♦ Preoperative
Operative Planning
- Magnetic resonance imaging (MRI): define rostral/caudal extent of tumor, edema, syrinx
- Computed tomography: spinal dysraphism
- Calcium and hemorrhage within lesion on MRI: teratomas contain remnants from each embryonic layer and have mixed signal intensities
- Teratomas have an age-related propensity for malignant degeneration
♦ Intraoperative
Equipment
- Basic spine tray
- High-speed drill
- 1-, 2-, and 3-mm Kerrison rongeurs
- Operating microscope
- Somatosensory evoked potentials and motor evoked potentials; electromyog-raphy in conus medullaris lesion
- Ultrasonic aspirator
Approach
- Dictated by level of involvement: cervical, thoracic, lumbar
Tumor Resection (Fig. 135.1)
- Dexamethasone 10 mg or 20 mg intravenous at start of case.
- Inspect skin for dermal sinus tract, and excise it completely
- Patient prone
- Standard laminectomy or laminoplasty
- Dura opened midline and tented to muscle laterally
- Identify dorsal midline by visualizing exiting nerve roots bilaterally (cord often rotated by tumor)
< div class='tao-gold-member'>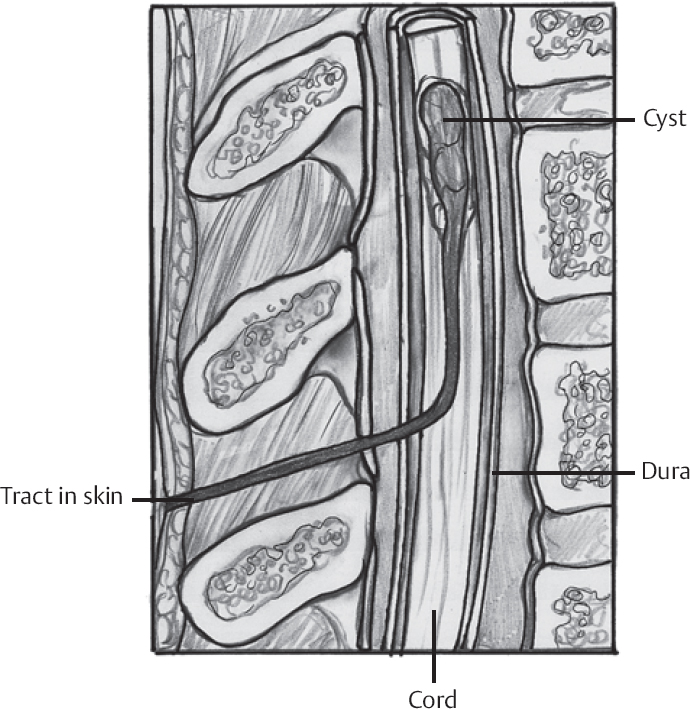 Only gold members can continue reading. Log In or Register to continue
Only gold members can continue reading. Log In or Register to continue








