Neuropsychiatric Approach to the Psychiatric Inpatient
Neuropsychiatric Approach to the Psychiatric Inpatient
Fred Ovsiew
Evan D. Murray
Bruce H. Price
This chapter focuses on the neuropsychiatric approach to patients admitted to inpatient psychiatric units. Its goal is to help clinicians construct rational evaluations to identify organic factors in their patients’ illnesses. “Neuropsychiatry” designates the psychiatric subspecialty area devoted to the psychological and behavioral consequences of organic brain disease. The term organic was dropped from the official nomenclature with the advent of Diagnostic and Statistical Manual of Mental Disorders Fourth Edition (DSM-IV), and wisely so insofar as the decision recognizes that the consequences of brain disease are manifold and cannot be lumped together as an “organic brain syndrome.” The primary goal of the framers of recent versions of the DSM, however, was to “retire”1 the term organic so as to eliminate “any implication that the nonorganic disorders are without a biological basis”2 [p. 127].
The word has not stayed “retired,” to judge by questions from colleagues. They know that some, but not all, individual patients with mental disorders can be shown to have brain disease by current diagnostic instruments: the history, the physical examination, the cognitive examination, neuropsychological examination, brain imaging, electroencephalography (EEG), examination of the cerebrospinal fluid (CSF), and so on. The continued vernacular usage acknowledges that the knowledge base and clinical skills required to diagnose and manage psychiatric patients with disorders such as epilepsy, traumatic brain injury, and autoimmune brain disease are different from those needed for the care of patients with idiopathic mental disorders. The distinctiveness of this specialty area and the overlap of neuropsychiatry with behavioral and cognitive neurology have recently been validated by the development of a credential in Behavioral Neurology and Neuropsychiatry (see http://www.ucns.org/go/subspecialty/behavioral/certification).
In asserting the distinctiveness of the neuropsychiatric approach, by no means do we deny a basis in biology to schizophrenia or depression or mania or any other idiopathic psychiatric syndrome. Neuropsychiatric understanding of organic mental disorders may well be able to cast light on the biology of the idiopathic disorders, although reasoning by similarity of phenomenology has important limits.3 Nor do the present authors assert that once an organic factor is discovered the remainder of the case is moot. Although a neuropsychiatric evaluation may lead to a diagnosis implying a specific treatment that promptly abolishes the condition and eliminates any need for further psychiatric care, such cases are not characteristic of the present authors’ practices. More commonly, the organic factors in the case feature among others that also need to be taken into account. The neuropsychiatric approach elaborated in this chapter is not meant to “scoop” other approaches and does not replace them.
Management of patients with known brain disease admitted to the psychiatric unit is discussed in Chapter 17, and the management of delirious patients is discussed in Chapter 18. General medical conditions in organ systems other than the brain commonly occur in patients with psychiatric illness and frequently contribute to psychiatric morbidity. These conditions and the appropriate general medical evaluation of the psychiatric inpatient are discussed in Chapter 4. In this chapter, the neuropsychiatric bedside evaluation (history, physical examination, and cognitive examination) and the use and interpretation of ancillary investigations (neuroimaging, EEG, CSF examination, genetic testing, metabolic testing, and neuropsychological assessment) are discussed. Guidance for neuropsychiatric evaluation in several common clinical contexts on the general psychiatric inpatient unit is then provided.
Taking the Neuropsychiatric History
Obtaining an adequate neuropsychiatric history requires an understanding of common organic factors in psychopathology and their clinical manifestations. Provided here is a sketch of these elements of the history. Fuller discussion of the comprehensive neuropsychiatric history is available elsewhere.3, 4, 5
Atypical features of the psychiatric history should raise the question of organic origin, although it is also true that organic mental disorders can closely mimic their idiopathic counterparts. An unusual age of onset, an unusually acute onset or rapid pace of progression, the absence of a family history in a disorder (such as bipolar mood disorder) that is highly familial, or an atypical response or lack of response to treatment should lead the examiner to pursue focused inquiry about neuropsychiatric issues. Similarly, the presence of somatic symptoms such as headache, somnolence, incontinence, or altered coordination or gait should be red flags for the diagnostician. A review of neurologic symptoms along with attention to the past medical history should form part of routine psychiatric history taking (see Table 5.1). In general, correlation of the psychiatric history with organic disease benefits from specificity in regard to the brain disease: not just “stroke,” but embolic stroke involving right parietal lobe, and so on. The development of psychiatric symptoms in the context of major medical illness, such as cancer, systemic autoimmune disease, or an immunocompromised state, should not be attributed to the obvious psychosocial stress of illness without full consideration of possible organic pathogenesis.
