CHAPTER 106 NEUROREHABILITATION
This chapter provides an overview of the rehabilitation principles used to improve function and facilitate recovery in patients with neurological injury. Numerous and varied neurological conditions manifest unique impairments. Neurorehabilitation is a diverse topic. This chapter presents a systematic approach to evaluation and implementation of general rehabilitation interventions for neurological injury. The paradigms for treatment presented focus on spinal cord injury (SCI) and brain injury models, although the treatment approaches can be applied to the rehabilitation of patients with other disorders with similar neurological sequelae. Rehabilitation programs typically consist of two parts: (1) skilled therapeutic exercise, to maximize function, and (2) prescription and incorporation of specific adaptive equipment, to facilitate optimal function, mobility, and independence.
ASSESSMENT
Initial Evaluation
Numerous disease states can cause injury to the spinal cord, including trauma, spondylosis, demyelinating diseases, tumor, neurodegenerative diseases, infection, vascular injury, and toxic metabolic disorders. There are approximately 11,000 new cases of traumatic SCI per year in the United States.1 About 700,000 people suffer a stroke each year, and stroke is currently the leading cause of serious long-term disability in the United States.2 However, numerous other disorders of brain function cause significant disability, and these patients may also benefit from directed rehabilitation therapies. Examples include encephalopathies, neurodegenerative diseases, hydrocephalus, demyelinating disease, and primary and metastatic brain malignancies. Many different types of rehabilitation programs are available for patients and are stratified in Table 106-1 according to level of medical acuity (the need for close medical supervision or nursing services) and intensity.
TABLE 106-1 Classification of Rehabilitation Programs
| Program | Medical Acuity* | Hours of Rehabilitation |
|---|---|---|
| Acute inpatient rehabilitation | High | 3 (minimum/day) |
| Day therapy (outpatient) | Low-moderate | 3-5 (usually 5 days/week) |
| Subacute rehabilitation | Moderate | 1-3 (usually 3-5 days/week) |
| Home therapy | Low | 1 (usually 2-3 times/week) |
| Outpatient therapy | Low | 1-2 (usually 2-3 times/week) |
| Extended care facility | Moderate | 1 (usually 2-3 times/week) |
