetic chain is treated with anesthesia of the → (T) stellate ganglion. See also → joints (elbow-joint syndrome). Epidemic parotitis, post-operative parotitis In mild cases, this is cured rapidly after administration of a neural-therapeutic preparation intravenously (→ (T) intravenous procaine injections) on the affected side and by → (T) quaddles over the gland. In more severe cases, periglandular infiltration and, the most effective treatment, anesthesia of the stellate or the → (T) Gasserian (otic) ganglion. Following parotitis, the parotid gland can turn into an interference field. To test and eliminate, insert the needle at the root of the earlobe and infiltrate fanwise into the gland over the masseter muscle. See also → neuralgia of the auriculotemporal nerve. Epididymitis As in any → inflammation, set → (T) quaddles locally over the affected area. In the highly acute state, additionally inject 1–2 mL to the spermatic cord and first wait to see what effect this has. If necessary, then inject another 1 mL to and into the palpable swelling of the epididymis, using a very fine needle. In chronic cases that do not respond adequately to this treatment (and when gonorrhea can be excluded), try injections into the → (T) prostate, to the → (T) pudendal nerve, or → (T) epidural infiltrations. Epilepsy 1. Idiopathic epilepsy: Genuinely hereditary diseases cannot be cured by neural therapy. In idiopathic epilepsy there is permanent brain damage. This is the cause for the convulsive tendency that is liable to become autonomous and automatic. From Speransky’s experiments we know that any point in the brain may become an epileptogenic interference field. Once convulsions have started, they can go on automatically and even the surgical removal of the primary focus will no longer have any effect. Apparently, in an attack, electrobiological voltage differences are discharged as in a thunderstorm, which cannot be brought back into equilibrium by physiological means. Since in most cases the physician does not know whether the patient is suffering from a hereditary or an acquired form of epilepsy, an attempt at treatment in doubtful cases is always justified. Treatment has shown that, in addition to the autonomous brain damage, there are also peripheral epileptogenic zones that are accessible to us. By treating these we are often able to reduce the number and severity of the attacks substantially. If, for example, the first attacks began with the first period, we inject the → (T) pelvic region. If they started shortly after a surgery or smallpox vaccination, we try the corresponding → (T) scars. In cryptogenic cases, in addition to the → (T) intravenous injections and injections under the → (T) scalp, we also try injections to the appendix, tonsils, etc., in order to reduce the internal stresses and with them the susceptibility to such attacks. It is important not to become irritated or discouraged by an attack that happens the day after we have treated the patient. An attack that is already on the way will still occur. It is essential to keep a detailed record, showing severe and minor attacks separately, to tell us whether an injection has produced more prolonged spells free from attacks or with relatively fewer or less severe attacks. 2. Traumatic epilepsy: The treatment of what is known as Jacksonian epilepsy is a substantially more favorable field for our efforts. As an example, let me quote a case in my experience. Mr. K. S. was shot in the head in 1914. For the next 40 (!) years, he suffered headaches totally resistant to all forms of treatment, and major epileptic attacks without aura three to four times a week. After only four treatments, at first weekly, then at longer intervals, with procaine intravenously (→ (T) intravenous procaine injections) and under the → (T) scalp, and under the scar down to the periosteum, he has remained completely free from symptoms or attacks for 15 years. In this time, he has become noticeably more agile mentally. Where an aura is present, it is possible to intercept epileptic attacks by injections into the → (T) stellate ganglion. Apparently it is possible by this means to eliminate the convulsive impulses to the innervation of the cerebral vessels. However, I have some doubts from a medical point of view on the advisability of completely suppressing a discharge when it is due. Case History 23: B. G., Aged 10 Ten-year-old B.G. from Roßlau had torticollis surgery when she was 6. The surgery caused a “non-sensitive” scar behind the left ear. One year later she began having epileptic seizures. Initially the seizures came every 2 weeks. Within the next 3 years they recurred with increasing frequency (every 3 days) and intensity, finally reaching grandmal seizures. They always occurred at night after going to bed and began with tingling of the left arm, followed by spasms, which lasted up to 5 minutes. During the next day she was always too exhausted and tired to attend school. In the course of 7 weeks, I removed the interference behind the ear three times. The seizures disappeared, medication was discontinued, and the treatment terminated. Follow-up period. The patient is now 35 years of age and in the last 25 years she has been without seizures. She has three children, 3, 9, and 15 years of age, who have never suffered this sort of disorder. This is a case of traumatic epilepsy, caused by an interference field originating in a surgery scar behind the left ear. 3. Status epilepticus: It is generally known that local anesthetics in large doses produce convulsions. In subconvulsive doses, however, they generally have an anti-convulsive action without having any side-effects on consciousness, as is the case with the barbiturates, which were used previously. About 80% of grandmal and Jacksonian epileptic attacks react promptly to the → (T) intravenous administration of 2–3 mg/kg of body weight of lidocaine (Xylocaine), injected over 30–40 seconds. If the epilepsy responds to the lidocaine, the attacks end within 30 seconds to a minute. The effect persists for about 20 minutes. If the attack recurs, it is advisable to change to an intravenous drip in a physiological saline or glucose solution, with an hourly dose of 6–8 mg/kg (never exceed 10 mg/kg per hour!). Example: 8 mg × 70 kg body weight 2 hours = 8 × 70 × 2 = 1120 mg lidocaine; 1000 mg equals 50 mL of 2% lidocaine (without adrenalin!). The infusion should be continued for 2– 3 hours after the last attack. If it is continued beyond 5 hours, a long-acting barbiturate should be injected intramuscularly (→ (T) intramuscular infiltrations) at 2-hourly intervals at the rate of 2 mg/kg body weight, in order to subdue cortical excitation. In rare cases, an overdose can produce convulsions. In this event, a short-acting barbiturate (e.g., 30–50 mg thiopenthal) is given intravenously. This should always be placed in readiness when lidocaine is administered intravenously. Episcleritis → eye disease. Epistaxis → nose. Erysipelas Infiltration with procaine at an early stage will definitely prevent the erysipelas from progressing further, since it can only develop because of autonomic disturbances with local depolarization and consequent reduced autonomous defense by the body itself. In critical cases, if antibiotics do not suffice, injections into the regional → (T) sympathetic chain and its → (T) ganglia can save the patient’s life. By these injections we revitalize the cardiac efficiency and the reduced autonomic tone. Blood supply is improved, metabolic waste products are eliminated more rapidly and the defensive capacity is increased. By this means we not only combat the bacteria but also reduce the irritation they have produced to a safe level, where the regulating mechanisms can again cope with it. Erythrodermia → skin, → neurocirculatory disturbances. Erythromelalgia The symptoms are painful attacks resulting from active vascular dilatation, particularly affecting the legs of elderly people and due to bed warmth. Anesthesia of the lumbar → (T) sympathetic chain restores balance to the disturbed perivascular nervous system. If necessary, a local anesthetic may also be infiltrated into the affected tissue areas. Erythromelalgia may be caused by diabetes mellitus, thromboangiitis obliterans, or polycythemia. If so, this condition must be treated appropriately at the same time. Erythroprosopalgia Unilateral headache due to neurovascular disturbance: → Bing-Horton syndrome, → headache, → migraine, → neuralgia. Esophageal