SECTION VI DIAGNOSTIC AIDS
CHAPTER 22
Imaging of the Brain
Brain imaging provides essential diagnostic information and is very useful for research on the brain. Images of the skull, the brain and its vessels, and spaces in the brain containing cerebrospinal fluid can aid immeasurably in the localization of lesions. In concert with physical examination and history, imaging studies can provide important clues to diagnosis, and often permit a definitive diagnosis. In emergency cases, images of unconscious patients may be the only diagnostic information available.
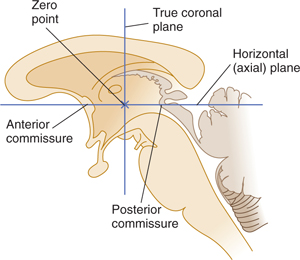
Computed tomography (CT), magnetic resonance imaging (MRI), and other similar imaging methods are usually displayed to show sections of the head, the sagittal, coronal (frontal), and horizontal (axial) planes are commonly used (Fig 22–1).
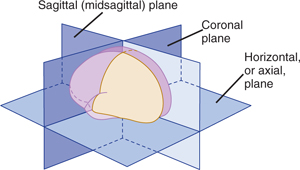
FIGURE 22–1 Planes used in modern imaging procedures.
SKULL X-RAY FILMS
Skull x-rays provide a simple method for imaging calcium and its distribution in and around the brain when more precise methods are unavailable. Plain films of the skull can be used to define the extent of a skull fracture and a possible depression or determine the presence of calcified brain lesions, foreign bodies, or tumors involving the skull. They can provide images of the bony structures and foramens at the base of the skull and of the sinuses. Skull x-ray films can also provide evidence for chronically increased intracranial pressure, accompanied by thinning of the dorsum sellae, and abnormalities in the size and shape of sella turcica, which suggest large pituitary tumors. Skull films are sometimes used to screen for metal objects before beginning MRI of the head.
ANGIOGRAPHY
Cerebral Angiography
Angiography (arteriography) of the head and neck is a neurodiagnostic procedure used when a vessel abnormality such as occlusion, malformation, or aneurysm is suspected (Figs 22–2 to 22–12; see also Chapter 12). Angiography can also be used to determine whether the position of the vessels in relation to intracranial structures is normal or pathologically changed. Aneurysms, arteriovenous fistulas, or vascular malformations can be treated by interventional angiography using balloons, a quickly coagulating solution that acts as a glue, or small, inert pellets that act like emboli.
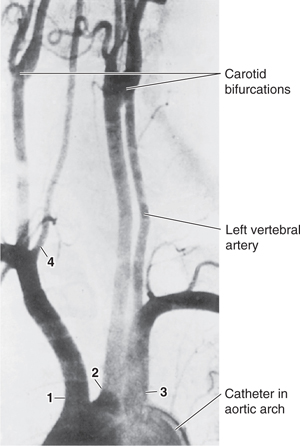
FIGURE 22–2 Angiogram of the aortic arch and stem vessels. Normal image. 1: Brachiocephalic artery; 2: common carotid artery; 3: left subclavian artery; 4: right vertebral artery. (Reproduced, with permission, from Peele TL: The Neuroanatomical Basis for Clinical Neurology. Blakiston, 1954.)
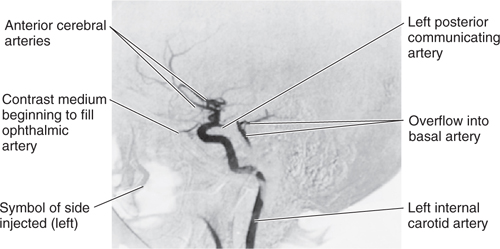
FIGURE 22–3 Left internal carotid angiogram, early arterial phase, lateral view. Normal image (compare with Fig 22–4).