* The need for close medical supervision or nursing services.
Assessment Scales
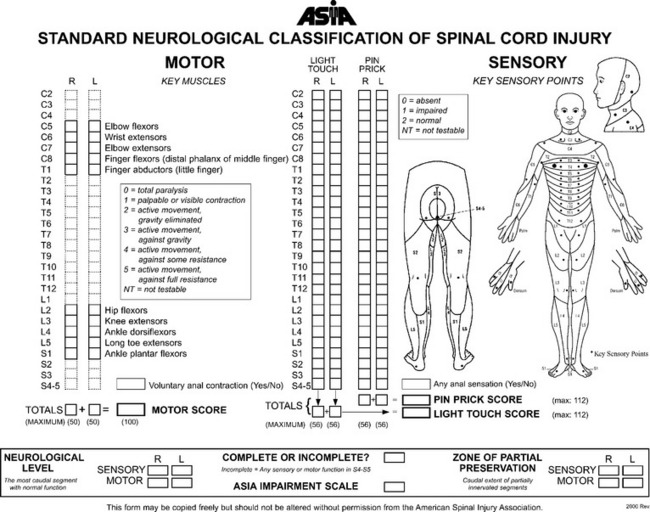
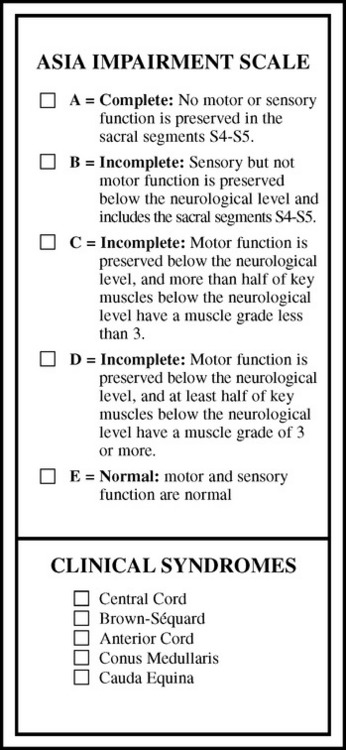
SCI assessment starts with a determination of the level and the completeness of the spinal injury. The American Spinal Injury Association has published standards for classification of SCI level (Fig. 106-1) and a grading system for completeness of neurological injury (Fig. 106-2).3 Incomplete injuries have a much better prognosis for motor recovery than do complete injuries. Since 2000, the most frequent SCI neurological category at rehabilitation hospital discharge of persons reported to the National Spinal Cord Injury database is incomplete tetraplegia (34.3%), followed by complete paraplegia (25.1%), complete tetraplegia (22.1%), and incomplete paraplegia (17.5%).1
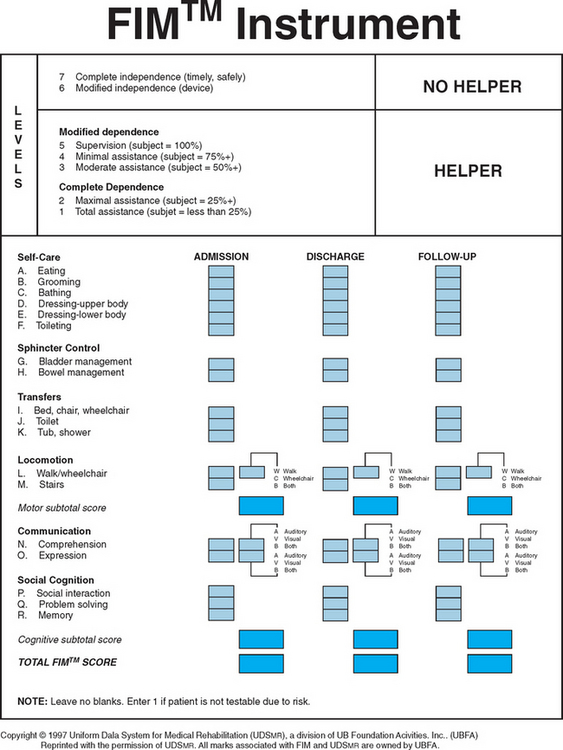
A variety of scales and assessment tools exist for evaluation of function after neurological injury. The primary initial assessment scale administered in traumatic brain injury is the Glasgow Coma Scale. The Glasgow Coma Scale numerical score reflects the depth of unconsciousness and is one of the most significant initial predictors of outcome and recovery.4 Table 106-2 summarizes some of the more commonly used scales in rehabilitation medicine. The Functional Independence Measure instrument is probably the most widely used functional assessment tool in the inpatient rehabilitation setting and can be applied irrespective of diagnosis (Fig. 106-3).
TABLE 106-2 Commonly Used Assessment Scales
| Scale Type | Scale Name |
|---|---|
| Spinal cord injury impairment | ASIA Impairment Scale |
| Stroke deficit | NIH Stroke Scale |
| Canadian Neurologic Scale | |
| Level of consciousness/cognitive function | Glasgow Coma Scale |
| (Ranchos) Level of Cognitive Function Scale | |
| Galveston Orientation and Amnesia Test | |
| Motor function | Fugl-Meyer Scale |
| Spasticity | Modified Ashworth Scale |
| Basic ADLs and mobility | Barthel Index |
| Functional Independence Measure | |
| Instrumental ADLs | Lawton & Brody Instrumental ADL Scale |
| Katz ADL Scale | |
| Depression | Beck Depression Scale |
| Hamilton Depression Scale | |
| Quality of life | Sickness Impact Profile |
| Health status | Short-Form 36 |
ADL, activity of daily living; ASIA, American Spinal Injury Association; NIH, National Institutes of Health.