Neuropsychiatric history taking regarding development begins with the patient’s gestation. Inquiry should cover abnormalities in the mother’s pregnancy, labor, and delivery and go on to include perinatal illness (such as any illness that kept the patient in the hospital immediately after birth) and early developmental milestones (such as the age of walking and talking). Childhood illnesses, especially those affecting the brain, should be reviewed. These developmental factors are of demonstrated importance in the major psychiatric disorders.6, 7, 8 In patients with epilepsy, the diagnostician should inquire about the occurrence of febrile convulsions in childhood. The patient’s school performance provides important information about intellectual capacity; not only the overall level (such as whether special education was required) but also anomalies or unevenness in performance should be ascertained. Early athletic skills provide information about developmental achievement. The patient’s handedness should be established by inquiry about hand use for actions including writing, using a scissors, brushing the teeth, and so on.
Among acquired illnesses, either in childhood or adulthood, traumatic brain injury and epilepsy require special mention, because of both their prevalence and their well-established relation to psychiatric symptoms. A screening question about traumatic brain injury is appropriate for virtually every psychiatric patient. Significance of head injury is generally marked by loss of consciousness and the severity of brain trauma indicated by duration of unconsciousness and the length of time between injury and recovery of ongoing memory function (posttraumatic amnesia). Traumatic brain injury is of probable significance in the histories of patients with a number of psychiatric disorders, including (to name two that may be of surprise to psychiatrists) borderline personality disorder and perpetration of domestic violence.9, 10, 11 More information about the psychopathology of traumatic brain injury is offered in Chapter 17. Attention to the details of the injury is important in part because attribution of psychopathology to head injury by patients and families may rest less on a demonstrable connection than on their understandable wish to find some explanation for mysterious and disabling symptoms. The clinician will have to make a judgment about the connection, a judgment that should be based on clinical data, starting with the history.
In regard to epilepsy, too, the clinician should gain specific information about the nature of the epileptic syndrome, the frequency of seizures (under best and worst control), the phenomena of the seizure itself (including auras, if present), and the treatment. Much of the psychiatric literature about epilepsy has concerned itself with temporal lobe epilepsy, but the connection of epilepsy to psychopathology is not limited to this syndrome. For example, the syndrome of juvenile myoclonic epilepsy (JME) appears to have characteristic cognitive and personality correlates.12,13 History taking in patients with limbic epilepsy should not be confined to the symptoms typical of the major psychiatric disorders, because more specific symptoms—such as hypergraphia, hyposexuality, and preoccupation with mystical or cosmic matters—are thought by some to be characteristic correlates of this form of epilepsy.14,15 In general, the clinical phenomena of neuropsychiatric illness may not be fully captured in the syndromes of DSM-IV, and the examiner should be on the lookout for data beyond the usual history checklists. Fitting the organic mental disorder into a DSM category by brute force is inadvisable.
TABLE 5.1 SOME FEATURES IN THE HISTORY AND REVIEW OF SYSTEMS WITH LEADING IMPLICATIONS FOR NEUROLOGIC DISEASE RELEVANT TO BEHAVIOR
System
Symptom
Possible Implications (not a Comprehensive List)
General
Weight loss
Neoplasm, endocrinopathy
Decreased energy
Systemic disease
Fever, chills
Systemic or CNS infection
Arthritis
Connective tissue disease, infection
Head
New or altered headache
Space-occupying lesions, many others
History of trauma
Subdural hematoma, postconcussion syndrome
Eyes
Chronic visual impairment
Ocular or posterior hemispheric disease (visual hallucinations possible with either location)
Episodic visual loss
Vascular disease
Diplopia
Brainstem disease
Ears
Hearing loss
—
Nose
Loss of olfactory sensitivity
Local nasal disease, head injury, subfrontal meningioma
Mouth
Oral lesions
Nutritional deficiency, autoimmune disease, self-injury from seizure
Skin
Rash
Autoimmune disease, Lyme disease, infection
Birthmarks
Phakomatoses
Cardiovascular
Heart disease
Risk of cerebrovascular disease
Hypertension
Risk of cerebrovascular disease
Arrhythmia
Risk of embolic disease
Sleep
Sleepwalking/talking
Dementia with Lewy bodies
Daytime sleepiness
Sleep apnea, narcolepsy
Motor
Focal weakness
Stroke, neoplasia
Gait disorder
Hydrocephalus, white-matter disease, movement disorder
CNS, central nervous system.
