Incidence and Prevalence
Poonam Nina Banerjee
W. Allen Hauser
Introduction
To develop optimal approaches to the treatment of epilepsy, to evaluate the effectiveness of treatment strategies, and more importantly, to identify interventions that may prevent the development of epilepsy, valid information regarding the frequency, cause, and natural history of the condition is necessary. Such information is provided by descriptive and hypothesis-testing epidemiologic studies. Early reports of the prevalence of epilepsy, which used information from selective service records, provided data similar to those of contemporary studies undertaken in industrialized countries, such as the United States, for the same age groups.27 Approaches to the study of the epidemiology of epilepsy have become increasingly sophisticated; current epidemiologic studies provide a much more comprehensive picture of the characteristics of persons with epilepsy, which has led to considerable improvement in understanding epidemiologic features of the seizure disorders in general and epilepsy in particular. These improved methods include the development of clear definitions of the condition being studied; use of data provided by incidence studies of the convulsive disorders; and use of these incidence cases and other inception cohorts to determine natural history and identify risk factors. Unfortunately, incidence studies are expensive and difficult to do. Therefore, there are relatively few reports dealing with total populations. Relying on less expensive and relatively less complex studies of prevalence to gain epidemiologic insights can be compared to an epileptologist performing epilepsy surgery based on clinical history alone. One may have some of the pieces, and a correct decision may be made, but in many cases, an inappropriate procedure will be undertaken.
The following discussion reviews data regarding the incidence of seizure disorders and epilepsy, and the risk factors for epilepsy as suggested by these studies. In addition, potential insights provided by prevalence studies are highlighted. Definitions are important in epidemiologic studies. In the present discussion, the term epilepsy represents a condition characterized by two or more unprovoked seizures. For other definitions, the reader is referred to the report of the Commission on Epidemiology and Prognosis of the International League Against Epilepsy (ILAE).46
Incidence of Epilepsy
Total Population Studies
There are relatively few studies of incidence of epilepsy in total populations. In developed countries, the age-adjusted incidence of epilepsy (recurrent unprovoked seizures) ranges from 24 to 53 per 100,000 person-years.6,30,44,50,57,58,59,60,72,95,100 Total population studies reporting the incidence of a first diagnosis of unprovoked seizures (differing from incidence of epilepsy by the inclusion of persons with a single unprovoked seizure as well as those with recurrent unprovoked seizures) provides estimates of incidence ranging from 26 to 70 per 100,000 person-years37,51,57,60,72,90,112 (see Table 1). Given methodologic differences, the incidence in studies of predominantly Western, industrialized countries seems remarkably consistent across geographic areas. This seems particularly true of reports for the last two decades (1986 to 2005).
Several recent studies provide incidence from developing countries. An incidence of epilepsy that is considerably higher than that reported in industrialized countries (114 per 100,000 person-years) has been reported from a rural area of Chile.66 A study in Tanzania106 reported the incidence of epilepsy to be 77 per 100,000. These are two to three times the incidence reported in industrialized countries in which similar definitions have been used. A study in Ethiopia reported an incidence of 64, but this fell to 46 after age adjustment, underscoring the importance of age adjustment if comparisons are to be made. A large population-based survey in Ecuador97 identified all individuals with a history of seizures. Included were all persons with newly occurring nonfebrile seizures (including acute symptomatic seizures) and some children with multiple febrile seizures. Based on the number of people seen with seizures in the year preceding the survey, incidence was higher than that of most other reports (190 per 100,000), although incidence for neurologically confirmed cases was about 30% lower. In studies in France72 and Rochester, Minnesota,50 about half of newly occurring afebrile seizures do not fulfill criteria for epilepsy. Because of the broader case-inclusion criteria in the study from Ecuador and uncertainty regarding age-specific distribution and cause of acute symptomatic seizures, there is no way to compare these incidence studies. Nonetheless, the incidence of epilepsy may likely be higher in developing countries than in industrialized countries.
