Chapter 4 Intradural Extramedullary Benign Tumors
MENINGIOMA
HISTOLOGY/GRADING
GENERAL
• Meningiomas are dural-based neoplastic proliferations of meningothelial cells (arachnoid cap cells).
• The classic histologic findings include lamellar (psammomatous) calcifications and nuclear pseudoinclusions, which can be found in all subtypes of this tumor.
• The neoplastic cells demonstrate uniform vimentin immunoreactivity and patchy to widespread epithelial membrane antigen (EMA) immunoreactivity.
• Adhering to the World Health Organization 2000 classification of central nervous system tumors,1 grading is based on histologic subtype and other features (e.g., necrosis, mitotic rate).
Grade I
MENINGOTHELIAL
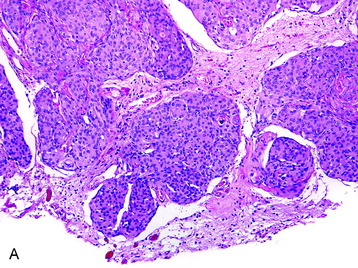
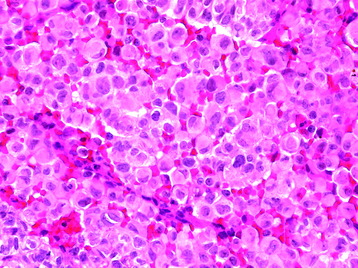
• The meningothelial meningioma is composed of syncytial lobules of uniform cells with oval nuclei (Fig. 4-1, A).
• The histologic differential (in small specimens) includes benign meningothelial proliferations associated with a neighboring process (e.g., a reactive response).
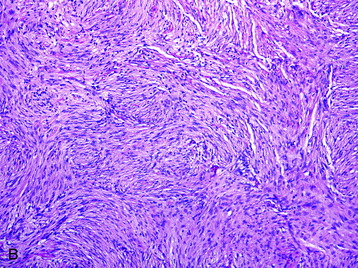
FIBROUS
• This subtype is composed of spindle-shaped meningothelial cells in a fascicular arrangement with a variable amount of interposed collagen (Fig. 4-1, B).
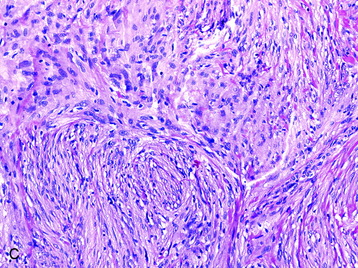
TRANSITIONAL
• The transitional meningioma has features of both meningothelial and fibrous subtypes with the cells commonly arranged in whorling architectural patterns (Fig. 4-1, C).
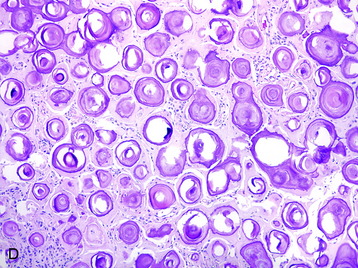
PSAMMOMATOUS
• This subtype is composed mainly of psammomatous calcifications with a paucity of cellular elements (Fig. 4-1, D).
• Even though schwannomas associated with the Carney complex, a multiple neoplasia syndrome, have a substantial psammomatous component and could be confused with this meningioma subtype, the former tumor is typically pigmented and demonstrates diffuse S100 protein and HMB-45 immunoreactivity.
Grade II
CLEAR CELL
• This subtype is composed of cells with clear glycogen-rich, periodic acid-Schiff–positive cytoplasm.
CHORDOID
• A chordoid phenotype is most often seen as a secondary pattern within meningiomas with other histologic subtypes.
Atypical
• Irrespective of the histologic subtypes previously described, a meningioma is assigned a grade II if three of the following five criteria are fulfilled:
• A grade of II is assigned if four or more mitotic figures per 10 high-power fields are identified.
• Clinicopathological studies3 have indicated that the presence of brain invasion confers a more aggressive clinical course, and this finding alone justifies a diagnosis of grade II meningioma (Fig. 4-2, D).
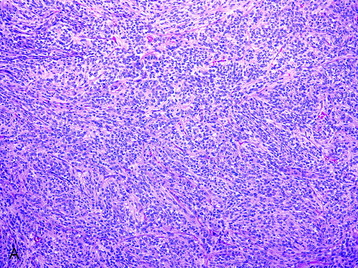
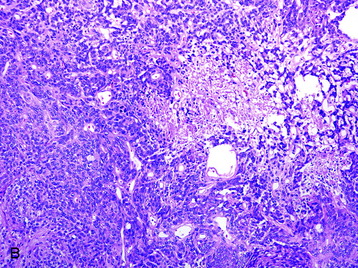
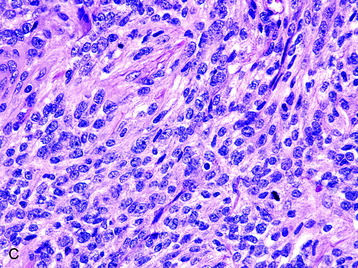
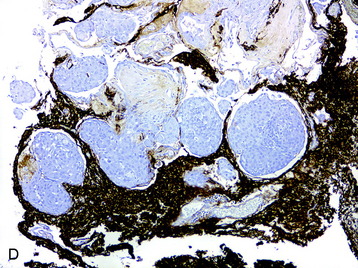
Fig. 4-2 Atypical features in meningiomas. A, Patternless or sheet-like growth pattern. B, Focus of spontaneous necrosis. C, A hypercellular area containing cells with prominent nucleoli and mitotic figures. D, Glial fibrillary acidic protein immunohistochemical stain of tumor in Fig. 4-1, A highlighting brain parenchyma between the infiltrating tumor nests (×100). (A-C, hematoxylin–eosin stain; A and B, ×100; C, ×400.)