stenosis First exclude cancer! If there is spastic stenosis, → (T) quaddles at segmental level on both sides of the sternum and the thoracic spine (T5 through T8). Or injection to the → (T) stellate ganglion or → (T) paravertebral anesthesias in the area of T5 (through T8), vagus → (T) nerve, interference field? Ethmoid cells, disorders of → nose. European adder bite In addition to the common proximal stasis and wound expansion, the easiest and best treatment for → snakebites consists in generous injections around the site of the bite with 1–2% procaine, ideally within the first half-hour after bite. Treatment is repeated if necessary until the “toxic” symptoms have vanished. → (T) Intravenous injections are given for → shock prophylaxis and rapid reversal of the circulatory disorder. Reports from all around the world confirm this approach. If available, the patient should be treated with the serum. See also → snakebite. Exophthalmic goiter → thyrotoxicosis. Exophthalmos → eye disease. According to Russian ophthalmologists, an 8 mm exophthalmos disappeared within 2 days after a dental extraction. F. Huneke described a similar cure from a thyroidectomy scar and another by injections within the segment. Therapy If the cause cannot be found and there is no contraindication try injections to the → (T) stellate or ciliary ganglion. Extrapyramidal spasticity → spasticity, extrapyramidal. Extrasystoles → heart, → thyroid. Eye disease F. Huneke’s statement that “Impletol attacks inflammatory conditions at the root of their being, no matter what the noxious agents may be called which have caused the inflammation” shows that segmental treatment with procaine is indicated for all inflammatory eye conditions. And most eye disorders are inflammatory in their acute phase, in which the fate of the eye is decided, whether we are confronted with neuritis of the optic nerve, retinal periphlebitis with vitreous hemorrhage, scleritis, keratitis, iridocyclitis, or even cases regarded as being due to a rheumato-allergic cause such as suspected tuberculosis of the eye. Misgivings about the use of Impletol near the eyes on account of its caffeine content are unfounded. The caffeine in this product is in a complex compound and is never contraindicated, not even in glaucoma. Obviously, neural therapy should always be started as soon as possible, before the possibility of regeneration and recovery of the eye’s functions has been lost and cicatrization has occurred. Any major eye surgery and prolonged cortisone treatment can only reduce the chances of success for neural therapy. Atrophy of the optic nerve and blindness do not occur if a retrobulbar neuritis of neural origin is cured in time by segmental treatment or by the elimination of the interference field responsible. The eye is not an isolated organ but part of an entity that can receive interference impulses from any part of the organism, and these can produce a disorder. No further hemorrhage or scar formation will occur in a periphlebitis of the retina, if the interference field causing it, located, for example, in the pelvis, is eliminated by appropriate treatment with procaine. The eye specialist forever staring through a tube at his or her specialist organ who forgets that a human being is still attached to the eye will never be able to cure such a disorder and must helplessly “treat” the eye to the bitter end. A great deal of suffering could be avoided if eye specialists learned to eliminate inflammatory conditions with procaine and to give any failures of segmental treatment the benefit of a skilled search for the interference field responsible (Case Histories 6 and 24). A good indicator for the effectiveness of injections is the rapid disappearance of pain in inflammatory changes of the eyes or in intraocular increases of pressure. For segmental treatment, the following injections are available to us: 1. As basic treatment, we have the → (T) intravenous injection on the side of the disorder, and where both eyes are affected, alternating administration of this injection left and right. It counters inflammation, improves the blood supply, eliminates edema of the retina, reduces allergic reaction, relieves pain, and reduces capillary permeability. 2. → (T) Quaddles over the temples at the lateral orbital margin and deeper injections down to the periosteum. Possibly also → (T) intramuscular injections of 0.5 mL into each of the temporal muscles, especially if there is any pressure-sensitive area there. Head’s zones for the eyes are in the region of the neck, the occiput, and the ears (C1 and C2). Any hyperalgetic points found there by palpation should always be treated by quaddles and deeper injections under the → (T) scalp down to the periosteum. 3. Injections to the → (T) nerve-exit points of the supraorbital nerves, particularly if these are pressure-sensitive or if the condition is accompanied by frontal headaches, in conjunctivitis irrespective of etiology, blepharospasm, herpes, and corneal ulcer. Hyperalgetic points found by palpation of the head must also be treated. 4. Injections to the ciliary and the → (T) pterygopalatine ganglion have proved especially valuable. The eye is supplied with its autonomic fibers by complex pathways via these ganglia. The intraocular pressure, for example, is controlled autonomically via a ganglionic cell system of the choroid membrane, which is regulated and controlled via the ciliary nerves and ganglia. 5. Injections to the → (T) stellate ganglion can also produce the turning point, since this, of course, innervates the upper quadrant of the body. 6. In eye disorders that tend to be therapy-resistant such as glaucoma, iritis, ophthalmic herpes zoster, and painful corneal disorders, an injection to (but not into) the → (T) carotid or vertebral arteries can likewise take us a long step further. 7. In cases of deep-seated keratitis and episcleritis, subconjunctival injections of 0.5–1 mL of procaine can be useful. 8. If segmental treatment yields no results, search for the interference field! In folk medicine, the premolars of the upper and lower jaw are called “canine teeth” (Cases Histories 6 and 24). If the disorder is unilateral and other circumstances indicate this as advisable, a → (T) cisternal injection should also be considered. Fuchs reported on the results he obtained with the injection to the ciliary and pterygopalatine ganglia described in (4) above. These ganglia supply the eye with its trophic nerve fibers. He used these injections especially for treating chronic disorders of the anterior parts of the eye, i.e., eyelids, conjunctiva, and particularly the cornea, “primarily those which to date it was not possible to treat by other modern methods. In other words, these were eyes that without neural therapy would go blind due to complete parenchymatous degeneration of the cornea or that might even be totally destroyed and require enucleation.” In these selected cases, for which the prognosis was distinctly unfavorable, he was able to achieve 45 cures out of a total of 71 patients, and obtain 11 improvements! There was no change in only 10, and five became worse. For an experienced neural therapist there is little doubt that a skilled search for an interference field would have yielded success in at least some of those classified as failures. The eye specialist is in the happy position that he or she can read the effect of his or her procaine injections into the two ganglia directly in the superficial and deeper-lying vessels of the conjunctiva and sclera. In the split-lamp microscope, he or she can follow the way the cloudy cornea clears as a result of decongestion of the parenchymatous fibers. Even the swollen fibers of the corneal nerves can be seen to become smaller, until they disappear entirely. Blepharitis Injections to the nerve-exit points of the lateral and medial supraorbital nerves or infraorbital nerve of the diseased side. In the case of severe blepharospasm, the temporo-zygomatic ramus of the facial nerve has to be treated several times with local anesthesia. This is done by injection below the mastoid process and infiltration one or two fingers’ breadth toward the infra-orbital margin. Cataract In the early stages of clouding of the lens, regression is usually still possible by means of neural therapy. A massive, ripe gray cataract, however, is a completely cicatrized terminal state in which the organism’s self-healing capacity can only rarely change matters for