Case Vignette
A young woman was seen for neuropsychiatric consultation after an admission for video-EEG monitoring required by her poorly controlled JME. During the admission, she required detoxification from large doses of alprazolam, which she was allegedly taking for myoclonus. Features of “borderline personality disorder” were thought to be recognized; other diagnoses previously attributed to her were schizophrenia and bipolar mood disorder. During the neuropsychiatric inquiry, her father reported that she had always been emotionally labile and easily frustrated (quite unlike her healthy sister), and he volunteered that she had never been able to get jokes because she did not understand (he searched for the right word) “irony.” She performed adequately or poorly in regular school classes and had menial jobs after high-school graduation. For several years before consultation, she had a clear depressive syndrome. No manic or psychotic phenomena could be identified. The neurologic examination was unremarkable. The cognitive examination disclosed particular difficulty with spontaneous word-list generation to a semantic stimulus and with a working memory task. These personality and cognitive features were considered typical of JME.
Especially in late-life psychiatric illness, history taking should seek evidence of cognitive impairment, which is sometimes subtle or overshadowed by florid mood or psychotic symptoms. Questions about forgetfulness, getting lost, and impairment of skills of everyday independent functioning are relevant. Of equal importance is the recognition of abnormal social behavior or personality change typical of organic brain disease. Such features are often described only by a family member and remain unrecognized by the patient. Patients may show alteration of social comportment, such as eating with the fingers at the dinner table; loss of the sense of humor; lack or coarsening of emotional responses to ordinarily affecting situations, such as the death of a relative; disinhibited sexual or other appetitive behavior; or apathy with loss of initiative without the self-denigrating ideation or pervasive low mood of the depressive state. The apathy syndrome deserves particular attention because of its similarity to depression yet phenomenological, pathophysiologic, and pharmacologic differences from that syndrome.16
Taking the family history can be done either disease-by-disease (“does anyone in the family have a psychiatric disorder?”) or family member-by-family member (ideally constructing a family tree in the process).5,17 The latter method is more sensitive, but the two methods can be combined in the clinical interview. Some neuropsychiatric illnesses are commonly familial (such as frontotemporal dementia), and the presence or absence of a family history is then an important clue to diagnosis.
The Cognitive Examination
On the basis of the unsystematic observations, the present authors believe that most psychiatric inpatients undergo a cognitive assessment limited to tests of orientation and perhaps memory, or at most the performance of a brief standardized screening test such as the Mini-Mental State Examination (MMSE). Not infrequently, the record of this testing is limited to a checkmark in a box labeled “memory” or “language,” without further reference to how the function was assessed. In this section, the domains of cognitive function and their bedside assessment are reviewed and screening instruments and their utility and drawbacks are surveyed. The authors argue for the centrality of assessment of executive function in the hospitalized psychiatric patient and provide guidelines for its performance.
COGNITIVE MODULES AND THEIR ASSESSMENT AT THE BEDSIDE
To listen properly to the heart and interpret the heart sounds and murmurs, the examiner must understand the anatomy of the cardiac chambers and the physiology of the circulation of the blood. Similarly, the assessment of cognition depends on an understanding of brain anatomy and mental function. Rote application of routine tests—“Name the last 4 presidents”—will not allow the examiner to use information from the cognitive examination to construct a brain-based formulation of cognitive deficits. A comprehensive discussion of the anatomy of cognition and behavior is beyond the scope of this chapter but has been addressed elsewhere.18,19
The essential concept of cognitive modularity entails that certain domains of function are relatively independent of others, with dedicated input and output streams and the possibility of derangement separate from other deficits.3 The concept does not necessarily imply distinct anatomic sites as the substrates of processing modules, and in fact contemporary theorists consider that individual cognitive functions depend on a distributed network of brain sites, any of which may also be involved in other processing functions (“selectively distributed processing”). Further, any probe of cognitive function results in the deployment of multiple modules; for example, a putative test of memory also requires language and focused attention. For these reasons, inference from clinical examination to brain lesion can be made only on the basis of a comprehensive assessment of multiple domains of cognition, by a process of “triangulation.”