Grade III
PAPILLARY
• This subtype, commonly found in the pediatric population, is composed of cells in a pseudopapillary arrangement with a fibrovascular core.
RHABDOID
• The rhabdoid subtype is composed of cells with abundant eosinophilic cytoplasm and eccentrically positioned nuclei (Fig. 4-3). This meningioma subtype typically has an association with high mitotic rate and other cytoarchitectural anaplastic features, as well as evidence of brain invasion.4,5
RADIOLOGY
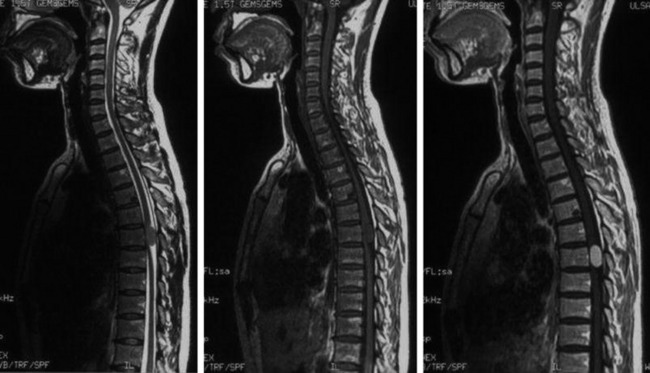
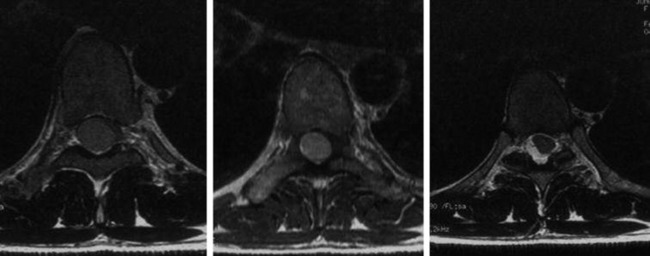
• The location of meningioma is typically intradural, extramedullary. However, it is rarely located in intraosseous, extradural, or even paraspinous areas. On T1-weighted images (T1WI), the signal of the mass is isointense to the spinal cord (Figs. 4-4 and 4-5).
• On T2-weighted images (T2WI), most parts of the mass show iso-signal to the spinal cord (see Figs. 4-4 and 4-5).
• If a calcified area is included, the signal may change to low. When the meningioma is very vascular, prominent flow void can be displayed.
NERVE SHEATH TUMOR—SCHWANNOMA
DISTRIBUTION
• Schwannomas may be found throughout all levels of the spinal cord and involve the sensory nerve roots.
• Schwannomas may have both intradural and extradural components; an intramedullary location is rare.
HISTOLOGY/GRADING
• Schwannomas are proliferations of neoplastic Schwann cells, which may have variable appearances (e.g., spindled, epithelioid, melanotic).
• Classic schwannoma (grade I)




• Histologic sections show Antoni A (densely cellular) and Antoni B (less cellular, sometimes cystic) areas (Fig. 4-7, A).
• Within Antoni A regions, Verocay bodies (small groups of fibrils surrounded by parallel rows of neoplastic cells) are commonly found.
• Cellular atypia alone (usually in Antoni B areas) in otherwise unremarkable schwannomas reflect degenerative (so-called “ancient”) changes and confers no prognostic significance. Other reactive and degenerative features, including cyst formation, macrophage and lymphocyte infiltration, and hemosiderin-laden cells, are commonly found in Antoni B areas (Fig. 4-7, B).
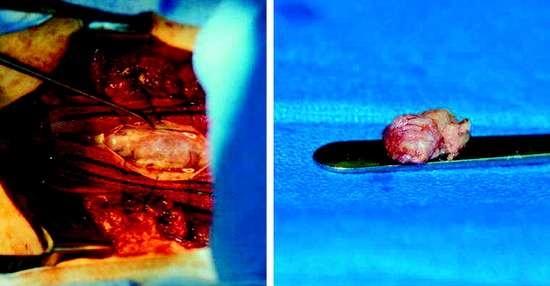
• The nerve from which the schwannoma arises may be identified in the specimen and, if so, is compressed to the edge of the tumor (Fig. 4-7, C).
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