Table 1 Incidence of Epilepsy in Select Population-based Studies of All Age Groups | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
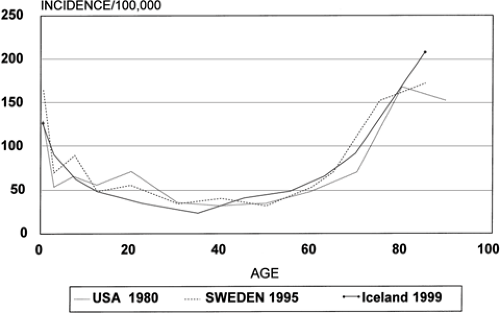 FIGURE 1. Age-specific incidence of epilepsy in industrialized countries. |
Studies in Selected Age Groups
A number of studies report the incidence of epilepsy in specific age groups. These include studies of child-ren,14,15,20,22,24,33,36,38,84,102,111,112,117 adults,37,50,64,90,95 and the elderly.71,76,105,115 Evaluation of these studies again requires consideration of definitions used, but in general, information is complementary to and consistent with incidence in total-population studies when age-specific rates are evaluated. For example, the more comprehensive studies limited to children111,117 include children with neonatal seizures and children with a single unprovoked seizure as incidence cases of epilepsy. Taking this into account, incidence in the youngest
age group in studies limited to children are, in general, similar to those reported in total population studies.
age group in studies limited to children are, in general, similar to those reported in total population studies.
Age-specific Incidence
Contrary to popular belief, epilepsy is a disease with onset at the extremes of life (Fig. 1), at least in industrialized countries. Where provided, age-specific incidence is consistently high in the youngest age groups, with highest incidence occurring during the first few months of life. Incidence falls dramatically after the first year of life, seems relatively stable through the first decade of life, and falls again during adolescence.22,51,90
In virtually all studies conducted in industrialized countries, age-specific incidence is lowest during the adult years. Contemporary incidence studies, most of which are in Western countries, show an increasing incidence—at times dramatic—in the elderly.37,50,71,88 In Western countries, the incidence of epilepsy is higher after the age of 70 years than during the first 10 years of life. Only about 50% of cases of epilepsy start in childhood or adolescence.50,90 A British general practice survey reported that almost 25% of all newly identified seizures (not epilepsy) occurred in persons aged 60 years and older.108
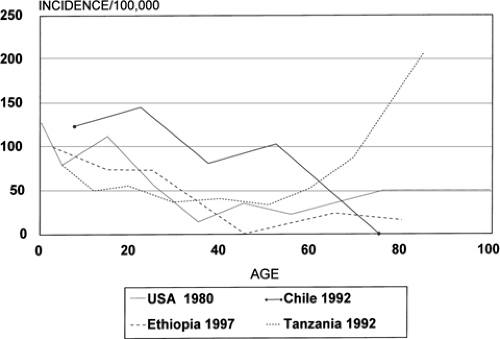 FIGURE 2. Age-specific incidence of epilepsy in developing countries. |
Table 2 Classification of Seizure Type in Select Incidence Studies | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
The reported patterns of age-specific incidence are quite different in developing countries. In studies from Africa and South America, the peak incidence of epilepsy occurs in young adults, and the dramatic increase in incidence in the elderly has not been identified (Fig. 2).66,106,116 It is likely that patterns of incidence, and therefore risks for epilepsy, are different in these populations.
Sex
In most total population studies, incidence of epilepsy or of unprovoked seizures is higher in males than in females. This seems true even after the higher incidence in males of definitive risk factors for epilepsy (i.e., head injury, stroke, central nervous system infection) is taken into account. One exception is the study from Ecuador,97 in which the male-to-female ratio is 0.8, although this study cannot be used for comparison as it included persons with acute symptomatic as well as unprovoked seizures. The other exception is the study of incidence in children in Sweden (male-to-female ratio of 0.7).112 For most but not all incidence studies, sex-specific differences in incidence are not statistically significant. The consistency of the male-to-female difference across studies suggests that males are at higher risk than females for unprovoked seizures and epilepsy.
