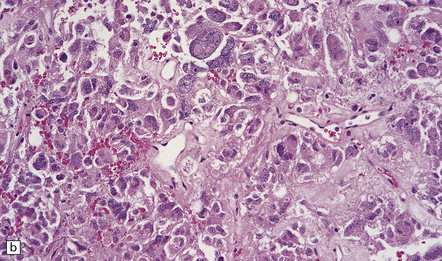
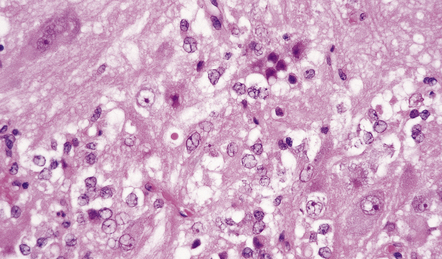
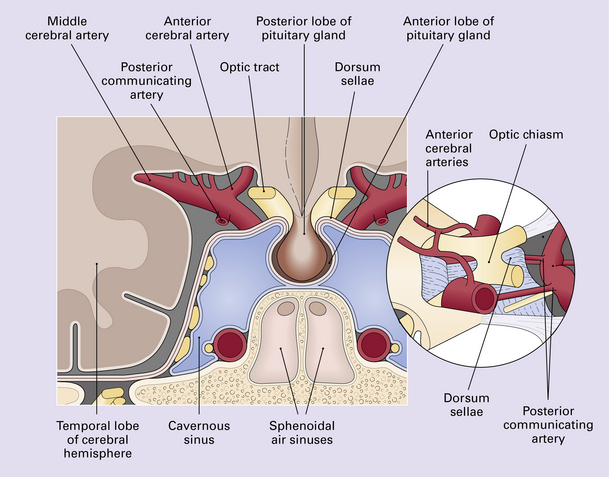
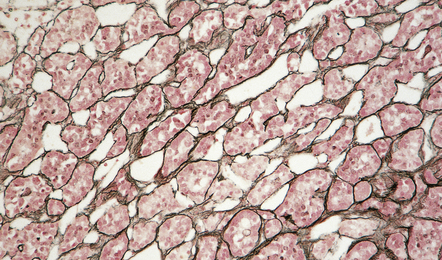
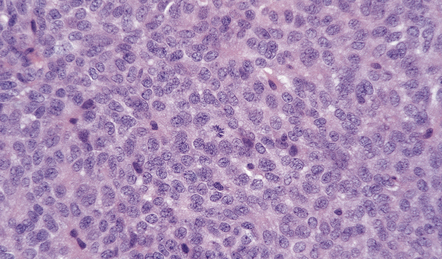
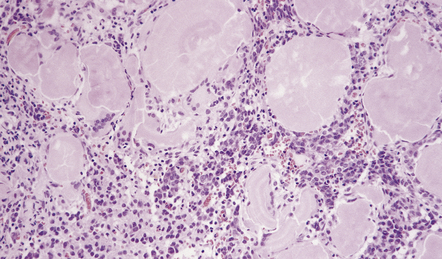
44 Neoplasms in the region of the pituitary fossa may arise in the pituitary gland itself, the sphenoid bone that surrounds the fossa, or the suprasellar region (Figs 44.1, 44.2). Structures in the suprasellar region and adjacent to the pituitary fossa include the hypothalamus, optic chiasm, nasal sinuses, and cavernous sinuses and their contents. 44.2 Schematic illustration of the types and sources of neoplasm that can affect the pituitary gland. Common neoplasms in this region are: Uncommon neoplasms in this region are: The pituitary gland weighs about 600 mg and consists mainly of the adenohypophysis (anterior lobe) and the neurohypophysis (posterior lobe) (Figs 44.3–44.6); the pars intermedia is poorly developed in man. 44.3 Hormonal cell type is mediated by transcription factors and estrogen receptors. 44.4 Normal adenohypophysis. 44.6 Normal neurohypophysis. Pituitary adenomas are derived from secretory cells in the adenohypophysis. Some adenomas secrete peptides in an unregulated manner and may therefore produce abnormal endocrine effects in addition to causing mass effects in the region of the pituitary fossa (Fig. 44.7). 44.7 Pituitary adenoma. Secretory cells in the adenohypophysis synthesize six major peptide hormones: The histology of pituitary adenomas is varied (Table 44.1). Many adenomas consist of small, oval, or polyhedral cells. These may be arranged in monotonous sheets or show a variety of acinar, papillary, trabecular, or other patterns (Figs 44.9–44.11). The nuclei of neoplastic cells are generally round or oval and contain the stippled chromatin typical of neuroendocrine neoplasms. Tiny nucleoli may be evident. Cytologic pleomorphism and mitotic figures may be present, but do not necessarily signify aggressive biologic behavior (Fig. 44.12). Invasion of local structures (Fig. 44.13), particularly the dura, is not infrequent, even by adenomas with bland cytologic features. 44.10 Pituitary adenoma. 44.11 Pituitary adenoma composed of two populations of cells. 44.12 Pituitary adenoma. (a,b) 44.13 Entrapped hypothalamic neurons at the invading edge of a suprasellar adenoma. Dystrophic calcification and eosinophilic (amyloid) bodies are strongly associated with prolactinomas (Fig. 44.14). Long-term treatment of prolactinomas with bromocriptine before surgical resection produces fibrosis.