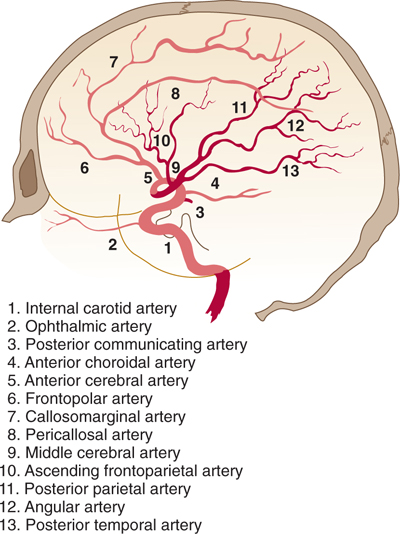
FIGURE 22–4 Schematic drawing of a normal angiogram of the internal carotid artery, arterial phase, lateral projection. The numbers refer to vessels shown in Figures 22–4 and 22–6. (Redrawn and reproduced, with permission, from List C, Burge M, Hodges L: Intracranial angiography. Radiology 1945;45:1.)
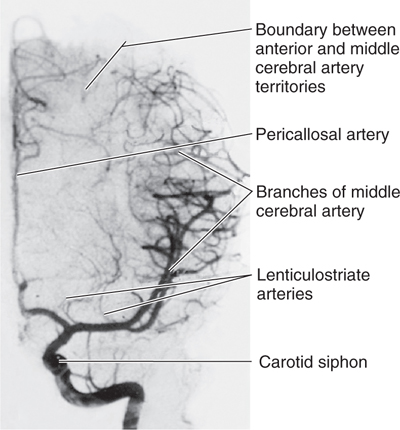
FIGURE 22–5 Left internal carotid angiogram, arterial phase, lateral view. Normal image (compare with Fig 22–6).
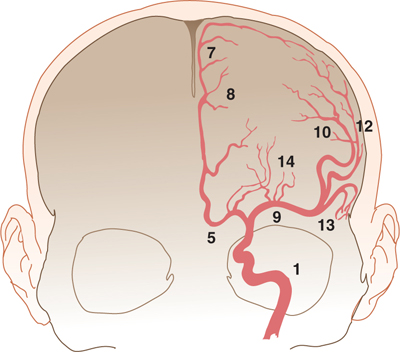
FIGURE 22–6 Schematic drawing of a normal angiogram of the internal carotid artery, arterial phase, frontal projection. (For significance of numbers, see Fig 22–4.) (Redrawn and reproduced, with permission, from List C, Burge M, Hodges L: Intracranial angiography. Radiology 1945;45:1.)
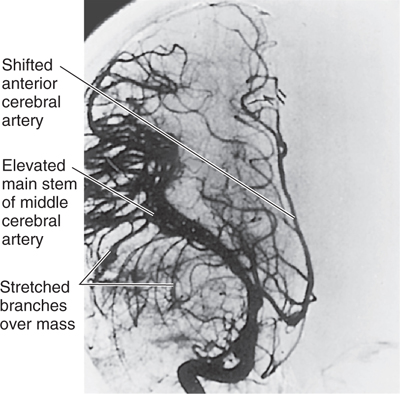
FIGURE 22–7 Right internal carotid angiogram, arterial phase, anteroposterior view. Abnormal image.
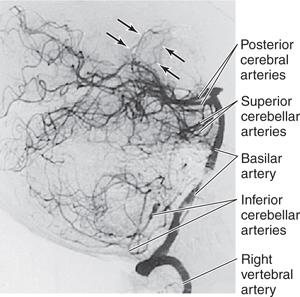
FIGURE 22–8 Vertebral angiogram, arterial phase, right lateral view. Normal image. Arrows indicate posterior choroidal arteries.
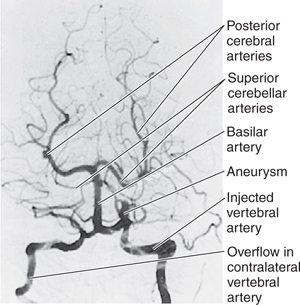
FIGURE 22–9 Vertebral angiogram, arterial phase, anteroposterior view, with head flexed (Towne position). An aneurysm is present, but the pattern of the vessels is normal.
