Fig. 41.1
Manganese toxicity in total parenteral nutrition. Axial (a, b) and sagittal (c, d) T1-weighted MRI images show patchy hyperintensity within the bilateral basal ganglia, cerebral peduncles, and anterior pituitary (arrows)
41.4 Differential Diagnosis
Besides excess total parenteral nutrition, a variety of conditions can produce T1 shortening in the basal ganglia, including hepatic encephalopathy (refer to Chap. 2), hypoxic ischemic injury (refer to Chaps. 3, 29, and 40), hypertensive hemorrhage, mineralizing angiopathy (refer to Chap. 19), hypoparathryroidism, pseudohypoparathyroidism, Fahr disease (refer to Chap. 19), Cockayne syndrome (Fig. 41.2), neurofibromatosis type 1 (Fig. 41.3), and neurodegenerative Langerhans cell histiocytosis (Fig. 41.4), among other conditions. In addition to clinical history, other imaging findings may help differentiate these conditions from the effects of manganese deposition. The differential diagnosis for T1 shortening in the anterior pituitary may include pituitary apoplexy (Fig. 41.5), although this has an acute presentation and appears as a mass on imaging. Ultimately, the history of hyperalimentation in manganese toxicity versus the presence of finding beyond the basal ganglia in the other conditions is key for elucidating the diagnosis.
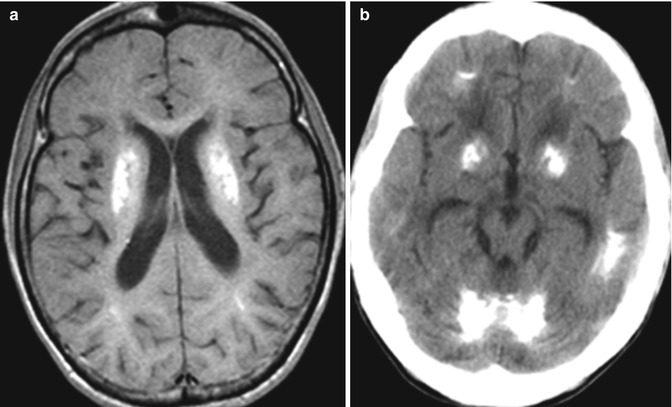
Fig. 41.2




Cockayne syndrome. Axial T1-weighted MRI (a) shows hyperintensity within the bilateral basal ganglia. Axial CT image (b) shows extensive cerebral calcifications
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
