COMPUTED TOMOGRAPHY
Computed tomography (CT) is a general term for several radiographic techniques that result in a series of images showing slices of an organ or body region, such as the brain. The CT systems measure the attenuation of X-ray beams passing through target tissue; this is done using a small X-ray device that rotates around the body region of interest in a fixed plane. Various absorption and scattering processes are utilized in CT: coherent scattering, photoelectric absorption and Compton scattering. The X-ray tubes provide incident X-rays yielding a spectrum of X-rays with a transmission of the signals. The signals are sent to a computer that produces the corresponding cross-sectional slice for that plane. The image is composed of a set of individual pixels, which represent the attenuation of the X-ray at the corresponding point. These attenuation values are referred to as the CT number or Hounsfield units. The computer can create sections in axial, coronal and sagittal alignments using an image reconstruction process. The three major paradigms of image reconstruction are (i) simple back-projection, (ii) filtered back-projection, and (iii) iterative reconstruction.
In a single CT scan across one section in a patient, thousands of X-ray transmission measurements are obtained along many different angular projections. From these measurements, utilizing a variety of mathematical paradigms, a matrix of CT numbers can be computed for the cross-sectional plane through the patient and then displayed as a grey-scale image. There are a number of artefacts that affect the performance of CT scanning and the quality of the acquired data. These artefacts lead to streak patterns on the image display or appear in the form of CT number inaccuracies. Some of the artefacts are caused during the X-ray transmission phase (e.g. patient motion, polychromatic effects), X-ray detection and measurement (e.g. detector imbalance, scatter collimation), data acquisition (e.g. slice geometry, profile sampling) and data processing (e.g. algorithm effects). CT scans require the use of a limited amount of radiation, which presents a potential health risk for those undergoing CT scans. The estimated radiation exposure varies by the particular type of CT scan performed. It is estimated that a head CT is associated with 1.5 millisieverts, which is equivalent to the radiation exposure from 75 chest X-rays. This amount of radiation exposure is considered an acceptable risk when the CT is medically indicated. CT studies should follow the radiation recommendation, including the special cases for multiple exposures and overlapping scanning techniques.
With advances in scanning, software and display systems, the quality of CT images improved (i.e. better resolution) and has led to many useful clinical applications, including virtual CT colonoscopy or angiography. Neuroimaging with CT is used for studying various psychiatric populations including schizophrenia and depression, as well as aging and dementia.
CT imaging is used to examine brain structure; it allows for the ready identification of many structures, although it does have limitations. By measuring differences in density, it can distinguish among CSF, blood, bone, grey matter and white matter. CT is particularly useful for demonstrating injuries such as skull fractures (bone abnormalities), subdural haematoma (haemorrhage regions) and different lesions (mass effect). CT is also used to study variation in atrophy or ventricular enlargement. However, CT studies are restricted by location of the structures like the brain stem because of surrounding bone. CT has been used to measure cerebral atrophy and grey matter (secondary loss of neurons) since 19741. CT has been widely used in the identification of dementia2. Many studies were performed to study age variation in geriatric populations3-6, normal ageing7 and the effect of presence of dementia8‘9.
With improvement in resolution of CT, it was used to distinguish some pathological processes, which primarily affect white matter (i.e. demyelination)10,11. A large number of CT studies of white-matter diseases in the geriatric population were published12-16. CT measurements of the cerebrospinal fluid (CSF) spaces from patients with geriatric depression, normal control subjects and patients with primary degenerative dementia have been compared and studied also17.
CT is widely available and well understood, but is nowadays supplemented with magnetic resonance imaging (MRI) to use the advantages of both techniques.
In 2003, Paul C. Lauterbur and Peter Mansfield were awarded the Nobel Prize in Medicine for their discovery of MRI. MRI revolutionized in vivo human brain imaging, allowing for remarkably clear high-resolution images of the brain. MRI is based on the concept of nuclear magnetic resonance (NMR), where the measurement of the signals comes from the nuclei in response to radio waves that have the same frequency as the nuclei themselves18,19. For a comprehensive review, please refer to18,19.
The relaxation time (T1) is a property of a tissue at a given magnetic field strength. With each excitation pulse, the longitudinal magnetization begins to recover and reduces to steady state after several pulses. The time between repetitions of the excitation pulse is called the repetition time (TR). The repetition time and flip angle are the two major parameters varied to control the T1 weighting of an image. The transverse magnetization decays at the rate of T2 relaxation time. The delay between the creation of the transverse magnetization and the measurement of the resulting echo is called the echo time (TE). The images where signal intensity is largely dependent on T2 differences (or TE values) are called T2-weighted images. The various pulse sequences are designed based on TR, TE and other parameters to obtain the necessary contrast variation in the magnetic resonance image. The magnetic resonance image can have different artefacts, such as motion-induced artefacts, susceptibility, wrap around, edge artefacts (partial volume, chemical shift edge, truncation, relaxation), ghost artefacts, altered signal intensity, stripes and image distortion. The different pulse sequences used in imaging sequences, such as T2*, echo planar imaging used in BOLD fMRI, fluid-attenuated inversion-recovery imaging (FLAIR), diffusion weighted imaging, magnetization transfer imaging and others, are novel variations obtained from optimization of the various parameters.
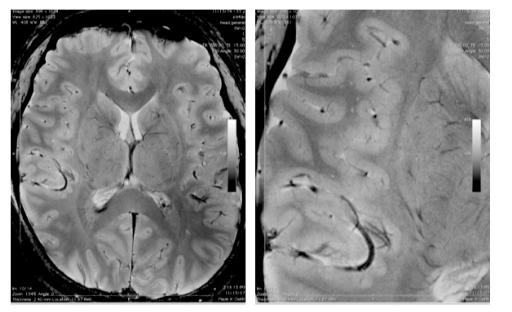
Difference between 1.5 T, 3 T vs. 7 T Images
Typically the MRI scanner is built around a permanent magnet, which is the most expensive and important component of the scanner1819
Related posts:
 The Care Home Experience Alisoun Milne
The Care Home Experience Alisoun Milne
 The Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE) Nicolas Cherbuin andAnthony Francis Jorm
The Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE) Nicolas Cherbuin andAnthony Francis Jorm
 The Lundby Study Mats Bogren, Cecilia Mattisson and Per Nettelbladt
Environmental Factors, Life Events and Coping Abilities Toni C. Antonucci and James S. Jackson
The Multidisciplinary Team and Day Care Provision Martin Orrell and Kunle Ashaye
The Lundby Study Mats Bogren, Cecilia Mattisson and Per Nettelbladt
Environmental Factors, Life Events and Coping Abilities Toni C. Antonucci and James S. Jackson
The Multidisciplinary Team and Day Care Provision Martin Orrell and Kunle Ashaye
 Training Requirements for Old Age Psychiatrists in the UK Susan Mary Benbow and Aparna Prasanna
Training Requirements for Old Age Psychiatrists in the UK Susan Mary Benbow and Aparna Prasanna
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


