CHAPTER 22
Neurourology
I. Micturition
A. Involves coordination of central nervous system (CNS) and peripheral nervous system (PNS)
B. Initiated by cerebral cortex
C. First step is relaxation of striated external urethral sphincter (EUS) by inhibition of somatic efferents
D. Inhibition of sympathetic efferents
E. Activation of parasympathetic efferents causing bladder contraction and urethral smooth muscle relaxation
1. CNS
a. Pontine micturition center (PMC) or Barrington nucleus mediates normal micturition reflex by coordinating activity of detrusor and urethral sphincter.
b. Afferent signals from the lower urinary tract are received in the periaqueductal grey matter (PAG) and relayed to insula.
c. Anterior cingulate gyrus controls micturition reflexes.
d. Prefrontal cortex makes voluntary voiding decisions.
2. PNS
a. Somatic nervous system S2 to S4, pudendal nerve
i. Striated external urinary sphincter
(A) Striated sphincter contraction via nicotinic cholinergic receptors
(B) Preganglionic efferent nerves exit from S2 to S4.
(C) Nerve bodies are located in Onuf’s nucleus.
(D) Nerve fibers travel with pudendal nerve to EUS, where they modulate voluntary sphincteric control.
(E) Release of acetylcholine stimulates nicotinic cholinergic receptors in EUS, causing contraction (storage).
b. Autonomic nervous system
i. Parasympathetic pathways S2 to S4, pelvic nerve
(A) Detrusor contraction via muscarinic receptors
(B) Preganglionic efferent nerves exit from S2 to S4.
(C) Travel in pelvic nerve to inferior pelvic plexus located adjacent to the bladder to modulate bladder contractions
(D) Release of acetylcholine stimulates muscarinic acetylcholine receptors (M3) in bladder, causing contraction (emptying).
ii. Sympathetic pathways T11 to L2, hypogastric nerve
(A) Smooth muscle relaxation via B-adrenergic receptors
(B) Preganglionic efferent nerves exit from T10 to L2.
(C) Ganglia are paraganglia (next to vertebrae), preganglia (between vertebrae and end organ), or peripheral ganglia (in end organ).
(D) Nerves travel within hypogastric nerve to the inferior pelvic plexus, where they modulate urethral smooth muscle contraction and inhibit parasympathetic activity.
(E) Release of norepinephrine stimulates beta-3 adrenergic receptor in bladder, causing relaxation (storage).
(F) Release of norepinephrine stimulates alpha-1 adrenergic receptors in involuntary sphincter, causing sphincter contraction (storage).
II. Voiding Dysfunction Classification System
A. Failure to store
1. Bladder: overactivity (idiopathic, neurogenic), decreased compliance, increased sensation
2. Outlet: stress urinary incontinence, intrinsic sphincteric deficiency
3. Both
B. Failure to empty
1. Bladder: underactive, acontractile
2. Outlet: anatomic (tumor, detrusor sphincter dyssynergia, stricture), functional (dysfunctional voiding, Fowler’s syndrome [failure of urethral sphincter relaxation in young women], primary bladder neck obstruction)
3. Both
III. Location of the Neurologic Lesion and Effect on Bladder (Figure 22.1)
A. Suprapontine (including cerebral cortex): detrusor overactivity with bladder and sphincter synergy, normal bladder sensation, usually adequate emptying
B. Pons to spinal cord above S2 (upper motor neuron damage): detrusor sphincter dyssynergia and spastic paresis of lower limbs
C. S2 to S4 (lower motor neuron damage): acontractile detrusor, flaccid striated sphincter, flaccid lower limbs
D. Peripheral nerves: acontractile detrusor and absent bladder sensation
IV. Evaluation
A. History
1. Urinary symptoms
a. Frequency, volumes of urination, urinary incontinence
b. Hesitancy, force of urinary stream, incomplete emptying
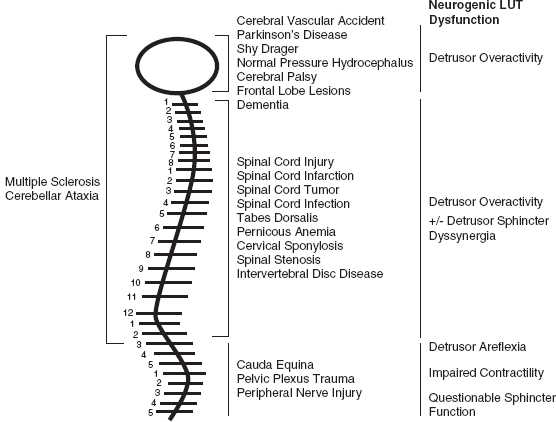
Figure 22.1 Symptoms associated with level of neurologic lesion.