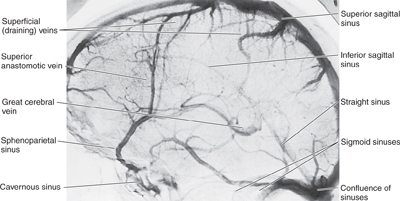
FIGURE 22–10 Left internal carotid angiogram, venous phase, lateral view. Normal image. (Compare with Figs 12–9 and 22–11.)
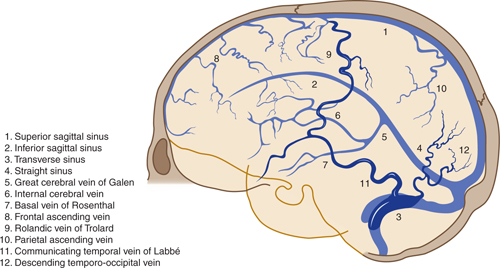
FIGURE 22–11 Schematic drawing of normal venogram in lateral projection, obtained by carotid injection. Superficial veins are shaded more darkly than the sinuses and deep veins. (Redrawn and reproduced, with permission, from List C, Burge M, Hodges L: Intracranial angiography. Radiology 1945;45:1.)
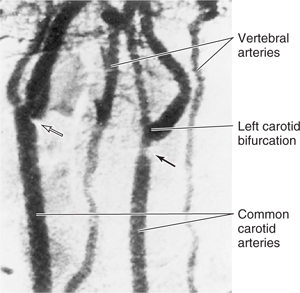
FIGURE 22–12 Digital subtraction angiogram of the neck vessels, oblique anterior view. Open arrow shows small sclerotic plaque; closed arrow shows large plaque.
Angiograms consist of a series of x-ray films showing contrast material introduced into a major artery (eg, via a catheter in the femoral) under fluoroscopic guidance. Arterial-phase films are followed by capillary and venous-phase films (see Figs 22–6 to 22–10). Right and left internal carotid and vertebral angiograms may be complemented by other films (eg, by an external carotid series in cases of meningioma or arteriovenous malformation). The films are often presented as subtracted, that is, as reversal prints superimposed on a plain film of the skull.
COMPUTED TOMOGRAPHY
CT, also called computed axial tomography (CAT), affords the possibility of inspecting cross sections of the skull, brain, ventricles, cisterns, large vessels, falx, and tentorium. Since its development in the 1960s, the CT scan has become a primary tool for demonstrating the presence of abnormal calcifications, brain edema, hydrocephalus, many types of tumors and cysts, hemorrhages, large aneurysms, vascular malformations, and other disorders.
CT scanning is noninvasive and fast. Although it has a high degree of sensitivity, its specificity is relatively limited. Correlation with the clinical history and physical examination is an absolute requirement. In the case of a subarachnoid hemorrhage, for example, although a CT scan may quickly localize the areas containing blood (Fig 12–21), additional CT images (Fig 12–22), magnetic resonance imaging, or angiography is often required to determine whether the cause was an aneurysm or an arteriovenous malformation.
The CT scanning apparatus rotates a narrow x-ray beam around the head. The quantity of x-ray absorbed in small volumes (voxels [volume elements, or units]) of brain, measuring approximately 0.5 mm2 × 1.5 mm or more in length, is computed. The amount of x-ray absorbed in any slice of the head can be thus determined and depicted in various ways as pixels (picture elements) in a matrix. In most cases, absorption is proportional to the density of the tissue. A converter translates the numeric value of each pixel to a gray scale. Black-and-white pictures of head slices are then displayed, with black representing low-density structures and white representing high-density structures. The thickness of the slices can vary, from 1.5 mm to 1 cm. The gray scale can also vary; although a setting at which brain tissue is distinguished best is commonly used, in some cases bone, fat, or air need to be defined in great detail.
A series of 10 to 20 scans, each reconstructing a slice of brain, is usually required for a complete study. The plane of these sections is the orbitomeatal plane, which is parallel to both Reid’s base plane and the intercommissural line used in stereotactic neurosurgery (Fig 22–13). Usually, a “scout view” similar to a lateral skull roentgenogram is taken with a CT scanner to align the planes of sections (Fig 22–14). With the modern technology now available, each scan takes only a few seconds. Examples of normal and abnormal CT scans are shown in Figures 22–15 and 22–16.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


