CHAPTER 62 LOW CEREBROSPINAL FLUID HEADACHE
BACKGROUND AND TERMINOLOGY
In 1938, Schaltenbrand used the term aliquorrhea to describe the spontaneous occurrence of an entity manifested by very low cerebrospinal fluid (CSF) opening pressures and orthostatic headaches, among other features.1,2 Sometimes referred to as Schaltenbrand’s headaches, this later came to be known as spontaneous intracranial hypotension.3 It is now realized that practically all cases of spontaneous intracranial hypotension result from spontaneous CSF leaks,4 often at the level of the spine (particularly the thoracic spine5) and only rarely at the skull base. CSF leak leads to CSF volume depletion. Terms such as spontaneous CSF leak, CSF hypovolemia, and CSF volume depletion have been used interchangeably with spontaneous intracranial hypotension, because some patients with this disorder have consistently normal CSF opening pressures.5,6 True hypovolemic state (reduced total body water), CSF shunt overdrainage, dural holes or tears as the result of lumbar puncture, epidural catheterization, surgery, and trauma all may lead to loss of CSF volume. In this chapter, we focus on spontaneous CSF leaks.
ETIOLOGY OF SPONTANEOUS CEREBROSPINAL FLUID LEAKS
Some patients report a history of trivial trauma, such as coughing, pushing, trivial falls, lifting, and sports activities. Evidence for weakness of the dural sac is accumulating. Meningeal diverticula are seen more frequently in patients with spontaneous CSF leaks. Increased frequency of meningeal diverticula and also CSF leaks have been reported in Marfan’s syndrome.7–9 Some patients with spontaneous CSF leaks show stigmata of the disorders of a connective tissue matrix (e.g., marfanoid features, hyperflexible joints, hyperextensible skin).5,10
In uncommon instances, a dural tear from a spondylotic spur or disc herniation11,12 may cause dural defect and CSF leak.
CLINICAL MANIFESTATIONS
Headache is the most common manifestation. It is “classically” orthostatic (present in upright position, relieved by recumbency).3,5 It is often not throbbing, but it may be throbbing; it is often bilateral, but it may be unilateral; and it is often aggravated or sometimes even triggered by Valsalva-type maneuvers. The headache may be frontal, fronto-occipital, holocephalic, or occipital. Not all headaches in CSF leaks are orthostatic, and variability is substantial (Table 62-1).5,13–17 Furthermore, not all orthostatic headaches result from CSF leaks. For example, they can be the dominant clinical manifestation in some patients with postural tachycardia syndrome.18
TABLE 62-1 Headache Variations in Cerebrospinal Fluid (CSF) Leaks
MRI, magnetic resonance imaging.
CLINICAL MANIFESTATIONS OTHER THAN HEADACHES
Many of the patients with spontaneous CSF leaks have one or, often, more symptoms in addition to the headaches (Table 62-2).3,5,19–32
TABLE 62-2 Clinical Features Other Than Headaches
Rare manifestations: facial numbness or weakness, diplopia due to third or fourth cranial nerve palsy,20–23 galactorrhea,24 Menière’s disease–like manifestations,25 upper limb radiculopathy,26 encephalopathy,27 stupor,28 coma,29 parkinsonism,30 ataxia, incontinence, gait unsteadiness,31 frontotemporal dementia32 |
Proposed mechanisms of clinical manifestations in CSF leaks and intracranial hypotension are listed in Table 62-3.3,5,19–34
TABLE 62-3 Mechanisms of Clinical Manifestations or Cerebrospinal Fluid Volume Depletion
| Clinical Manifestation | Proposed Mechanism |
|---|---|
| Headache | Descent of the brain, stretch and distortion of pain-sensitive suspending structures of the brain3,5,33,34,34a |
| Cranial nerve palsies | Stretching or compression of related cranial nerves19–23 |
| Dizziness, change in hearing | Stretching of eighth cranial nerve or pressure changes in perilymphatic fluid of the inner ear5,25 |
| Galactorrhea and increased prolactin | Distortion of pituitary stalk24 |
| Radicular upper limb symptoms | Stretching of cervical nerve roots or irritation by dilated epidural venous plexus5,26 |
| Encephalopathy, stupor, coma | Diencephalic compression27–29 |
| Cerebellar ataxia, parkinsonism | Compression of posterior fossa and deep midline structures30 |
| Frontotemporal dementia | Compression of frontotemporal lobes32 |
| Gait disorder | Spinal cord venous congestion31 |
DIAGNOSIS
Cerebrospinal Fluid Examination
Analysis reveals the following characteristics:

 Protein concentration: normal or elevated (protein concentrations up to 100 mg/dL are common, and a concentration up to 1000 mg/dL has been reported).15
Protein concentration: normal or elevated (protein concentrations up to 100 mg/dL are common, and a concentration up to 1000 mg/dL has been reported).15
 Leukocyte count: normal or elevated (pleocytosis with counts up to 50 cells/mm3 is common, and a count up to 222 cells/mm3 has been reported).5
Leukocyte count: normal or elevated (pleocytosis with counts up to 50 cells/mm3 is common, and a count up to 222 cells/mm3 has been reported).5

Radioisotope Cisternography
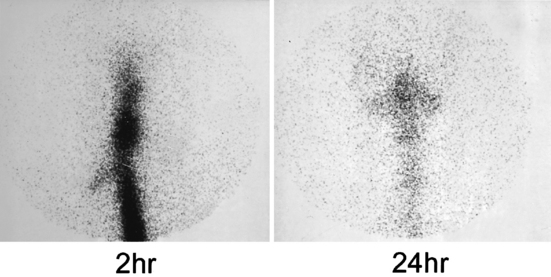
Indium 111 is the radioisotope of choice. This is introduced intrathecally, typically through a lumbar puncture, and its movement is monitored by sequential scanning at various intervals, up to 24 or even 48 hours. Normally, by 24 hours (but often earlier), substantial radioactivity can be detected over the cerebral convexities. When a spinal CSF leak exists, the activity typically does not extend much beyond the basal cisterns. Therefore, images at 24 or even 48 hours reveal either absence or paucity of activity over the cerebral convexities.35–37 This finding is the most common cisternographic abnormality in CSF leaks. Detection of parathecal activity that may point to the level or approximate site of the leak, although more desirable, is noted much less commonly (Fig. 62-1). Furthermore, meningeal diverticula, if large enough, may appear as foci of parathecal activity. Another cisternographic observation in CSF leaks is the early appearance of radioactivity in the kidneys and urinary bladder (<4 hours versus 6 to 24 hours), indicative of early entrance of extravasated isotope into the venous system and its early renal clearance and early appearance in the urinary bladder.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) has truly revolutionized the diagnosis of spontaneous CSF leaks and has been instrumental in recognizing its broad clinical spectrum. Head and spine MRI abnormalities are listed in Table 62-4.
TABLE 62-4 MRI Abnormalities in Cerebrospinal Fluid Leaks
Diffuse pachymeningeal enhancement: the most common head MRI abnormality; may be thick or thin but is typically uninterrupted, nonnodular, bilateral, both supratentorial and infratentorial, and without leptomeningeal involvement (see Fig. 62-2A)5,41,54 Descent (“sagging” or “sinking”) of the brain: manifested by descent of cerebellar tonsils, which may mimic Chiari type I malformation (see Fig. 62-3)55; by obliteration of prepontine or perichiasmatic cisterns; by crowding of the posterior fossa; and by flattening of the optic chiasm (see Figs. 62-2A and 62-3) < div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