the better even with outside help. Senile cataract can remain stationary for years, even decades, and may even improve spontaneously. This benign tendency justifies us in trying neural therapy where the condition has not progressed too far. Choriorenitis If the specified injections do not bring improvement, the search for an interference field is indicated (teeth, tonsils, etc.). The incompatibility with contact lenses can often be removed by repeated injections to the maxillary → (T) nerve (Vill). Corneal ulcer and keratitis therapy Ciliary and → (T) pterygopalatine ganglion. See → Sjögren syndrome. Dacryocystitis In the case of an inflammation of the tear sac, a short and thin needle (size 18 or 20) 0.5– 1 cm is inserted cranially to the medial corner of the eye, moving dorsal-medially until the resistance of the orbital septum can be felt. Here, 1 mL is injected, the needle slightly retracted and another 0.5 mL are injected medially toward the bone. A third subcutaneous injection of 0.5 mL is placed 1 cm inferior and slightly medially to the corner of the eye. After that, the area of the injection receives gentle pressure to disperse the local anesthetic around the tear sac. Glaucoma Locally administered beta blockers (e.g., retrobulbar procaine) can lower the intraocular pressure by 35–50% for at least 24 hours by reducing fluid production. The intraocular pressure is determined by the amount of fluid that is produced in the ciliary epithelium of the posterior ocular chamber and by the ease with which it can drain out. The lens and posterior cornea are nourished by intraocular fluid and not by blood. The composition of the fluid depends on the condition of the walls of the intraocular blood vessels. The episcleral plexus communicates with the Schlemm canal. Increased pressure in the plexus causes a backlog, which obstructs drainage of the intraocular fluid. If the osmotic pressure of the blood falls, the intraocular pressure rises. The autonomic reactive position is one of the determining factors of intraocular pressure. Repeated injections are required only until the computer represented by the ganglionic cells has learned to keep the pressure constantly regulated at the correct level. Vascular congestion of the ciliary body is the result of a block in the vascular regulating system. Anesthesia restores the disturbed circulation, thus relieving congestion and reducing pressure. In the case of an acute congestive glaucoma, any physician can provide relief by injecting procaine intravenously to the → (T) ciliary and stellate ganglion. This reduces intraocular pressure until treatment by a specialist is available. Ophthalmic herpes zoster This reacts well to injections into the exit point of the supraorbital nerve in the supraorbital notch. Dammer reported on 80 cases treated successfully by this method. A second injection proved necessary in only four or five cases, 2 or 3 days after the first. Squint For treating squint, we make several test injections into the → (T) ciliary ganglion on the affected side and into the hypertonic eye muscle. Several cases of squint that presented following diphtheria or scarlet fever were cured via the Huneke phenomenon following injections into the tonsils, which were acting as interference fields. In geriatric eye conditions such as macular degeneration, an attempt to use neural therapy (with ample repetition) can often still be successful (Piotrovski). Case History 24: Truck Driver, Aged 35 L.W., a 35-year-old truck driver from Kirchseeon came to see me in 1973. All specialists, including the ones from the clinic for chronic eye diseases, gave the following diagnosis: since January of 1972 chronically recurring bilateral iridocyclitis, central iridocyclitic retinopathy on the left. In spite of ongoing treatment, including cortisone and tonsillectomy, no considerable change in the condition. The patient had to give up his driver’s license. Due to imminent blindness he began to study Braille and started to work with a guide dog. Therapy: The electro skin test indicated an interference field in the fourth tooth at the upper right. Its extraction by the dentist was of no consequence. Supposedly, the remaining teeth were NAD. A new electro skin test showed red discoloration superior to the right mandibular angle. Radiography that included this area showed a dislocated impacted wisdom tooth in the right lower jaw. It was located in the immediate vicinity of the mandibular canal. After removal of teeth 47 and 48, the condition of the patient improved considerably. Two months later, an abscess formed at the extraction site and was drained. It contained a copious amount of pus. The wound healed very slowly and required biological treatment (without antibiotics and sulfonamides). The eyes had become inflamed during the abscess formation. Now they improved and cleared up. After examination by specialists, the patient was allowed to work in his job as a truck driver. One year later, a clinical tampon drained from an abscess at the right mandibular angle. It had been forgotten during surgery. This was without any effect on the eyes. The patient was monitored for 11 years, without relapse. The true diagnosis including the cause: chronically recurring iritis and uveitis, due to an interference field caused by a dislocated wisdom tooth. Eyelid, spasmodic twitching of → (T) nerve-exit points supraorbital nerve. Facial neuralgia → neuralgia. Facial pains → trigeminal neuralgia; see Head’s zones for teeth in Chapter 1, Section C, Part I on Segmental Therapy. Facial paralysis → paralysis, facial. Facial spasm, facial tic → spasm, facial. Fat metabolism, disturbed → lipodystrophy, progressive. Fecal incontinence → encopresis. Feet, cold According to W. Scheidt, the transition segment S2 has a close relation to the segments L2 and C8. This explains why cold feet can cause inflammation of the bladder, kidneys, and tonsils: • In acute cases, a warm foot soak or alcoholic beverages can dilate the vessels and stimulate the blood circulation. • In chronic cases, we begin by setting → (T) quaddles all round the ankle and calcaneal region. Injections to the periosteum of the medial aspect of the calcaneum. Also try peri- and intra-arterial injections to and into the → (T) tibial and femoral arteries and to the adjacent fossa ovalis. In women, injections into the → pelvis. If necessary, injections to the lumbar → (T) sympathetic chain may help. See also → neurovegetative dystonia, → neurocirculatory disturbances, → geriatric disorders. Femoral neuralgia → neuralgia, femoral. Femur, fracture of the neck of, pain following Injections to the periosteum of the → (T) trochanter major. See also → fractures. Fever Health is not a static condition, but the product of continually active maintenance and restoration efforts by the vital regulating mechanisms. These spontaneous healing powers function cybernetically. Their most effective defensive weapons are the healing effects of inflammation and fever. Biologically oriented physicians regard fever primarily as a natural healing force reacting throughout the organism to effect a cure via the basic autonomic system. Modern medicine regards fever as a measurable disturbance in physiochemical areas and sees its main task in trying to normalize this totally and at once. To this end, chemotherapeutic preparations such as antibiotics and corticosteroids, which are all capable of saving the patient’s life in an emergency, are often used too soon, for too long, in too large doses. The routine use of these medications for the treatment of fever without positive indication for a bacterial infection constitutes an irresponsible interference with the body’s own → immune system. This has fundamentally altered the body’s reactive capability to defend itself. As a result, the evolution of many disorders has also changed. Whilst all these substances reduce the virulence of the micro-organisms involved, they weaken the body’s natural defenses to such an extent that the bacteria remain active even in their attenuated form and can establish interference fields and allergies. Perger and Pischinger demonstrated that chemotherapeutic substances, antibiotics, and corticosteroids substantially restrict or paralyze the reactive capability of the basic autonomic system. In other words, an acute → inflammation is transformed into a chronic process, which places the basic autonomic functions under constant additional stress and consequently creates a