Fig. 3.1
Methanol intoxication. Axial non-contrast CT image (a) demonstrates bilateral symmetrical putaminal and subcortical white matter hypoattenuation. Axial FLAIR (b), DWI (c), and T2*-weighted (d) MRI sequences performed 4 days later show symmetrical putaminal and subcortical white matter FLAIR hyperintensity with diffusion restriction. T2* imaging confirms the presence of associated putaminal hemorrhage. The patient did not survive
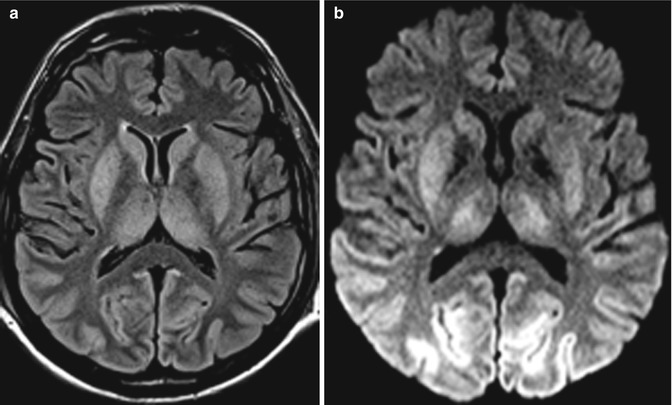
Fig. 3.2
A 60-year-old man with cerebral hypoxic injury from cardiac arrest. Axial FLAIR (a) and DWI (b) MR images show bilateral symmetrical basal ganglia and thalamic and occipital lobe cortical T2 hyperintensity and diffusion restriction
Emergent management of acute methanol ingestion involves initial resuscitation, enhanced elimination via dialysis, competitive inhibition of alcohol dehydrogenase using enteral or intravenous ethanol or fomepizole, and treatment of the metabolic acidosis. In spite of treatment, mortality rates are extremely high, particularly for patients with seizure or coma on presentation.
3.4 Differential Diagnosis
Bilateral putaminal necrosis can be seen in other conditions. However, when a patient presents with initial visual disturbance with imaging revealing bilateral putaminal and subcortical white matter abnormalities, methanol intoxication should be strongly considered.
Hypoxic injury: Brain injury patterns are variable depending on the severity and duration of hypoxia. Symmetrical basal ganglia T2 hyperintensities with diffusion restriction typically occur in severe hypoxic injury. However, this is often accompanied by loss of gray-white differentiation of the cerebral cortex on CT and/or cortical T2 hyperintensities and diffusion restriction on MRI; such cortical changes are not typically associated with methanol intoxication (Fig. 3.2).
Viral encephalitis: Flavivirus infections such as Japanese encephalitis, West Nile fever, and Murray Valley fever typically demonstrate symmetric involvement of the deep gray matter structures. On MRI, this appears as swelling and T2 hyperintensity of these structures (Fig. 3.3). Restricted diffusion and intralesional hemorrhage may also be observed. Other sites that may be involved include the substantia nigra, red nucleus, pons, hippocampi, cerebral cortex, and cerebellum, depending upon the particular virus.