♦ Preoperative
Special Equipment
- Basic tray
- Intrathecal catheter (Medtronic, two piece, Model 8731)
- Catheter passer (Medtronic, Model 8583)
- Infusion pump for most patients (Medtronic, SynchroMed 2, 20 mL, Model 8637–20)
- Infusion pump for select patients (Medtronic, SynchroMed 2, 40 mL, Model 8637–40)
Operating Room Set-up
- Headlight
- Loupes
- Bovie, bipolar
- C-arm fluoroscopy
Anesthetic Issues
- Monitored anesthesia care in most cases
- General anesthesia for uncooperative or extremely pain-sensitive patients
- Perioperative antibiotics (first generation cephalosporin)
- Pad patient appropriately
Miscellaneous
- Chronic pain patients customarily undergo evaluation by a pain psychologist prior to implantation to rule out psychologic comorbidities that may compromise outcome; this is generally unnecessary for cancer pain or spasticity patients.
- Patients undergo an intrathecal trial of the desired medication prior to implantation; this may consist of a single bolus dose or a catheter-based infusion lasting several days. The purpose is to test the patient’s response to the medication prior to implantation.
- Intrathecal bolus dose for morphine: 1 mg
- Intrathecal bolus dose for baclofen: 50 mcg
- Intrathecal bolus dose for morphine: 1 mg
♦ Intraoperative (Fig. 146.1)
Positioning
- Lateral decubitus position, beanbag support, patient chooses side of pump placement
- Hip and knee flexion to open interlaminar spaces
- Intraoperative fluoroscopy is positioned to permit anteroposterior spinal views; the image intensifier is positioned ventrally so that the surgeon has more room to work when situated at the dorsal incision
Planning of Sterile Scrub and Preparation
- Chlorhexidine scrub of back, flank, and abdomen, followed by alcohol paint, followed by Betadine paint that is allowed to dry
- The goal is to position the infusion pump equidistant from the costal margin superiorly and iliac crest inferiorly, and equidistant from the umbilicus medially and the midaxillary line laterally.
- A 10-cm subcostal incision is marked parallel to and several centimeters below the costal margin to accommodate the desired pump positioning.
- A 4-cm midline dorsal incision is marked over the L4-L5 spinous processes.
Technique
- The incisions are injected with local anesthetic (four parts lidocaine 0.5% with epinephrine, four parts bupivacaine 0.25%, one part sodium bicarbonate)
- Withdraw pump contents using the 22-gauge noncoring needle, and fill with desired drug
- The abdominal incision is opened first, and a subcutaneous pocket large enough to accommodate the infusion pump is created. There should be 1 to 2 cm of subcutaneous fat superficial to the pump; more makes refilling difficult. The wound is packed with gauze to allow hemostasis.
- The dorsal incision is then opened, and dissection is carried down to (but not through) the thoracolumbar fascia. The soft tissue is dissected off the fascia over about a 3- by 3-cm area; this space allows for later coiling and anchoring of the catheter.
- A catheter passer is tunneled from the dorsal to the abdominal incision and is used to place the extension catheter.
- Under fluoroscopic guidance, and using a paraspinous approach, the large gauge Tuohy needle is advanced through the fascia into the next higher interspace (L3-L4). A direct midline approach is avoided since the spinous processes may compress and break the catheter in spinal extension.
- Once the intrathecal space is encountered, cerebrospinal fluid (CSF) will generally flow briskly through the needle with the stylet removed; avoid loss of an excessive amount of CSF.
< div class='tao-gold-member'>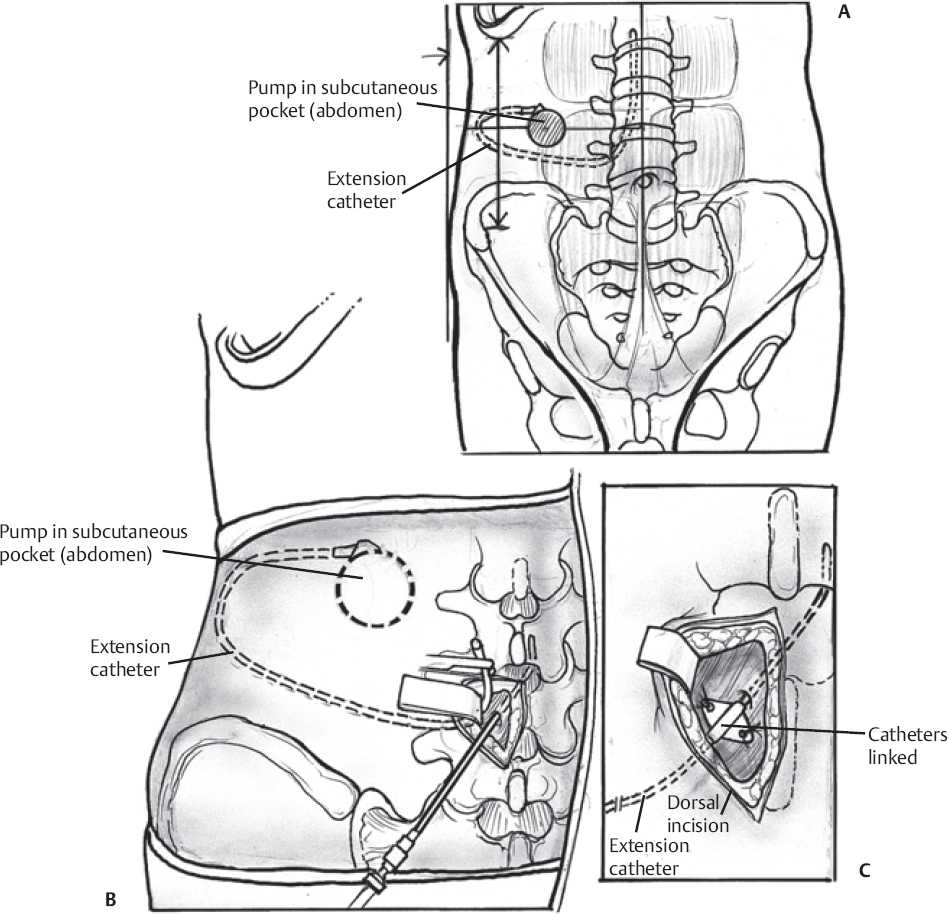 Only gold members can continue reading. Log In or Register to continue
Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel






Full access? Get Clinical Tree