continual readiness to fall ill. An acute illness, which nature with sensible medical help used to be able to fight and cure from within, has now frequently become a disturbance that the medical profession fights with potent chemical weapons by what must in the long run seem an unbiological approach. The pay-off for the body’s natural defenses is now all too often that this prepares the way for infectious relapse and for new disorders, because by being repressed the disease has been transformed to a continually smoldering chronic state, which not infrequently gives rise to interference fields. Procaine reduces fever. In infections with high fever, an → (T) intravenous injection can reduce the patient’s temperature from over 39°C to normal within an hour. In some cases, this means can be used to arrest the illness in its initial stages, complete with all attendant symptoms. In colds, the early use of a → (T) nasal spray with a mucosal anesthetic often proves effective. See also → influenza. Fibrillation, ventricular → ventricular fibrillation. Fibromatosis, penile → penis. Fibrositic nodules At the beginning of every neural-therapeutic treatment, the well-lubricated skin needs to be thoroughly palpated! By doing so, we are frequently surprised to find hyperalgetic nodules and bulges in the subcutaneous connective tissue of the lateral neck, the neck-shoulder area, paravertebrally in the anterior thoracic area, and superior to the sacrum. Those are so-called fibrositic nodules (gelosen, myogelosen). This cannot be confused with → muscle spasms that loosen up during anesthesia, whereas fibrositic nodules remain unchanged. The latter can be primarily found in the corresponding reflex areas of chronic and degenerative processes. Their formation is explained as a fixed disorder of plasma colloids. Metabolic roughage and potential difference causes a transformation from fluid sol to pathological gel. According to Preusser, this is a constant regulation-disturbing strain for the basic autonomic system, which takes place on the pathways between the nerve and the cell membrane. The formation occurs on viscerocutaneous reflex pathways. Reciprocally, they can have a negative effect on internal organs, joints, and regulation systems on dermatovisceral pathways. They fulfill all requirements for interference fields. By localizing and treating these nodules, we can enrich our diagnostic and therapeutic knowledge. Therapy A fibrositic nodule will disappear simply by setting a → (T) quaddle directly above it. Larger amounts of nodules will soften and shrink. The tonus of the nodule environment will relax. If there is a muscular spasm, it will dissolve and the patient will report a general relaxation in addition to the local improvement. With considerable improvement of the circulation the pain vanishes. The effect is even greater if we inject some drops of a local anesthetic through the quaddle, 1 mm into the nodule, just like an → (T) intramuscular infiltration. This interrupts the disturbed reflexes, which have produced the fibrositic nodules and reverses the gel into the physiologic sol condition. If the treatment does not remove the nodules completely and permanently, any trigger may produce a recurrence of the condition. Thus, we have to record and control the location, number, and size of the nodules. For a differential diagnosis between fibrositic nodules and neuralgia, see → cervical syndrome. Fingers (Heberden disease) Polyarthrosis of the distal interphalangeal joints with dorsal formation of two pea-size nodules formed by bone and cartilage growth at the base of the distal phalanx. This should not be confused with gouty tophi that are rounder and more distant from the joint. Bouchard nodes are not separated into two nodes and are the periarticular dorsal thickening of the arthrotic proximal interphalangeal joint. Therapy Local injections in and around the → (T) joints or the Oberst method; also injections in the afferent → (T) subclavian or brachial artery and the afferent (brachial plexus, radial, median, or ulnar) → (T) nerves, possibly to the → (T) stellate ganglion. If this effort fails, one has to search for an interference field (tonsils, teeth etc.). See also → scalene syndrome. Injections into the fingers, especially the fingertips, are extremely painful, and the patient’s hand must therefore first be securely fixed. Fish-skin disease → ichthyosis. Fissures, anal → anal disorders. Fit, apoplectic → stroke. Flatulence → abdomen. Flora, intestinal → intestinal flora. Flu → influenza. Foehn disease This condition is the sign of autonomic tonus disturbance. It is usually accompanied by increased excitability and lowering of the stimulation threshold. Regardless of the individual situation, → (T) intravenous procaine solutions act to relax and reverse. In the majority of patients, however, balance is only restored by removal of an interference field. See also → neurodystonia, → thyroid, → weather susceptibility. Fox–Fordyce disease → skin. Fracture of the neck of the femur → femur, fracture of the neck of. Fractures “Following an injection into a fracture hematoma, the local anesthetic diffuses all the way to the nerve fibers supplying the soft tissues in the region of the fracture, and to the nerves of the bone and periosteum” (Eriksson). After skin disinfection, slowly inject 5–10 mL into the hematoma. After about 5 minutes, the fracture can be manipulated into position with relatively little pain. This method is recommended in emergencies. In minor fractures, e.g., ribs, fingers, toes, etc., first aid is given by injecting 1– 2 mL into the fracture site to provide immediate freedom from pain. Repeat after 2–3 days if necessary. In joint fractures and in fractures adjacent to joints but without dislocation (patella, olecranon, clavicle, upper end of humerus), infiltration around the fracture will promote early active movement and rapid healing without contractures or ankylosis. Animal experiments have proved conclusively that fractures treated with procaine or lidocaine heal better and more quickly. Procaine supplies the deficient voltage and restores the potential to normal, thus promoting the healing process. In poor → callus formation we also inject close to the periosteum near the fracture or, better still, directly into the fracture gap. This also reduces the risk of pseudarthrosis formation. Leriche recommended this treatment as long ago as 1928 and praised it for improving the blood supply and more rapid callus formation, which he was able to prove to result from it. Further, early procaine treatment of a fracture and its associated functional impairment is a reliable means of preventing the autonomic deviation of post-traumatic → osteoporosis. If callus formation is slow, if the fracture is painful for longer than the severity of the trauma seems to justify or if there is any other discrepancy between morphology and function, an interference field may be the cause. In such cases the fracture has allowed pre-sensitized regulating systems to deviate pathologically. We need always to bear in mind that any fracture site is a scar capable of becoming an interference field for other disorders. Frigidity → pelvis, → sexual disturbances. For anorgasmia and frigidity, Mink recommends the injection of 1 mL of procaine bilaterally → (T) preperitoneally about halfway between the symphysis pubis and the anterior superior iliac spine. Frontal sinusitis → nose. Frostbite The current standard treatment for local frostbite consists of the rapid rewarming of the frostbitten part to 43°C and the intravenous administration of dextran of low molecular weight. We add procaine to this. Procaine combats → shock and has a positive effect on everything to do with the blood supply. Stimulation of the blood supply is an urgent necessity and can best and most easily be achieved by “medical sympathectomy.” This is possible at a very early stage, as soon as the frostbite victim is found and/or during transport, and consists in procaine injections into and around the → (T) afferent arteries and into the sympathetic → (T) ganglia supplying the affected parts. These can be given immediately and without misgivings even to seriously injured patients. Procaine (but not lidocaine or mepivacaine!) dilates the vessels, seals the capillaries, and prevents the formation of → edema: 1. Upper extremities: Intravenously (→ (T) intravenous procaine injections), → (T) brachial plexus nerves, → (T) subclavian or brachial arteries, → (T) stellate ganglion. Fingers and toes: repeated infiltrations around frostbitten areas, also small doses for the Oberst method. 