Neoplasms in the region of the pituitary fossa
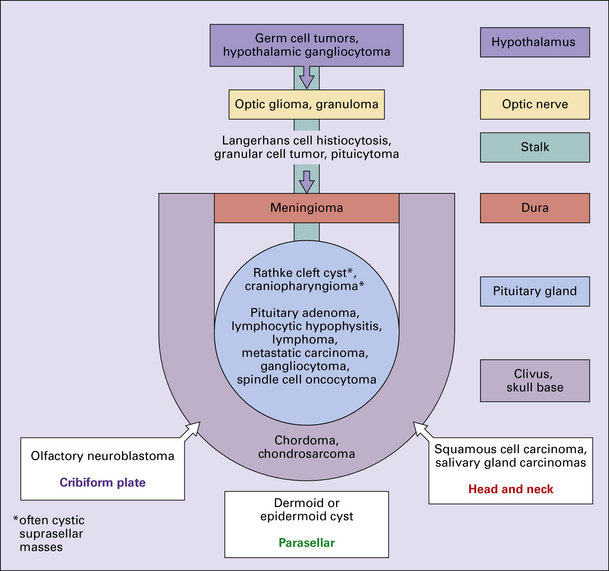
 LOCALIZATION IN THE DIFFERENTIAL DIAGNOSIS OF PITUITARY REGION LESIONS
LOCALIZATION IN THE DIFFERENTIAL DIAGNOSIS OF PITUITARY REGION LESIONS
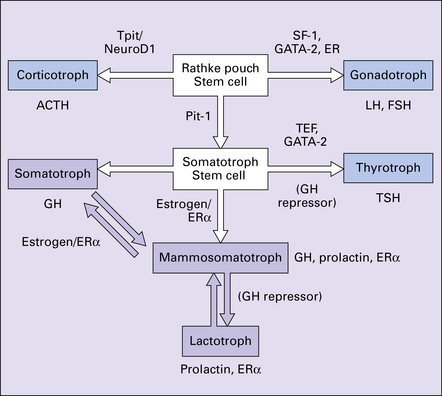
ERa, estrogen receptor alpha; FSH, follicle stimulating hormone; GATA-2, GATA binding protein 2; GH, growth hormone; (GH repressor), postulated growth hormone repressor; LH, luteinizing hormone; NeuroD1, neurogenic differentiation 1; Pit-1, pituitary transcription factor 1; SF1, steroidogenic factor 1; TEF, thyroid embryonic factor; TPit, pituitary restricted transcription factor; TSH, thyroid stimulating hormone.
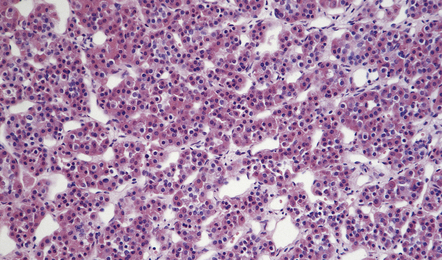
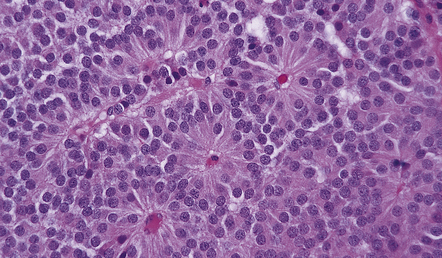
Nests of round or polyhedral cells, and an intervening network of vascular sinusoids are evident.
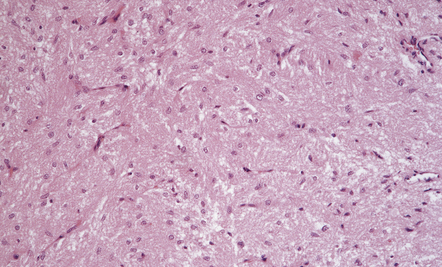
This consists of non-myelinated hypothalamohypophysial nerve fibers and a meshwork of capillaries adjacent to which the fibers terminate. Also present are specialized astrocytes (pituicytes).
PITUITARY ADENOMAS
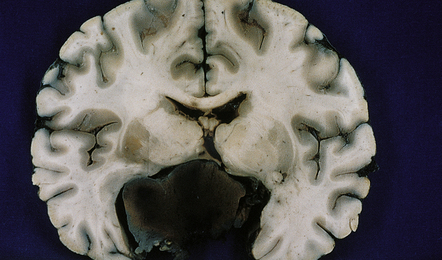
Large, hemorrhagic pituitary adenoma producing distortion of surrounding structures.
 Somatotrophs synthesize growth hormone (GH).
Somatotrophs synthesize growth hormone (GH).
 Lactotrophs (mammotrophs) synthesize prolactin (PRL).
Lactotrophs (mammotrophs) synthesize prolactin (PRL).
 Corticotrophs synthesize corticotropin (ACTH).
