Infratentorial Midline Cyst
Gregory L. Katzman, MD, MBA
DIFFERENTIAL DIAGNOSIS
Common
Mega Cisterna Magna
Arachnoid Cyst
Less Common
Neurocysticercosis
Dandy-Walker Continuum
Obstructive Hydrocephalus (“Trapped” or “Encysted” 4th Ventricle)
Pilocytic Astrocytoma
Hemangioblastoma
Epidermoid Cyst
Dermoid Cyst
Enlarged Perivascular Spaces
Rare but Important
Congenital Vermian Hypoplasia
Ganglioglioma
Pleomorphic Xanthoastrocytoma
Neurenteric Cyst
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Is mass intra- or extra-axial?
If extra-axial, cistern or 4th ventricle?
CSF cistern (mega cisterna magna, Dandy-Walker continuum, arachnoid cyst, epidermoid cyst)
4th ventricle (encysted ventricle, neurocysticercosis, dermoid or epidermoid cyst, cystic neoplasm)
If intra-axial, pons, vermis, or cerebellum?
Cerebellum (enlarged perivascular spaces, cystic neoplasm)
Vermis (cystic neoplasm, vermian hypoplasia)
Pons (cystic neoplasm > > enlarged perivascular spaces)
Helpful Clues for Common Diagnoses
Mega Cisterna Magna
Enlarged posterior fossa CSF space
Normal vermis completely covers 4th ventricle (rules out Dandy-Walker malformation/variant)
May show striking scalloping of skull (due to CSF pulsations)
Arachnoid Cyst
Sharply demarcated extra-axial cyst
Follows CSF attenuation/signal
Suppresses on FLAIR, no DWI restriction
Size varies from few millimeters to giant
Often asymptomatic, found incidentally
Helpful Clues for Less Common Diagnoses
Neurocysticercosis
Best clue: Cyst with “dot” inside
± Discrete eccentric scolex
Cyst slightly hyperintense to CSF
Cisterns > 4th ventricle
Dandy-Walker Continuum
DWC: Broad spectrum of cystic posterior fossa malformations
DW malformation: Large posterior fossa + large CSF cyst, normal 4th ventricle absent, lambdoid-torcular inversion
DW variant: Failure of “closure” of 4th ventricle, vermian hypoplasia
Includes persistent Blake pouch cyst, mega cisterna magna
2/3 have associated CNS &/or extracranial anomalies
Obstructive Hydrocephalus (“Trapped” or “Encysted” 4th Ventricle)
Due to obstructing lesions of 4th ventricle; all foramina must be involved (Magendie, Luschka, aqueduct)
May be from hemorrhage, infectious, inflammatory, or neoplastic causes
Ventricle enlarged but maintains basic shape
CSF intensity/attenuation
Pilocytic Astrocytoma
Cystic cerebellar mass with enhancing mural nodule
Cerebellum > vermis, 4th ventricle
Child > adult
Hemangioblastoma
Best diagnostic clue: Adult with intra-axial posterior fossa mass with cyst, enhancing mural nodule abutting pia
Size varies from tiny to several centimeters
1-2% of primary intracranial tumors, 7-10% of posterior fossa tumors
May be associated with von Hippel-Lindau syndrome
Epidermoid Cyst
Congenital inclusion cyst
Lobulated, irregular, insinuating CSF-like mass with “fronds”
Cerebellopontine angle cistern > 4th ventricle
FLAIR usually doesn’t completely null; restricts on DWI
Dermoid Cyst
Congenital inclusion cyst
Looks like fat
Use fat-suppression sequence to confirm
± Rupture (fat droplets in cisterns, sulci, ventricles)
May cause chemical meningitis, extensive enhancement
Enlarged Perivascular Spaces
Pial-lined interstitial fluid-filled structures that accompany penetrating arteries but do not communicate directly with subarachnoid space
Cluster of variably sized intra-axial cysts
Off-midline (dentate nuclei) > midline (vermis, pons)
Follow CSF
Suppress completely on FLAIR
No restriction on DWI
No enhancement
“Leave me alone” lesion that should not be mistaken for serious disease
Helpful Clues for Rare Diagnoses
Congenital Vermian Hypoplasia
Prototype = Joubert syndrome
Inherited hypoplasia or aplasia of vermis characterized by transient episodic hyperpnea, oculomotor abnormalities, ataxia, variable mental retardation
“Molar tooth” brainstem; “bat wing” or “umbrella” shaped 4th ventricle; vermian remnant variable size
Midline anomalies common (holoprosencephaly, frontonasal dysplasia, facial clefting)
Ganglioglioma
Best diagnostic clue: Partially cystic, enhancing, cortically based mass in child/young adult
Cortical dysplasia commonly associated
Excellent prognosis if surgical resection complete
Malignant degeneration rare, approximately 5-10% (glial component)
Pleomorphic Xanthoastrocytoma
Supratentorial cortical mass with adjacent enhancing dural tail
Cyst and enhancing mural nodule typical
98% supratentorial, rarely found in cerebellum
Despite circumscribed appearance, tumor often infiltrates
Neurenteric Cyst
Benign malformative endodermal CNS cyst
Round/lobulated nonenhancing mass
Anterior to pontomedullary junction, slightly off-midline
Slightly/moderately hyperintense compared to CSF
Image Gallery
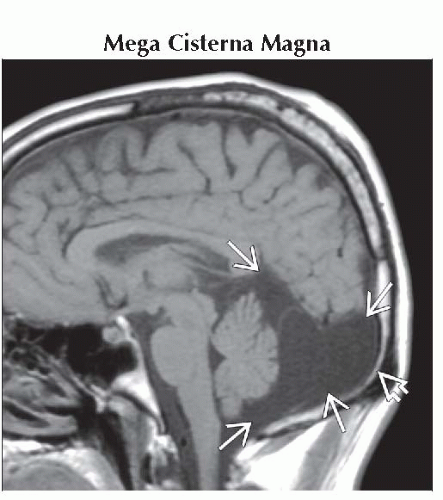 Sagittal T1WI MR in the midline shows a very large CSF-intensity space behind an intact vermis
 . Note the thinned inner table of the occipital bone . Note the thinned inner table of the occipital bone  . .Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