2. Lower extremities: Intra- and periarterially into and around the → (T) femoral artery and nerve, injection into the lower → (T) sympathetic chain and/or the root of the → (T) sciatic nerve. In third-degree frostbite of the lower extremities, injection into the lower → (T) sympathetic chain will noticeably promote demarcation, and injection into the → (T) stellate ganglion will do the same with regard to the upper extremities. The demarcation line is displaced distally by this treatment, i.e., severely damaged tissue whose fate is still in the balance and which would otherwise necrose will be saved. In the first stage of frostbite, injection into the sympathetic chain supplying the affected parts eliminates arterial spasm. In the second stage it restores vasomotor equilibrium, and in the gangrenous stage it extends collateral circulation. In follow-up treatment of severe frostbite, these injections relieve pain, circulatory disturbances, and hyperhidrosis. This was confirmed through experiences during World War II in Germany and the Soviet Union. See also → neurocirculatory disturbances, hypothermic shock: see page 211 (Gerecht). Frozen shoulder → periarthritis of the humeroscapular joint. Functional disorders We regard these as the preliminary step to organic disorders, which our insufficiently refined methods of investigation are not yet able to identify. We treat them as if we were dealing with an organic disorder. Fungus infections of the skin → skin. Furuncles Early treatment by infiltration of the surrounding healthy tissue rapidly relieves pain, demarcates necrosis, and allows the → inflammation to heal. In furunculosis, the site of the first furuncle often provides the clue as to which organ in the related segment is disturbed or acting as an interference field and thus weakening the defensive capability at the periphery. See also → abscess, → nose, →furuncles of the upper lip. Furuncles of the upper lip In serious cases, injections to the → (T) stellate ganglion can be life-saving. See also → furuncles, → erysipelas. Gallbladder, gallstones → abdomen. Ganglion Synovial cysts tend to form on the back of the wrist. As long as they do not seriously inconvenience the patient, they ought not to be treated. They may be eliminated by strong pressure or a blow. Procaine injection into the cyst can break up the cystic wall. But the cysts frequently recur. Surgery is a relatively major operation and offers no guarantee against a recurrence. The simplest therapy is paracentesis and aspiration of the ganglionic contents, followed by the injection of a procaine solution and a tight bandage for several days. Gangrene (diabetic, intestinal, senile) → intestinal atony, → frostbite, → neurocirculatory disturbances; → (T) femoral artery. Gastric crises → tabes dorsalis. In genuine gastric crises, local anesthetics are often ineffective, but an attempt is always worthwhile. Apart from tabes, a remote disturbance due to an interference field can produce the → abdominal symptoms. Gastritis → abdomen. Gastroenteritis, infantile As a supportive measure for the customary treatment, inject 0.5 mL procaine intravenously (→ (T) intravenous procaine injections) or l mL around the → (T) brachial artery, plus a → (T) quaddle over the → (T) epigastrium and passing through this down to the peritoneum. Where the patient’s life is at stake, inject into the abdominal → (T) celiac ganglion. Gelosa → fibrositic nodules. Genital pains → dysmenorrhea, → epididymitis, → pelvis, → sexual disturbances, → neuralgia, pudendal nerve, → prostate, → vaginismus. Geriatric disorders See also Chapter 3, Part I, Section C on Rejuvenation With Procaine. Procaine cannot rejuvenate a patient. But premature aging and physiologically abnormal degenerative symptoms of all kinds are a disease and must be treated like any other chronic disorder. Aslan, Marx, and others have shown conclusively that procaine, even administered at random, stimulates both male and female sex-hormone glands and the suprarenal glands, and consequently halts the degenerative involution processes of the sexual organs. By the revitalizing action of procaine, senile changes in the skin were consistently reversed. We generally give l mL of procaine intravenously (→ (T) intravenous procaine injections) as the basic treatment, and → (T) quaddles and deeper injections in the segment of the principal disorder, e.g., in cerebral arteriosclerosis under the → (T) scalp, in senile emphysema over chest and back, in aortic sclerosis parasternally, in micturition difficulties into the → (T) prostate etc. Injections into the → (T) stellate ganglion produce active vascular dilatation in the brain, relaxation of vascular spasms, and an improved supply of oxygen. As a result, the degenerative process is halted. Dystrophies are eliminated to the extent that they are still reversible. In consequence, the symptoms disappear and functional performance is improved. Improved circulation comes with a pleasant cosmetic benefit: the facial skin tightens and looks younger. However, the best-intentioned segmental therapy fails if an interference field causes an early decline. In some cases a series of injections to the → (T) thyroid can be helpful. Hoster pointed out that approximately 10% of people over 60 years of age suffer from a thyroid disorder. Hypothyroidism may be the result of atropic autoimmune thyroiditis. Because local complaints are missing, the condition is frequently labeled as a “sign of old age.” Indications include: unusual sensitivity to cold, edema around the eyes, non-specific “rheumatoid” complaints, immobility, fatigue, and changes that compare to dementia due to old age. Hyperthyroidism due to old age is hard to recognize: general weakness, hyper-kinesis, hyperhidrosis, and hypermetabolism with intense weight loss and lethargy, combined with tachycardia and arrythmia can be indicative. Diarrhea and hair loss are usually not present. In cases of nodular goiter, malignancy (using sonography, scintigraphy, needle biopsy) has to be excluded in older patients. The risks of surgeries increase in older people. Thus, indications for surgery have to be carefully evaluated. Senile gangrene see → neurocirculatory disturbances. Giant colon → megacolon. Gingivitis → periodontosis. Glaucoma → eye disease. Glomerular nephritis → kidneys. Glossodynia Exclude pernicious anemia, diabetes, vitamin B and iron deficiency. Inject a neural-therapeutic preparation to the lingual nerve, submucously to the retroglossal region, level with the third molar. Glossopharyngeal neuralgia Chewing, yawning, and thermal stimuli can produce attacks of neuralgia on the affected side of the neck and throat, in the pharynx, tongue, tonsils, and radiating as far as the ear. Pressure on the tonsils, the pillars of the fauces, the lateral wall of the pharynx, and the posterior third of the tongue produces severe pain. Treatment Injections to the → (T) glossopharyngeal nerve, or to → (T) tonsils and adenoids, the → (T) mastoid, and → (T) quaddles in the region of the base of the skull; also to the upper cervical or → (T) stellate ganglion. If the treatment is ineffective, find the interference field. See also → neuralgia, → neuralgia of the temporomandibular joint, → trigeminal neuralgia. Goiter → thyroid. Goiter, exophthalmic → thyrotoxicosis. Gonarthritis → joints. Gout Gout is ultimately the result of a regulatory disturbance that occurs in consequence of defective control in the autonomic centers of the diencephalon. The means described under → joints thus hold out good prospects of success in treating this disorder, since they tend to normalize defects of autonomic control if administered at the correct site. Of course proper nutrition and uricostatics are required. Gracilis syndrome See under → (T) obturator nerve. Granuloma annulare Infiltrate around and under the lesion. See also → skin. Graves’ disease → thyrotoxicosis. Greenstick fracture → fractures; → rib, fractures, cracks. Gynecological disorders → pelvis. Gynecological dysfunction, autonomic This neurodystonic disturbance occurs in 5% of all women and can account for half the patients attending a gynecological surgery session (Mink). It produces a regulatory paralysis that makes it impossible to change from a vagotonic to a sympathicotonic state and vice versa. The functional