Although every cognitive examination should address multiple modules as well as nonmodular cognitive functions, a comprehensive examination cannot be recommended for every psychiatric inpatient. Not only would the time requirements be excessive and the yield unreasonably low but also the psychiatric state of the patient on admission would often preclude valid testing. The goal of initial assessment at the bedside is to identify patients with deficits relevant to their functional capacity and patients who require further evaluation. At times the assessment will have to be repeated as the patient’s psychiatric state changes.
The cognitive modules assessable by bedside examination include language, memory, and visuospatial function. In addition, attention, which is subserved by a highly distributed system, should be assessed. Assessment of the cognitive state is extensively described in other texts and is merely sketched here.4,20 Executive cognitive function has a special place in the assessment of psychiatric patients and is discussed at greater length in the next section.
Attention
Attentional function can be divided into the maintenance of sustained attention, or arousal; the capacity for focused attention, or concentration; and higher forms of attentional behavior such as the capacity for divided attention or the ability to inhibit automatic attention that verge on or form part of the concept of executive cognitive function, which is discussed in detail in the subsequent text. Arousal can be gauged by the patient’s responsiveness to graded interventions: the examiner’s entering the room, voice, loud voice, touch, and so on. The clinician’s note should specify the intervention and the response rather than relying on terms such as lethargic or stuporous.
Although observations during the interview may yield an estimate of the intactness of the patient’s attentional function, every patient should have some formal probe of attention; all other cognitive functions depend on attention to some degree. Simple tasks serve well, such as forward digit span, counting backward from 20, or giving in reverse order the days of the week or the months of the year. On the MMSE, serial subtraction of 7s or spelling “WORLD” in reverse assesses this domain. Giving the letters of “WORLD” in alphabetic order is a similar probe.21 The patient’s capacity for sustained attention to external stimuli can be assessed by asking the patient to signal each time the examiner says the letter “A” during a list of randomly produced letters: “B, A, R, L, A, A, etc.” The more difficult tasks (such as giving the months in reverse) require the patient to inhibit the more usual response (in that instance, giving the months in forward order) and to that extent represent tasks of executive function.
Language
Bedside examination of language should start with attention to the patient’s spontaneous speech considered as a linguistic performance. That is to say, the examiner must deliberately focus on the syntactic, semantic, and prosodic aspects of speech, as against the meaning, affect, or narrative structure of the patient’s output. Spontaneous speech can be fluent, with normal length of phrases and normal prosodic contour, or dysfluent, with effortful, slowed, and agrammatic output. Word-finding difficulties, circumlocution, and paraphasic errors also should be listened for.
In addition to deliberate attention to spontaneous speech, the examiner can test naming, comprehension, repetition, reading, and writing. This discussion is confined to a brief description of such testing; full discussions can be found elsewhere.20,22 Naming can usually be tested by confrontation, using items at hand: “what is this (sleeve, thumb, pen, etc.) called?” Comprehension should be tested by commands that require little verbal or motor output, such as yes/no questions (“am I wearing a hat?” or “is ice cream hotter than coffee?”) or requests to “point to the chair” or “point to the ceiling, then to the floor.” The degree of impairment of repetition of spoken language may be discrepant from that of spontaneous speech. Sparing of repetition suggests a lesion outside the perisylvian language areas; disproportionate impairment suggests a lesion in or deep to left parietal cortex. Repetition can be tested by asking the patient to repeat a series of phrases of increasing complexity, starting with single words and advancing to lengthy sentences. Testing of reading entails assessment of reading comprehension (not ability to read aloud); asking the patient to point to items after reading their printed names is a simple method. Writing can be assessed by asking the patient to construct a sentence. Before testing both reading and writing, the examiner is well advised to be sure of the patient’s premorbid literacy.
A thorough language examination can help to categorize an acquired disorder of language, or aphasia, although many patients have disorders that do not fit well into any established category. Fuller discussions of the classification of the aphasias can be found elsewhere.22,23 Language errors do not always indicate language system dysfunction, and knowledge of certain confounding phenomena should help the examiner of psychiatric inpatients. “Wild paraphasias” occur in delirium, sometimes with an apparent witty quality, such as the patient mentioned by Geschwind who called an IV pole a Christmas tree.24 Disturbed writing may be an especially sensitive indicator of an encephalopathic state.24 Cutting noted that an intermittent irrelevant remark in the midst of competent replies was characteristic of delirium.25 Although delirious patients may produce abnormal language, they also show confusion in performance (ideational apraxia) on nonlanguage tasks, such as everyday instrumental behaviors. Patients with psychotic thought disorder, even when incoherent, may show adequate performance on structured language tasks if their cooperation can be gained.
