Chapter 35 Metastatic Brain Tumors
• A metastatic brain tumor means that the patient has stage IV cancer, with median survival of under 1 year.
• When a patient presents with a new brain metastasis, without a known primary site, the chance of finding the primary tumor during the patient’s lifetime is approximately 50%.
• As long as brain metastases undergo some form of treatment, the vast majority of patients will succumb to progression of systemic disease as opposed to brain metastases.
• Therapies for brain metastases are roughly equivalent, with local recurrence rate of 40% to 50% at 1 year. Therefore, the choice of therapy must be tailored to the individual patient, taking into account Karnofsky performance scale (KPS) score, medical comorbid conditions, systemic disease status, number of metastases, size and location of metastases, and symptoms.
• It is essential that treatment decisions for this lethal disease be made as a multidisciplinary team of oncologists, radiation oncologists, and neurosurgeons, as well as the patient and the patient’s family.
The histology and epidemiology of the primary cancer are the principal determinants of the frequency of cerebral metastases. Although the most common cancers diagnosed in adults in the United States are colorectal, prostate, breast, and lung, the two of these with the greatest proclivity to spread to the brain are lung and breast. In decreasing order of relative frequency, the majority of cerebral metastases are due to lung, breast, melanoma, renal, and colon cancers. Primary lung cancer accounts for 30% to 60% of all cerebral metastases. Lung cancer is more frequently diagnosed in males, and as a result, primary lung cancer is the most common cause of cerebral metastases in males. Brain metastases from lung cancer are often synchronous at diagnosis. Breast cancer accounts for 10% to 30% of all cerebral metastases and is the most common cause of cerebral metastases in females. Unlike brain metastases from lung cancer, breast metastases to the brain are more often metachronous. Melanoma accounts for 5% to 20% of all cerebral metastases, while renal and colon cancer each account for 5% to 10% of cerebral metastatic disease. The tendency of a primary cancer to metastasize to the brain has a distinct order of relative frequency. The frequency of cerebral metastases for melanoma is greater than 50%, but the low incidence of melanoma relative to other cancers accounts for its lower overall relative frequency of all cerebral metastases. Lung cancer has the second highest overall tendency to metastasize to the brain. The frequency of cerebral metastases for lung cancer is 20% to 60%, but there is variability in the frequency of cerebral metastases based on lung tumor type. Small cell lung cancer and lung adenocarcinoma tend to metastasize to the brain more frequently than other types of lung cancer. Breast cancer has the third highest overall tendency to metastasize to the brain, with a frequency of 20% to 30%.
Clinical Presentation and Diagnostic Studies
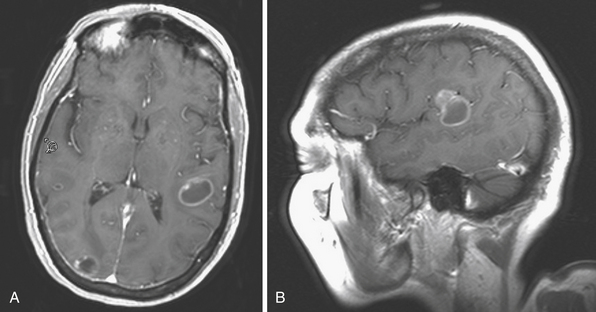
The best imaging tool for cerebral metastases is contrast-enhanced MRI (Figs. 35.1 and 35.2). On nonenhanced T1-weighted sequences, cerebral metastases generally appear isointense or hypointense. Certain metastases with intrinsically short T1, such as melanoma (due to the ferromagnetic melanin within the tumor), can appear hyperintense. Hemorrhage within the tumor will appear disorganized, with atypical evolution, and is best evaluated on T2-weighted gradient echo (GRE) sequences. On nonenhanced T2-weighted sequences, cerebral metastases generally appear hyperintense, but can be variable. Similarly, on FLAIR (fluid-attenuated inversion recovery) sequences the appearance of cerebral metastases can be variable, but is generally hyperintense. Both FLAIR and T2-weighted images usually demonstrate marked vasogenic edema. Tumor cysts and surrounding edema appear markedly hyperintense. The vast majority of cerebral metastases will enhance. On contrast-enhanced T1-weighted sequences cerebral metastases show strong enhancement in variable patterns. Cerebral metastases usually do not show restriction on diffusion-weighted imaging (DWI) sequences and exhibit elevated apparent diffusion coefficient (ADC) values. The differential diagnosis of cerebral lesions with imaging characteristics similar to cerebral metastases includes abscess, encephalitis, malignant glioma, radiation necrosis, thromboembolic stroke, demyelinating disease, and resolving hematoma. Multiplicity of lesions or location in the posterior fossa may increase the likelihood that the lesions are metastatic, rather than primary.
< div class='tao-gold-member'>
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