Corticotrophs synthesize corticotropin (ACTH).
 Thyrotrophs synthesize thyrotropin (TSH).
Thyrotrophs synthesize thyrotropin (TSH).
 Gonadotrophs synthesize follicle stimulating hormone (FSH) and luteinizing hormone (LH).
Gonadotrophs synthesize follicle stimulating hormone (FSH) and luteinizing hormone (LH).
MACROSCOPIC APPEARANCES
MICROSCOPIC APPEARANCES
 The commonest neoplasms in the region of the pituitary fossa, and represent 10–15% of intracranial neoplasms.
The commonest neoplasms in the region of the pituitary fossa, and represent 10–15% of intracranial neoplasms.
 Have an incidence ranging from 1–15/100 000 in different series.
Have an incidence ranging from 1–15/100 000 in different series.
 Most common in the third to sixth decades.
Most common in the third to sixth decades.
 Show a female:male ratio of approximately 2:1 in younger patients.
Show a female:male ratio of approximately 2:1 in younger patients.
 May present acutely with mass effects when they undergo infarction or hemorrhage.
May present acutely with mass effects when they undergo infarction or hemorrhage.
 PITUITARY ADENOMAS WITH INCREASED RISK FOR AGGRESSIVE BEHAVIOR
PITUITARY ADENOMAS WITH INCREASED RISK FOR AGGRESSIVE BEHAVIOR
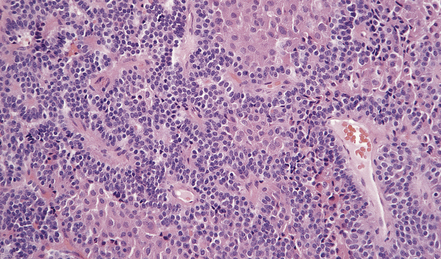
A vascular network is seen between cells, some of which have formed pseudorosettes.
The larger cells were immunoreactive for GH.
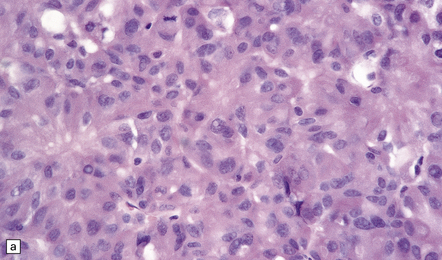
Cytologic pleomorphism and rare mitotic figures may be present and do not necessarily signify aggressive behavior.
Adenomas containing neoplastic ganglion cells are recorded but are very rare.
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Neoplasms in the region of the pituitary fossa















 PITUITARY PEPTIDES
PITUITARY PEPTIDES

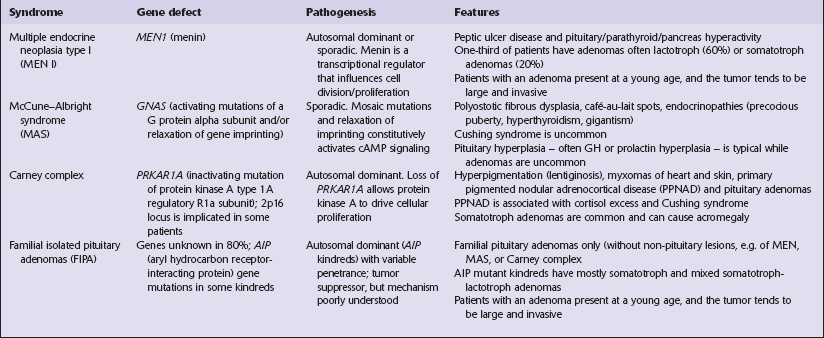
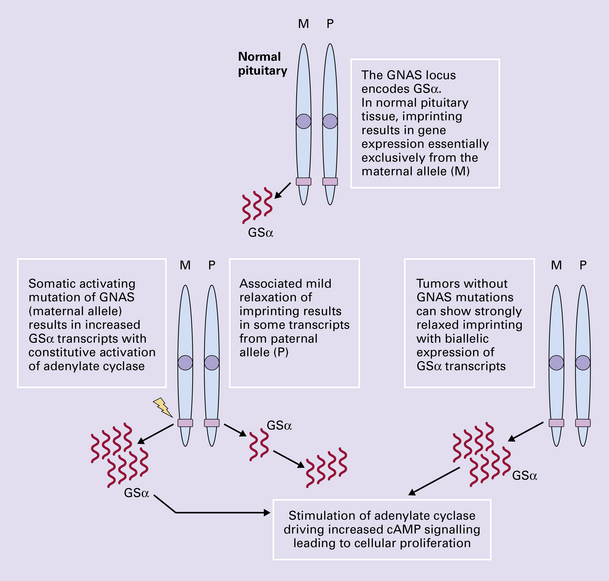
 GENETICS OF SPORADIC PITUITARY TUMORS
GENETICS OF SPORADIC PITUITARY TUMORS





 PITUITARY ADENOMAS
PITUITARY ADENOMAS




















Only gold members can continue reading. Log In or Register to continue

