Chapter 21 Lateral Approaches to Cervicothoracic Junction
RADIOLOGICAL IMAGING FOR CERVICOTHORACIC JUNCTION AREA
As a simple radiological study, three serial views (anteroposterior [AP] and both lateral views) are commonly used in the cervical spine. At the cervicothoracic junction, the shoulder joint may preclude the correct imaging of the lesion (Fig. 21-1, A). Radiography of this region that allows adequate visualization may be technically difficult to obtain, and in at least 30% of the patients the C7–T1 space is not visualized on the three-view series.1 The bilateral oblique view and swimmer’s views can be helpful in this situation. In patients for whom the standard AP and lateral view series fails to demonstrate the cervicothoracic junction, swimmer’s views and supine oblique views show the alignment of the vertebral bodies with equal frequency (Fig. 21-1, B). However, supine oblique films are safer, expose patients to less radiation, and are more often successful in demonstrating the posterior elements at the cervicothoracic junction.1


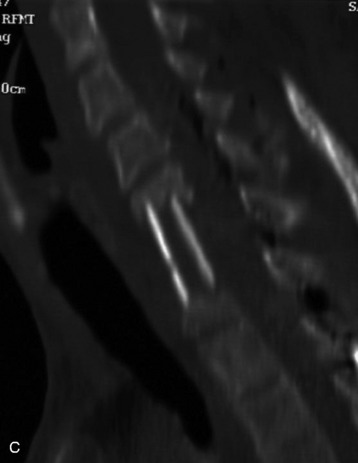
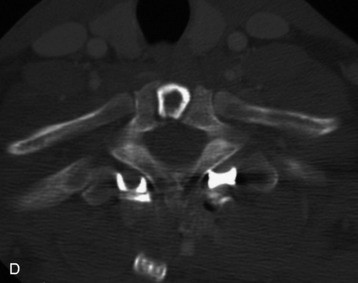
When the corpectomy is performed at the C7 and T1 levels, the graft position is not evaluated with a simple lateral view (Fig. 21-2, A). With the oblique view, the alignment can be recognized with relative ease (Fig. 21-2, B). For the adequate evaluation of the C7–T1 region, a computed tomography (CT) scan is superior to simple radiography and has several advantages. It shows correct anatomical structures around the transverse process and rib head complex. It also provides sagittal reconstruction, which enables the surgeons to decide the correct position of the graft and instrument. If the CT scan is performed, the correct position of the bone graft and instrument is easily seen with axial and sagittal scans (Fig. 21-2, C and D).


POSTEROLATERAL PARASCAPULAR APPROACH TO UPPER THORACIC SPINE (TRANSTHORACIC, TRANSPLEURAL THIRD RIB RESECTION APPROACH)
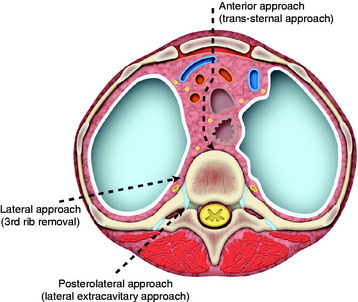
A small thoracotomy through the third rib bed provides access to the retromediastinal space of the cervicothoracic junction (Fig. 21-3). This approach can be accessed with the posterolateral or anterolateral route. The posterolateral approach has several advantages over the anterolateral one. The posterolateral approach can expose the cervical region simultaneously and allow posterior fusion surgery if necessary. It provides a shorter access than the anterior route.
Position and Incision
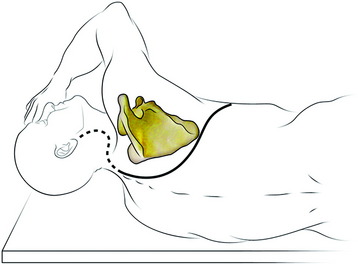
The patient is in the lateral decubitus position with the upper limb of the same side hanging in front of the thorax to encourage the maximum displacement of the scapula (Fig. 21-4). The right side approach is preferred to left side approach below the T4 level because greater vessels can be avoided. At the levels of T1–3 the greater vessels are not encountered, so the approach side is selected according to the lesion side.2 A curve commencing at the tip of the spinous process around the posterior angle of the scapula continues along its vertebral border and runs forward 2 or 3 cm above its tip to pass along the line of the fifth rib.1
Muscle Dissection
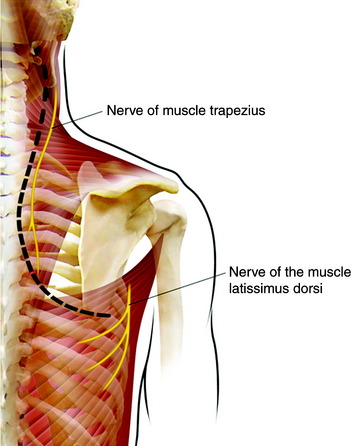
The muscles that connect the spine to the scapula are the trapezius, rhomboid, and levator scapulae. The trapezius muscle is incised along the medial border of the scapula. The division should be made not more than two fingers breadth from the spine to prevent injury of the spinal accessory nerve (Fig. 21-5). Inferior fibers of the trapezius muscle should be transected for the flap to be reflected. The rhomboids are then detached from the vertebral border of the scapula. Then the scapula is mobilized and lifted up, while the surgeon pulls upward and forward with a self-retaining hook. The levator scapulae muscle should be transected for the exposure of the lower cervical region. The entire group of erector spinae muscle and transversospinalis muscle can be dissected off the spinous process, laminae, facets, and transverse processes as a single muscular mass. The insertion of the iliocostalis thoracis muscle also is taken down.
Rib Resection
The intercostal muscles and soft tissue are stripped from the rib. In those tissues, the intercostal artery, vein, and nerve are included. Underneath the rib, a vein is located just below the bone, and artery and nerve are arranged from cephalad to caudad order. The ribs that are involved to the surgical lesion are resected 5–6 cm lateral to the junction of the rib with the transverse process (Fig. 21-6).
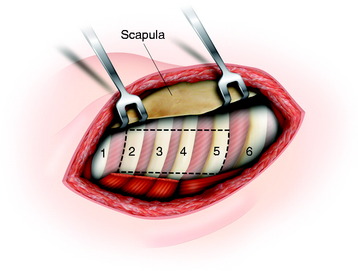
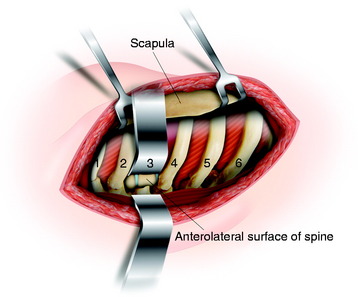
The posterior arches of the second, third, fourth, and fifth ribs are resected, which gives an excellent view of the upper thoracic vertebrae. When wide exposure is not required, the resection of the third rib only will allow for a sufficient view of the upper thoracic spine (Fig. 21-7).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