Seizure Type
Seizure-specific incidence or proportions of cases with a specific seizure type based on the International Classification of Epileptic Seizures100 are provided in several contemporary incidence studies (Table 2). A detailed distribution from the Iceland study90 is provided in Figure 3. In studies in Rochester, Minnesota,50 the Faeroe Islands,59 and Chile,66 slightly more than 50% of incidence cases were classified as partial seizures. Partial seizures are also the predominant seizure type in Sweden in adults after information from the separate studies of adults and children is combined.37,112
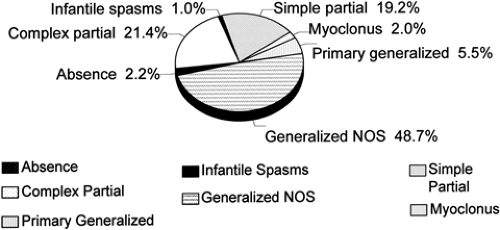 FIGURE 3. Distribution of seizure type in Iceland incidence cases, 1995–1999. NOS, not otherwise specified. |
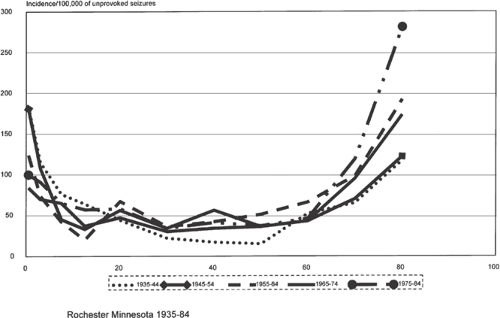 FIGURE 4. Time trends in Rochester, Minnesota, 1935–1984. |
Race
Most total population incidence studies have been performed in white populations of European extraction. Even in
studies of incidence in Asian or African populations, study groups have been homogeneous. Racial differences have been examined only in incidence or cohort studies in children. In the National Collaborative Perinatal Project,83 incidence of afebrile seizures did not differ across racial groups through the age of 7 years. In studies of Japanese children in Tokyo117 and Caucasian children in Rochester, Minnesota,50 age-specific incidence and incidence by seizure type through the age of 14 years were virtually identical. Definitions of epilepsy were similar in these two studies, although methodology was different. A study of children in New Haven, Connecticut,111 reported incidence of epilepsy through age 15 years to be 1.7 times greater in blacks than in whites, although the definition of epilepsy was quite different from those used in many of the studies mentioned above. This study also made an ecologic comparison based on mean neighborhood socioeconomic level. After controlling for race, incidence of epilepsy was significantly higher in lower socioeconomic classes.
studies of incidence in Asian or African populations, study groups have been homogeneous. Racial differences have been examined only in incidence or cohort studies in children. In the National Collaborative Perinatal Project,83 incidence of afebrile seizures did not differ across racial groups through the age of 7 years. In studies of Japanese children in Tokyo117 and Caucasian children in Rochester, Minnesota,50 age-specific incidence and incidence by seizure type through the age of 14 years were virtually identical. Definitions of epilepsy were similar in these two studies, although methodology was different. A study of children in New Haven, Connecticut,111 reported incidence of epilepsy through age 15 years to be 1.7 times greater in blacks than in whites, although the definition of epilepsy was quite different from those used in many of the studies mentioned above. This study also made an ecologic comparison based on mean neighborhood socioeconomic level. After controlling for race, incidence of epilepsy was significantly higher in lower socioeconomic classes.
Time Trends
Information on time trends of incidence is provided in the studies from Copparo, Italy,44 and Rochester, Minnesota.50 In the Italian study, the incidence of epilepsy decreased over three time intervals from 1964 to 1978, although this may be related to methodologic issues (Fig. 4). The Minnesota study reports a more than 50% decrease in the incidence of epilepsy in those under the age of 10 years from 1935 to 1984. During these same years, there was an increase in incidence in those over age 60 years, causing the age-adjusted incidence in this community over the entire 50-year interval to show little change.
The fall in the middle decades of this century is largely unexplained, but the increase after 1975 may be related to increased survivorship of very-low-birth-weight infants. The findings of this study underscore the potential pitfalls in relying on total incidence of epilepsy in children.
The fall in the middle decades of this century is largely unexplained, but the increase after 1975 may be related to increased survivorship of very-low-birth-weight infants. The findings of this study underscore the potential pitfalls in relying on total incidence of epilepsy in children.
In the studies of a British general practice that included all afebrile seizures, incidence under age 20 was 172 per 100,000 between 1964 and 1973, 152 per 100,000 between 1974 and 1983, and significantly lower (61 per 100,000) from 1984 to 1993.26 This difference may be explained partially by inclusion in the earlier period of nonepileptic episodes, but even cautious interpretation of these data suggest dramatic reductions in the incidence of childhood-onset epilepsy in industrialized countries. The reduction in incidence over time in children is not readily explained by current epidemiologic or clinical data and deserves further investigation.
It appears that the incidence of epilepsy in the elderly is increasing—at least in the United States. This may be related, at least in part, to an increase in the proportion of the population with a history of stroke.4 Although the incidence of stroke is decreasing, the prevalence is increasing as more people are surviving strokes.
Epileptic Syndromes
There are few total population incidence studies that present the distribution of epilepsy syndromes such as the study conducted in Bordeaux,72 studies from Rochester,50 and studies from Iceland.90 Some studies provide the distribution of epilepsy syndromes among newly diagnosed cases of epilepsy.63,72,78,112,121
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