control defect presents the following leading symptoms: diffuse pain or discomfort in the lower or middle abdominal region. This is felt as a piercing or burning pain, an ache or soreness and appears to be uncontrollable. In spite of thorough examination, British gynecologists have reported no pathological findings in 63% of laparoscopies performed on women with complaints of chronic pelvic discomfort. They called it the “pelvic pain syndrome.” Merely varicose changes in the venous plexus around the uterus and the appendages were noted. This was interpreted as the result of a deviation by the autonomic regulation. The common disease picture manifests itself in the following cardinal symptoms: pain on moving the cervix and pressure sensitivity of the posterior wall of the pubic symphysis due to reflex hypertonus of the myometrium. Ropelike parametric processes, pressure-sensitive tight uterosacral ligament, and muscle spasms of the fallopian tubes and the uterus that cause dyspareunia can be detected. In addition, the previously mentioned venous insufficiency and persistent cervical hypersecretion can be found. Many of the patients will already have undergone unsuccessful laparotomy on that account, on one or more occasions. Congestive hyperemia, as a result, is wrongly interpreted as “chronic adnexitis.” “Complications with adhesions” are listed as the reason for further surgeries. Therapy In addition to the regular gynecological examination, we test for sensitivity of the abdominal wall, because non-specific complaints in the entire abdominal area can originate in hyperalgetic areas of the abdominal wall. We approach this situation with → (T) preperitoneal infiltrations. We consider autonomic gynecological dysfunction, the “disease with 21 names,” as a reversible functional disorder that can be treated successfully with regulation therapy. We give injections into the → (T) pelvic region and → (T) Frankenhauser’s plexus, with particular health history → (T) intramurally. Also, injections to the lower → (T) sympathetic chain and in and to the → (T) femoral artery can be considered. In the course of the treatment, the pain diminishes soon, the indurated ropy tissue softens, and the usually small and rough uterus is loosened up, because the hormonal regulation also depends on impulses of the neurovegetative system. If segmental therapy fails, one has to search for an interference field. See also → pelvis. Hair, loss of → alopecia. Hallux valgus, inflammation of Infiltrate around and under the inflamed area as far as the periosteum, and repeat once or twice weekly if required. This chronic irritation can act as an interference field! In testing scars it is important not to forget those left by surgery of a hallux valgus. Hay fever → nose. Headache Obviously, before starting treatment, the neural therapist must ascertain that the condition is not due to space-occupying cerebral lesions (Case History 1, Part I, Section C, Chapter 1). See also → neuralgia. The treatment of headaches is one of the classic domains of neural therapy. It is so reliable and effective in all headaches of functional or organic etiology that one is justified in suspecting psychogenic causes whenever it fails to provide complete relief! Therapy The standard treatment by which we can reduce the host of sufferers from chronic headaches consists of an → (T) intravenous injection of procaine or lidocaine, in conjunction with injections under the → (T) scalp. Intravenous injection is indicated in cases of causal or concomitant vasomotor dysregulation. In frequent vertical headache, an injection down to the periosteum at the temporal or parietal level on each side is generally adequate. A bony ridge can be felt two fingers’ breadths above the middle of the maxilla, which is usually pressure-sensitive. It is always advisable to palpate the head very thoroughly before giving these injections and to inject to any particularly painful points and into all → (T) scars found in the segment. Avoid proceeding by rote and blueprint! We generally find that the → (T) nerve-exit points above and below the eyes and at the back of the head (infra- and supraorbital nerves, occipital nerve: → (T) nerves [afferent]) are pressure-sensitive. In this case, we infiltrate them directly. If in sinusitis headaches the exit points of both the supraorbital nerves are sensitive, we generally also inject a few drops in the center to the root of the nose. These three points form the “anterior magic triangle” in acupuncture. Frontal headache is treated with a quaddle set two fingers’ breadth cranially to the root of the nose, superior to the horizontal line between the eyebrows. From there we infiltrate the area superior and parallel to the brows subcutaneously. We use 3 mL on the left and again on the right side. This disables both branches of the supraorbital nerve and the supratrochlear nerve, which supply the forehead up to the hairline. In headaches that affect only the temporal areas, usually accompanied by overtiredness and disturbed vision or pain behind the eyes, → (T) quaddles set approximately on a line connecting eye and ear and injections down to the periosteum of the temporal bone have been found to give relief. Occipital neuralgia presents with piercing, stabbing pains radiating from the neck up and forward over the dome of the skull. Again, the head should be thoroughly palpated before treatment and the injections accurately pinpointed on the pressure-sensitive points found. An isolated headache above the right eye can indicate a disturbance in the region of the liver and gallbladder, particularly, if they occur after the consumption of certain foods (such as chocolate, cheese, sausages). See also → abdomen. If the scalp is painful over a circumscribed area of the skull or on the crown when the hair is brushed or combed, the → (T) tonsils are often found to be the interference field. Some forms of → migraine respond well to a para-arterial injection of the temporal artery. This can be readily located at its exit point in front of the ear, just above the zygomatic arch. If the headache is the symptom of a ciliary → neuralgia, we have to inject into the → (T) ciliary ganglion. The leading symptom reported by patients is that “during an attack they feel like wanting to tear out their eye.” In other therapy-resistant headaches, where the injections described above fail to provide relief, injection into the stellate or superior → (T) cervical ganglion and to the → (T) vertebral artery will help. Headaches following concussion and hypotonic forms, e.g., after lumbar punctures, will be amongst the most frequent in this category. The cause of post-surgical headache after intradural anesthetic procedures is most likely the draining of CSF through the puncture into the tissue. Thus, the use of thick needles should be avoided. Some diseases will also respond to injections to the → (T) pterygopalatine ganglion or the mandibular nerve near the Gasserian (otic) → (T) ganglion, others will be relieved by injections to the → (T) nasal conchae or by local anesthesia with a → (T) nasal spray. A persistent headache can make life unbearable, especially when, as is so often the case, it is accompanied by severe insomnia. In such cases it is worth trying literally anything, and even a → (T) cisternal procaine injection may be justified. (Case Study 16, Part I, Section C, Chapter 2). Headache and migraine in women is often closely associated with the menstrual cycle and is then due to a hormonally conditioned sympathetic dystonia, which alters the autonomic state shortly before menstruation and changes the stimulus threshold, leading to increased pain sensitivity. Treatment consists in injecting into the → (T) pelvic region and → (T) thyroid. The former helps restore the hormonal balance and the latter serves primarily to reduce the patient’s autonomic hyperexcitability. In all forms of migraines and headaches, we begin to search for an interference field if segmental treatment fails. Hearing defects → ears. Heart Cardiac disorders can present with pain, pressure or burning sensations in the associated Head’s zones, by tightness in the chest, feelings of oppression, and anxiety states. The pain travels via the inferior cardiac nerve to the stellate ganglion, on to the thoracic ganglia, the communicating rami, thence via C3 to T4, to the spinal cord. The capillary spasm in the skin, which produces pain as a result of hypoxemia, can accurately mirror