Case Vignette
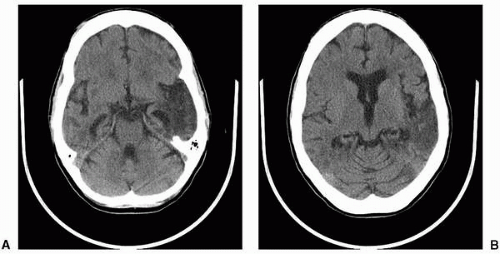
A woman in her 30s had a history of alcohol abuse and several admissions for detoxification. Approximately 8 months before consultation she presented in delirium to an emergency room (ER), where a tentative diagnosis of Wernicke encephalopathy was made. After admission, however, she developed a fever, and CSF showed a lymphocytic pleocytosis with protein elevated to 100 and normal glucose. The findings for CSF herpes simplex virus (HSV) and head computed tomography (CT) were negative. Upon discharge, she was incoherent and was sent to a nursing home, where a psychiatrist prescribed a combination of two antipsychotics on a diagnosis of “schizoaffective disorder.” At neuropsychiatric consultation, examination disclosed a cooperative and socially appropriate woman who had no elementary neurologic signs. Speech output was fluent but so full of paraphasic errors, such as “spoketal” for key and “farris” for glove, as to be incomprehensible. Comprehension was severely impaired. Clinically, she had Wernicke aphasia, not the Wernicke encephalopathy that her family had been told about. Subsequently, repeat CT (magnetic resonance imaging [MRI] could not be accomplished) showed extensive damage to the left temporal lobe (see Fig. 5.1). Antipsychotics were successfully discontinued.
Memory
Every cognitive examination should include some probe of memory, both because of its sensitivity to brain disease and because of the functional importance of memory.26 Tasks such as recalling a name and address after several minutes or recalling a list of several words tap into verbal memory function. However, the examiner should not ignore possible relative impairment or sparing of nonverbal memory, which can be ascertained by recall of figures or of objects hidden by the examiner in the examination room. A substantial discrepancy between verbal and nonverbal memory can be seen in patients with temporal lobe epilepsy and is of lateralizing significance.
▪ Figure 5.1 Left temporal lobe encephalomalacia seen on computed tomography (CT) images at two levels.
Two forms of organic memory impairment should be emphasized. One, dependent on hippocampal mechanisms, involves rapid forgetting of material; the other, dependent on frontosubcortical mechanisms, involves impairment of retrieval. To some extent, although not so well as neuropsychological assessment, bedside evaluation can identify the form of memory impairment by using cuing strategies. While everyone is better at cued than at free recall—a multiple-choice test rather than an essay test—the discrepancy is particularly large in patients with impaired retrieval. Therefore, marked improvement in memory performance with cueing by multiple choice or by a semantic cue (“it was the name of a musical instrument”) suggests dysfunction in frontal or subcortical structures.
Although relative impairment of “long-term” or “remote” memory can be identified in the neuropsychological laboratory, bedside examiners have difficulty making this distinction. Results of tests such as asking the patient to name recent American presidents have no compelling neuropsychological interpretation. Prominent forgetting of personal information, such as one’s own name, with intact capacity to learn new information (as assessed by the tasks such as those described earlier) is virtually pathognomonic of psychogenic amnesia.
Visuospatial Function
Tasks of visuospatial function tap into the capacities of the “nondominant” hemisphere, typically the right hemisphere of dextrals. Failing to ascertain whether nonverbal cognitive impairment is present is particularly problematic in psychiatric settings because of the “dominant” role of the right hemisphere in affect regulation. Copying figures or the examiner’s presentation of hand positions is a simple set of tasks that probe this domain.4 Asking the patient to bisect a line drawn by the examiner or to cross out short lines arrayed within a page may reveal the hemineglect of the patient with right-hemisphere injury; this deficit also may be apparent on the clock-drawing test (see subsequent text). However, such a gross deficit as neglecting the left half of space, while not unusual in acute right-hemisphere stroke, may not be present in patients with milder or less acute damage, so these are not the most sensitive probes of visuospatial function. Patients with deficits in this domain may also show impairment in face recognition, impairment in recognizing affect in pictured scenes or vocal intonations, impairment in encoding affect into vocal output, and route-finding impairment.