ACUTE ILLNESS REHABILITION
Rehabilitation protocols should begin immediately after neurological injury, even if the patient is critically ill. One of the main goals is to minimize the effects of prolonged immobility that can be associated with severe neurological injury. In addition, quick identification of other body systems that may have been adversely affected facilitates immediate implementation of treatment schemes and thus minimizes the potential for morbidity. Table 106-3 outlines the various areas that require assessment.
TABLE 106-3 Acute Illness Rehabilitation Principles
| Rehabilitation Measure | Principle |
|---|---|
| Musculoskeletal | Prevention of contractures with range-of-motion exercise, stretching, positioning, splints, and footboards |
| Pulmonary | Incentive spirometry, chest percussive therapy, pulmonary toilet |
| Swallowing | Bedside or video swallowing evaluation to assess aspiration risk |
| Skin | Frequent repositioning (every 2 hours), padding of bony prominences, pressure-reducing mattresses, and specialized beds |
| Bowl | Assessment of continence, constipation, neurogenic bowl |
| Bladder | Assessment of continence, check for infection, implementation of indwelling or intermittent catheterization |
| DVT prophylaxis | Subcutaneous heparin, sequential leg compression devices, compression garments, encouraging mobility and active calf exercises |
| Confusion | Reducing sedating medications, installing restraints or net bed for patient safety |
DVT, deep vein thrombosis.
FUNDAMENTAL REHABILITATION INTERVENTIONS
Flexibility
Flexibility is an integral component of most rehabilitation schemes. Flexibility exercises can reduce contractures, reduce muscle pain, and decrease spasticity. Prolonged gentle passive stretching is preferred over aggressive forced or ballistic stretching,5 which can tear myofibrils and supportive connective tissue, leading to increased pain. The pain and microscopic tearing associated with aggressive stretching techniques reduces the potential for progressive gains in flexibility. Heat application before stretching or a gentle aerobic warmup (if the patient is able to perform this) improves blood flow to the muscle and improves tissue elasticity. Ideally, stretches should be held for at least 30 seconds6 and, for optimal results, repeated twice a day.
Strengthening
For patients with profound motor impairment, neuromuscular electrical stimulation can be used to facilitate strengthening, and in patients with SCI, such stimulation has been demonstrated to reduce disuse-related atrophy.7 However, caution should be exercised with use of neuromuscular electrical stimulation in patients with myopathy because it may result in exhaustion of the myopathic muscle.
The primary physiological processes by which normal muscles achieve greater strength are muscle hypertrophy and enhanced neuromuscular control. In the initial 2 weeks of any strengthening program, the improvements in strength are related less to muscle hypertrophy than to enhanced neuromuscular control8; thereafter, muscle hypertrophy is the predominant factor. In the patient with neurological injury as the cause of weakness, improvements in strength also depend greatly on the processes of neurological recovery. The mechanisms of recovery vary, depending on the precise nature and extent of neurological injury.9 For example, central reorganization of motor control (neural plasticity) occurs after stroke, and collateral sprouting of motor unit nerve endings occurs in peripheral neurological injury.
Balance, Coordination, and Neuromuscular Reeducation
Rehabilitation of an extremity where injury has significantly impaired voluntary motor control is likewise challenging. Selection of a rehabilitation strategy depends, in part, on whether the limb is flaccid or spastic. Treatment in the flaccid extremity focuses on exploiting synergy patterns of muscle activation to facilitate voluntary movement. In the spastic extremity, techniques such as the Bobath neurodevelopmental training method or proprioceptive neuromuscular facilitation are used along with gentle prolonged stretching to decrease spasticity and improve motor control by using specific tone-reducing postures and movement patterns.10,11 Biofeedback with surface electromyography can be used to facilitate neuromuscular reeducation.11 Orthoses and adaptive equipment are commonly used thoroughout the rehabilitation process to facilitate improvements in extremity function. These are discussed in more detail in subsequent sections.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