the circulatory disturbances in the cardiac region. Despite this, the severity and extent of the hyperalgetic areas do not always allow firm conclusions to be drawn as regards the seriousness and type of the organic disturbance concerned. According to statistics, some 40% of the total population between the ages of 45 and 50 have coronary sclerosis. In Hochrein’s view, the severity of sclerosis and the frequency and severity of angina pectoris by no means run parallel. According to him, only about 15% of all patients suffering from coronary sclerosis also have angina pectoris. In other words, major anatomical changes do not constitute the main factor in a heart attack. In the large majority of cases angina pectoris results from disturbed neurovegetative regulation of the heart. The hypersensitivity of the nervous system in the angina pectoris patient results in a lowering of the irritation threshold and hence in an abnormal increase in his or her proneness to spasm. Our task is to use neural therapy to arrest these abnormal reflex processes in the cardiac nervous system at an early stage and make them return to normal by using the normalizing effect of neural therapy. Any abnormal sensations in the region of the heart, the left clavicle, and shoulder should therefore be regarded as warning signals and be eliminated as thoroughly as possible at the earliest opportunity: 1. As basic treatment in all cardiac disorders we inject procaine or lidocaine intravenously (→ (T) intravenous procaine injections) into the left antecubital vein. Procaine is a beta blocker, which in addition has a quinidine- and sparteinelike effect on the heart in inhibiting the formation and transmission of irritant stimuli. Procaine also has an oxygen-economizing effect on the heart and is thus able to prevent angina pectoris attacks and cardiac arrhythmia caused by anoxemia. In severe cases, the injections can be given every half-hour. 2. The cutaneovisceral reflex zones of the heart are on the left side of the chest, to the left of the sternum, inferior to the left clavicle, over the left shoulder as far as the side of the neck, and along the arm, from the inside of the forearm to the ulnar side of the hand. On the back, they travel down to a point between the shoulder blades (C2 to C4, T1 to T6, left). We frequently find that the first acupuncture point on the heart channel (HT1) is unpleasantly pressure-sensitive. Starting from the upper end of the axillary fold, we go one fingers’ breadth cranially and thence medially to the nipple line. If this point is hyperalgetic, we inject there left and right. If the → (T) sternoclavicular joint is pressure-sensitive, it can cause pseudo-anginal complaints. This is another reason for extremely thorough inspection and palpation of the thoracic area before injecting local anesthetics in the case of heart disease! In cardiac pain, there is interaction between organ and periphery. This is often disregarded in therapy. The visceral and peripheral terminal vessels react jointly because they are linked together by segmental reflex-regulating complexes. We can improve the state of the peripheral vasomotor system by means of intradermal quaddles. If we repeat this treatment often enough we can eliminate these changes entirely. The positive cutaneovisceral reflex effect can then be seen in the ECG. From the left brachial plexus (→ (T) nerves [afferent]), pain radiates to the left arm, particularly to the region supplied by the→ (T) ulnar nerve. We have to palpate these skin areas thoroughly, together with their underlying subcutaneous tissue and the corresponding intercostal spaces, the ribs, neck, trapezius, pectoral, and neck muscles, and even the area around and along the spine, in order to locate any points that are especially tender. This is especially necessary if there is a history of fractures of the vertebrae or their spinous or transverse processes. Costovertebral and→ (T) sternoclavicular joints can produce disturbing impulses that sustain the symptoms. These algetic points have to be treated with → (T) quaddles and deeper injections, if necessary going down to the periosteum and pleura. The area to the right of the shoulder blade has to be palpated with particular thoroughness. Fibrositic nodules and hyperalgetic points can be frequently found in this area. A long-forgotten accident, with contusion of the sternum, the xiphoid process and the lower portions of the thorax, perhaps a sudden blow from the handlebars of a bicycle or the steering wheel of a car, can have left behind a state of irritation that may now be affecting the heart via osteovisceral reflexes. We need to question our patients closely about this, and examine and treat them accordingly. If the examination of the organs does not provide conclusive results, the case history gives an indication about the connection between the complaints and the skeletal system. The case history reveals the influence of body posture, certain movements, and positions on the complaints. As basic treatment we set two to four → (T) quaddles directly beside the sternum in the first to third intercostal spaces, over the pressure-sensitive points and further laterally into any fibrositic nodules found by palpation; these are often located between the ribs. If there is an increased and prolonged dermographic reaction on the left side of the chest, → (T) quaddles should also be set there and the → (T) thyroid treated. A further quaddle is set in the angle formed by the left lower edge of the thorax and the xiphoid process. If this point of the periosteum is found to be pressure-sensitive, it should also be injected. If an angina pectoris patient tells us that he or she has previously received a short, sharp blow in this region, we set an additional quaddle and also inject the → (T) epigastrium. The intravenous injection and the parasternal quaddles constitute our basic treatment in all cardiac disorders. We always use these first, generally to very good effect, irrespective of whether we happen to be dealing with an angina pectoris, pseudo-angina pectoris, valvular insufficiency, a disorder resulting from cardiac catheterization, an injured myocardium, syphilitic aortitis, or cardiac neurosis. In all suitable cases this treatment of Head’s zones effects a reflex improvement of cardiac performance, at the same time producing a dilatation of the coronary vessels. This benefits the pulmonary circulation and facilitates oxygen absorption. And this, in its turn, again benefits the heart. By treating the principal superficial hyperalgetic points, we thus also have an opportunity, as it were, of conducting the irritation, which causes the hypertonic heart muscle to go into spasm, from the deeper regions to the surface. The reactive improvement of the thoracic excursions also helps to reduce the precordial sensation of pressure. We cannot achieve any organic cardiac change by our therapy, but the heart’s functional performance becomes more economical as a result of it. All scars in the segment must be treated as hyperalgetic points, i.e., they must be injected at the same time. Special attention should be given to neck scars (e.g., from boils, carbuncles, injuries) and especially to scars on the left arm, hand, and above all the fingers! As the proverb has it: “Finger pain travels to the heart” (Case History 25). The most powerful weapon in our armory for the segmental treatment of the heart is the injection to the → (T) stellate ganglion. Autonomic innervation, i.e., functional regulation and pain transmission, take place via this ganglion. Experience has shown that the right stellate ganglion is more important than the left for the innervation and regulation of cardiac function, since more of the accelerant fibers pass through it (Schmitt). This is of particular significance for reducing the heart rate in cardiac rhythm disturbances, for example, paroxysmal tachycardia. In angina pectoris, anesthesia of the stellate ganglion can correct the sympathetic hyperstimulation and restore the disturbed autonomic control to equilibrium. Hypertension and increased heart rate are symptoms of increased sympathetic activity following coronary bypass surgery and can be prevented by pre-operative stellatum anesthesia on the right. In cardiac disorders, therefore, we always first inject the right-hand stellate ganglion and try the left only if this has been insufficient. The left may then be more effective. Care should be exercised in cases