Other Aspects of Modular Processing
Although what is described in the preceding text samples the classical elements of cognitive modules of long-standing interest in behavioral neurology, other aspects of cognitive processing may be disturbed with relative specificity and may be of clinical significance. Although screening for all possible deficits is impractical, awareness of other forms of impairment may lead to appropriate investigation in situations where a history of brain injury, unusual features of the psychiatric history or examination, or physical findings raise the question of additional deficits.
For example, the discussion of language disorders above addresses only disturbances of propositional discourse, not the pragmatic or affective elements of language performance. But patients with brain injury may show deficits in appreciation of emotion as coded into speech;27 deficits in recognition of emotion in facial expression or visual scenes may occur as well. Such patients may present disturbances of affect suggestive of depression but pathophysiologically quite different from depressive states. Nothing substitutes for a broad awareness of the complex, multifarious, and at times counter-intuitive behavioral phenomena of brain disease.
SCREENING TESTS OF COGNITIVE FUNCTION
Many brief instruments have been devised to facilitate screening for cognitive deficits.28 These instruments have the advantages of being quantitative, systematic, and repeatable across occasions and venues. They vary in their intended use, and potential users must keep in mind that the requirements for effectiveness of a brief instrument on the inpatient psychiatric unit are likely quite different from those, say, in community surveys assessing the prevalence of Alzheimer disease.
No doubt the best known instrument is the MMSE.29 It has the advantage of being widely used and therefore easily compared across institutions. However, it has numerous limitations.30 Of these, perhaps the most serious for the inpatient psychiatrist is its lack of any measure of executive dysfunction. The MMSE total score is also insensitive to focal brain disorders (as against delirium and dementia, its original focus) and to mild cognitive impairment. If used on the inpatient psychiatric unit, it should be supplemented by some screen for executive dysfunction. Further, any errors—even if the total score is above the standard cutoff—should be considered an indication for further evaluation, at least by additional bedside cognitive testing.
The Modified Mini-Mental State Examination (3MSE) is an expanded instrument that includes, among other additions to the MMSE, tests of executive function.30 It contains the MMSE so that performances on the 3MSE can be compared with past or future results on the MMSE. Some instruments even simpler than the MMSE have been proposed as capable of identifying mild dementia. For example, the TE4D is an eight-item scale covering the domains of immediate recall, semantic memory, orientation, category fluency, clock drawing, and following commands.31 The Mini-Cog assesses memory and clock drawing only.32
A scale developed to identify cognitive impairment related to human immunodeficiency virus (HIV) encephalopathy, the HIV Dementia Scale (HDS), focuses on the subcortical features of mental slowing, executive dysfunction, and attentional impairment characteristic of that disorder, in contrast to the MMSE and its successors, which focus more on the cortical features characteristic of Alzheimer disease.33,34 These subcortical impairments may be especially important not to miss in patients with psychiatric disorders, because depressive states produce a picture not unlike subcortical dementia and because subcortical vascular disease may be an important cause of de novo psychiatric illness in late life. The HDS contains four elements: a memory task, a test of response inhibition using antisaccades, a test of psychomotor speed, and a visuoconstructional task. The antisaccade task starts with the patient looking straight ahead at the examiner’s face, while the examiner places one hand in each of the patient’s visual fields. The patient is asked to look at the examiner’s right hand when the examiner’s left hand moves, and at the examiner’s left hand when the right hand moves. Looking at the moving hand represents a failure of inhibition.
Several research groups have developed broader cognitive screening instruments. For example, the Montreal Cognitive Assessment (MoCA, see http://www.mocatest.org/) probes the domains of attention, verbal fluency, language, memory, and constructional ability. The Addenbrooke’s Cognitive Examination-Revised similarly explores attention, orientation, memory, language, and visuospatial function.35
Review of these instruments reveals that several make use of clock drawing. Drawing a clock has been touted as “the ideal cognitive screening test” because it is quick, provides a visual record of the patient’s performance, is relatively insensitive to cultural variables, and is sensitive to multiple domains of cognitive impairment, including executive dysfunction.36, 37, 38 To utilize clock drawing as an executive screen requires considering not only the visual-spatial elements of the performance (such as neglect of the left side of the clock face) but also the planning of the placement of the numbers and the setting of the hands. Scoring systems to capture these elements have been proposed. As a simple clinical procedure, the patient can be provided with a circle and asked to put in the numbers of the clock face while leaving out the hands. Then the examiner requests the patient to set the hands to “5 after 10,” or some other time in which the number spoken by the examiner is not the number to which the patient must point the hand. The goal of the instruction is to see whether the patient can abstract from the concrete stimulus (the number 5) and construe it in terms of a clock face (in this instance, with the little hand of the clock pointing to the 1).
EXECUTIVE COGNITIVE FUNCTION AND ITS ASSESSMENT
Executive cognitive function refers to those aspects of mental function that deploy, monitor, and inhibit elementary cognitive functions.39 These aspects include planning, reasoning, and judgment; deficits show themselves as perseveration, disinhibition, and poor adaptation of internal states and resources to the demands of the environment. Executive function can be measured neuropsychologically using tasks such as the Stroop test and the Wisconsin Card Sorting Test and identified at the bedside by probes such as motor sequencing tasks, tests of working memory, tests of response inhibition (such as go/no-go tapping tests or the antisaccade test mentioned earlier), and tests of verbal or design fluency. Asking a patient to name all the animals he or she can think of in 1 minute is a typical semantic verbal fluency task; an instruction to name all the words starting with a given letter creates a phonemic fluency task. Having the patient tap once when the examiner taps once and not tap at all when the examiner taps twice is a simple go/no-go test of response inhibition. Perseveration and impaired motor sequencing can be elicited by asking the patient to alternate between making a fist and forming a ring with the thumb and index finger, the Luria ring/fist test.
The Mental Alternation Test, or alphanumeric sequencing, is an oral version of the Trails B test. A patient who is able to count and able to recite the alphabet is asked to alternate numbers and letters: “1-A-2-B-3-C” is given as an example, and then the patient is asked to start at 1. Correct alternations are scored, with errors not counted; considering a score of 15 or above to be normal has been recommended.40,41 This is a working memory test that presumptively relies on prefrontal-subcortical function. It is very simple to administer, and the expanding data about its utility are encouraging.40, 41, 42, 43, 44
Several bedside batteries of tests of executive function have been constructed. The Frontal/Subcortical Assessment Battery includes a verbal fluency task, a go/no-go task, and a motor sequencing task.45 The Frontal Assessment Battery includes probes of abstraction, motor sequencing, verbal fluency, perseveration, response inhibition, and the grasp reflex.46 The Behavioral Dyscontrol Scale, based on the work of the Russian neuropsychologist A. R. Luria, includes go/no-go and motor sequencing tasks, probes of perseveration and echopraxia, and the alphanumeric sequencing test described earlier.47 The Executive Interview (EXIT-25), a copyrighted neuropsychological instrument, is somewhat more extensive, and more time-consuming, than the briefer batteries just mentioned.48
In addition to systematic probes, observation of the patient’s behavior during the clinical evaluation can yield data regarding executive function. For example, during the interview or physical examination the patient may demonstrate echopraxia, duplicating the examiner’s spontaneous gestures or mirroring the examiner’s movements, or may demonstrate impersistence by failing to maintain postures or eyelid closure (“peeking”). Executive function is multidimensional, that is, no single test fully interrogates executive function, so that one, several, or even all commonly used tests can be normal in the presence of executive dysfunction.
The reason that executive cognitive function is of special importance in the cognitive examination is its correlation with autonomous functioning outside the clinical setting. Executive dysfunction is associated with functional decline and behavioral disturbance in dementia,49 with the capacity to live independently in elders,50 and with insight and adaptive functioning in schizophrenia.51,52 Patients with late-onset depression and executive dysfunction (often the result of subcortical white-matter disease) show poorer outcomes than patients with similar depressive states but lacking executive dysfunction.53 No cognitive examination on the inpatient psychiatric unit is complete without attention to executive cognitive function.
The clinician should be aware, however, that real-world functioning may differ from performance on formal testing. This may be because the testing situation—quiet, structured, based on veridical perception rather than value or emotion—does not duplicate the world in which the patient lives and in fact may make up for executive deficits. This problem, so-called ecologic validity, is the stimulus for devising new methods of examination within neuropsychology.54
Only gold members can continue reading. Log In or Register to continue
 The Ins and Outs of 200 Years of Psychiatric Hospitals in the United States
The Ins and Outs of 200 Years of Psychiatric Hospitals in the United States