2. Review of symptoms
a. Gastrointestinal (GI): frequency and consistency of bowel movements
b. Need to splint—use fingers to press on the vagina or perineum to aid in obtaining a sense of complete evacuation during defecation, manual disimpaction.
B. Examination
1. General: appearance, nutritional status, upper extremity dexterity
2. Abdominal examination: presence of masses, assess for constipation
3. Neurologic examination: should include assessment of perineal sensation
4. Pelvic examination in women
a. Evidence of leakage with cough
b. Presence of pelvic organ prolapse beyond the hymen
c. Strength of anal sphincter, presence of hemorrhoids
C. Testing
1. Voiding diary: record volume voided, fluid consumed, incontinence episodes, pads/diapers for 3 days
2. Postvoid residual
3. Noninvasive uroflow
4. Urodynamic study with or without video (video to assess outlet)
a. In patients with spinal cord injury (SCI), wait until spinal shock resolves (~12 weeks).
5. Cystoscopy
6. Upper tract imaging: voiding cystourethrogram (assess for reflux), renal ultrasound (US) (assess for hydronephrosis, stones, renal scarring)
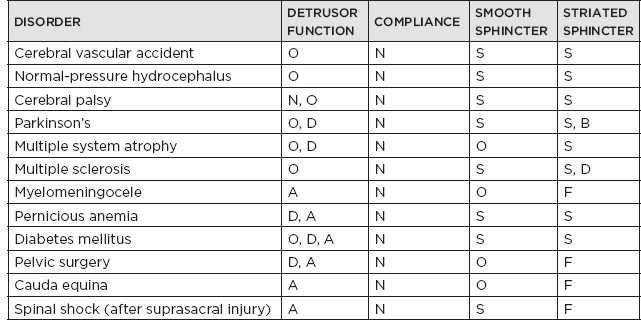
V. Urodynamic Findings Associated With Common Neurologic Disorders (Table 22.1)
A. Detrusor function: normal (N), overactive (O), acontractile (A), detrusor underactivity (D)
B. Detrusor compliance: normal (N), decreased (D), increased (I)
C. Smooth sphincter activity: synergic (S), dyssynergic (D), open (O)
D. Striated sphincter activity: synergic (S), dyssynergic (D), bradykinetic (B), impaired voluntary control (I), fixed tone (F)
VI. Management
A. Upper urinary tract preservation/preservation of renal function
B. Absence of infection
C. Adequate bladder capacity at low intravesical pressure (to prevent upper tract damage)
D. Adequate emptying at low intravesical pressure
E. Urinary control
Table 22.1 Detrusor Function, Sphincteric Function, and Bladder Compliance Associated With Common Neurologic Diseases
F. Failure to store
1. Bladder: overactive bladder idiopathic
a. Bladder retraining
b. Dietary modification
c. Pelvic floor physical therapy
d. Pharmacotherapy
i. Anticholinergics: oxybutynin, tolterodine, trospium chloride, fesoterodine, solifenacin, darifenacin
ii. β-3 agonists: mirabegron
e. Refractory treatments (fail pharmacotherapy)
i. Sacral nerve stimulation (InterStim)
ii. OnabotulinumtoxinA 100 units
iii. Posterior tibial nerve stimulation
iv. Augmentation cystoplasty
2. Bladder: neurogenic detrusor overactivity
a. Bladder retraining
b. Dietary modification
c. Pelvic floor physical therapy
d. Pharmacotherapy
i. Anticholinergics: oxybutynin, tolterodine, trospium chloride, fesoterodine, solifenacin, darifenacin
e. β-3 agonists: mirabegron
f. Refractory treatments (fail pharmacotherapy)
i. OnabotulinumtoxinA 200 units
ii. Posterior tibial nerve stimulation
iii. Augmentation cystoplasty
3. Outlet: stress urinary incontinence
a. Pelvic floor physical therapy
b. Incontinence pessary
c. Intra-urethral bulking agents
d. Mid-urethral synthetic sling
e. Pubovaginal fascial sling
G. Failure to empty
1. Bladder: underactive, acontractile
a. Timed, double voiding
b. Intermittent self-catheterization (ISC)
c. Suprapubic tube
d. Sacral nerve stimulation (only in nonobstructive idiopathic urinary retention)
e. Catheterizable stoma
f. Indwelling Foley catheter (last resort)
2. Outlet:
a. Pelvic floor physical therapy
b. ISC
c. OnabotulinumtoxinA 100 units into urinary sphincter (off-label usage)
d. Sacral nerve stimulation in Fowler’s syndrome
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