of cardiac and bronchial asthma bordering on the limits of decompensation, as there is then a risk of reflex cardiac arrest! There is an important rule that experience has taught us: if the heart responds unequivocally to strophantin and other glucosides, procaine will not help. On the other hand, 30–40% of strophantin-refractory cases react promptly and convincingly to procaine given intravenously (→ (T) intravenous procaine injections) together with parasternal → (T) quaddles. Fig. 2.5 Segmental therapy in cardiac disorders, anterior aspect. Any diagnosed myocardial infarct should be treated only in hospital. But according to Hochrein, 40% of all cardiac infarcts are symptomless. During an acute myocardial infarction, ventricular fibrillations endanger the patient’s life during the first 4 hours. Even before transporting the patient to the hospital, every physician should instantly administer relative high doses of local anesthetics intravenously in an effort to remedy this critical situation. Taking 1– 2 minutes, 3–5 mL of a 2% procaine or 1% lidocaine solution are given intravenously through an indwelling catheter. If effects subside, the injection may be repeated one to three times every 5–10 minutes. The therapeutic effect of this intravenous pre-injection prevents or stops ventricular fibrillation and tachycardia immediately. In an experiment, Bezold and Jarisch were able to prevent a collapse induced by veratrin poisoning, which is the clinical equivalent to a myocardial infarction, by injecting procaine intravenously (Hirsch). To cover the time of transportation to the hospital, 20 (–40!) mL of the longer-lasting 1% lidocaine was administered intramuscularly (→ (T) intramuscular infiltrations) to the left deltoid and trapezius muscle. Contraindications: severe conduction defects, such as arteriovenous blocks (I-II) III, bradycardia, cardiac decompensation, and liver and kidney insufficiency. The arteriovenous block and bradycardia need to be considered alarming symptoms. In the case of posterior myocardial infarction we give additional injections into the → (T) epigastrium and set quaddles next to the sternum and above the angle formed by the xiphoid process and the inferior thoracic margin. In the case of lateral myocardial infarction we inject prepleurally to the left of the sternum. If pain in the forearm or fingers is present, we inject to the nail fold of the fourth and fifth finger. If the patient complains about shoulder pain, we inject to the pleura of the first intercostal space inferior to the left clavicle or to the cervical plexus (→ (T) nerves [afferent]). Fig. 2.6 Segmental therapy in cardiac disorders, posterior aspect. To re-establish normal autonomic regulation quickly, Leriche, Huneke, Schmitt, Siegen, and other authors explicitly recommend anesthesia of the → (T) stellate ganglion, even in the acute stage of the myocardial infarction. Hyperactivity of the sympathetic nervous system causes increased cardiac activity, which expands the area of infarction. The pain that is caused by the infarction can be eliminated through anesthesia of the stellate ganglion. In careless patients, this opens the door for re-infarction because they do not rest enough or overload themselves too soon. Killian warns against stellate injections in the acute stage. His concern is the deactivation of accelerator fibers. If a patient who presents with anginous complaints is treated with injections, the CPK values (ceratinphosphokinase) are unstable during the following days. The values are increased for lesions of the peripheral and cardiac muscles. If necessary, the relevant iso-enzymes have to be determined in order to clarify the situation. As a first-aid measure in recurrent coronary spasms, the patient should be advised to pinch the skin over the site of the pain firmly between two fingernails. The fresh, sharp pain seems to drive off the old and less severe one. This ancient piece of empirical lore about segmental reflex reaction has now been given a modern label, acupressure. Ventricular cardiac arrhythmia and fibrillation often occur in conjunction with myocardial ischemia, particularly in myocarditis and cardiomyopathy with vascular occlusion. Further factors that may produce these are cardiac catheterization, mechanical irritation, and hypothermia in cardiac surgery, and electrolyte disturbances (hypokalemia) after prolonged use of diuretics, especially in conjunction with digitalis. The excellent results obtained in the prophylaxis and treatment of such ventricular arrhythmia by giving procaine and other local anesthetics (Xylocaine, Scandicaine, Xyloneural etc.) intravenously (→ (T) intravenous procaine injections) is explained by the fact that the local anesthetic acts as a beta blocker and fends off the excessive impulses from the sympathetic system, thus reducing excessive oxygen demand. As the labile cell membranes are stabilized, the formation and transmission of irritant stimuli is inhibited, cardiac rhythm is made more regular and cardiac performance becomes more economical. In other words, the stimulus threshold of the myocardium is raised and the risk of infarction therefore reduced. In cardiac arrest: oxygen, artificial respiration, external heart massage, pacemaker, possibly procaine intracardially; the injection has to reach the left ventricle. Injection with 10 cm needle to the left of the xiphoid process sagittally, 9 cm deep; follow with 10% calcium chloride (→ Table 3.4, Part III). In tachycardia of uncertain etiology, try an injection into the → (T) thyroid, or intravenously (→ (T) intravenous procaine injections) and chest → (T) quaddles. Alternatively, an injection to the → (T) stellate ganglion is usually effective. See also → cervical syndrome. In endocarditis, always arrange for a dental status and treatment urgently. In women who present not only with a stenocardial disorder but also with → dysmenorrhea, treat only the → (T) pelvic region. The cardiac and circulatory disturbances will vanish with the dysmenorrhea. Interference fields cause approximately 30% of all cardiac disorders! We can only help if we locate and eliminate this noxious influence! Where neural therapy remains ineffective, the heart condition may have a psychogenic origin, or its cause may be vertebral (→ cervical syndrome). Chirotherapy may possibly help in such cases. Case History 25: Opera Singer, Aged 54 The 54-year-old renowned opera singer R. Sch. from Starnberg suffered a myocardial infarction during a beach vacation in 1969. On the day of the incident, in spite of being plagued by angina, he went swimming in the ocean, went for a run along the beach, played tennis, and went to the sauna. Obviously, even for an athletic person, that was a bit much all at once. There is too much of everything – even health! He was transported to an ICU by helicopter, which saved his live, and went through rehabilitation at a clinic for heart disease. The rehabilitation was not entirely successful and he was unable to work again. His autonomic regulation system was unable to compensate environmental stressors, such as changes in temperature and altitude, foehn wind and humid weather. Under these conditions he suffered from unpleasant anginose discomfort. Therapy: The standard treatment, including intravenous injections and quaddles above the sternum and fibrositic nodules and even stellate injections brought no improvement. Testing the tonsils and devitalized teeth was without useful result. During the fourth treatment, anesthesia of a painless scar at the fifth finger, remnant of a Dupuytren surgery, caused a lightning reaction. I was petrified when he told me that he had gone right after the treatment (during humid weather) for several runs up and down the Isar embankment to test his newly regained vigor. He was able to perform as a tenor again and without relapse. In the course of 14 years of follow-ups, he participated with great success every year in celebrity ski races. The neural-therapeutic diagnosis is: condition after myocardial infarction and angina pectoris episodes caused by segmental interference field scar at the fifth finger on the left.
Encylopedia of Neural Therapy
Introduction
Facts to Remember
Symbols Used in the Text
Alphabetical List of Conditions and Indications
A Necessary Foreword
Alphabetical List of Conditions and Indications
A
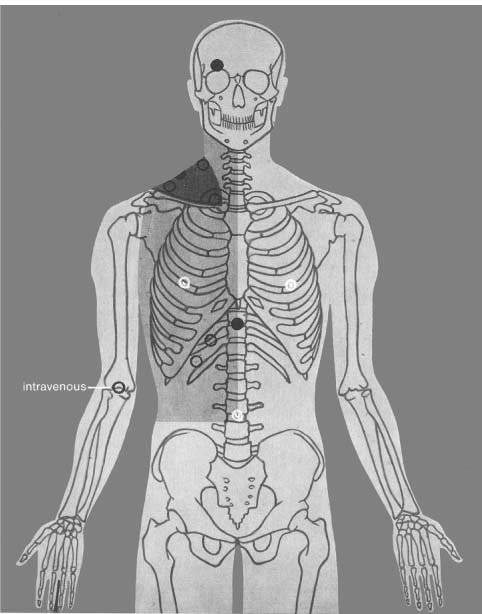







B
C
D
E
F
G
H



Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree









