
This has parallels with consent to medication and engagement in psychotherapies and occupational activities, particularly in the forensic setting.
Ethical considerations must take account of possible benefits of EM, including potential increases in users’ autonomy and acceleration of clinical progression through secure services and back to the community, as well as cost effectiveness of treatment programs. A research group was established to investigate quantitative and qualitative analysis of the impact of EM. Several projects are completed or nearing completion, and our research group aims to publish data on these projects in the near future. In the UK, GPS-based EM is currently being used by two other medium secure forensic units and for some individuals with severe neurodevelopmental disorders. Several psychiatric intensive care units are also investigating its potential use. It is anticipated that the next Code of Practice for the UK Mental Health Act will include specific guidance on the use of EM in detained patients.
Closed Circuit Television (CCTV)
Background
Closed circuit television (CCTV) is the use of video cameras to transmit a signal to a specific place, on a limited set of monitors. CCTV has become widespread in UK society, where it is estimated that there are now over 4 million CCTV cameras [28]. A major report into effectiveness of CCTV in the UK [29] suggested that the majority of the schemes evaluated did not reduce crime, nor did CCTV schemes make people feel safer or change their behavior. However, these conclusions were qualified in the same report as being too simplistic, pointing to the fact that mechanisms that increase recorded crime rates can work alongside those that reduce crime, cancelling each other out.
Use of CCTV in psychiatry was pioneered in 1953 by Tucker for mass therapy in California because of “the increasingly difficult situation of overcrowding and understaffing faced by most mental hospitals,” and by Wittson for psychiatry education in Nebraska from 1955 [4]. In the UK, CCTV cameras have featured as a surveillance tool in mental health hospitals since 2002 [29] and have become commonplace in both general and psychiatric hospitals.
General and forensic psychiatric hospitals have identified several potential uses of CCTV. Many of these are practical considerations, such as monitoring of visits, protection of staff during searches, and easier monitoring of ward and patient areas where sightlines are suboptimal. CCTV can also assist robust prosecution of offending behaviors by patients or staff, and the review of serious incidents for training purposes. In this way, it can make both staff and patients safer, and act as a deterrent toward inappropriate practice by staff. This is particularly pertinent in the wake of a recent enquiry into abuse of vulnerable patients by staff in the UK [30].
CCTV can be used to monitor a range of more specific risks. For example, it may be employed in supervised confinement to monitor patient behavior more closely. Monitoring may be particularly difficult in the early stages of supervised confinement, when a severely unwell patient may be violent and hostile. In this way, risk of self-harm or injury can be minimized. Longitudinal assessment using CCTV may allow staff to get a clearer picture of the patient’s level of agitation prior to face-to-face assessment. CCTV footage of disturbed or aggressive behavior could also be reviewed with a patient when he or she is relatively well, as part of overall treatment and planning.
Limitations of CCTV
Some research and development on CCTV in psychiatric settings has been undertaken, and comprehensive guidelines have been devised for its use [31]. However, very little research has assessed the impact of the cameras on patients and nursing practices. Desai [32] expressed concern about several aspects of the use of CCTV, including ethical considerations, the potential to distort the reality of what is happening in a ward environment, and reduction in face-to-face contact between staff and patients. In another article [28], the same author pointed to other potential negative consequences of CCTV, including “function creep” (applications for CCTV that did not feature in the original mandate), increased paranoia, and creation of a “panoptican” – an all-seeing eye reigning over staff and patients alike, as described by Foucault. A recent report was critical of use of CCTV in patients’ bedrooms in an Irish psychiatric hospital without patients’ consent [33].
Use of CCTV in a high secure hospital (Broadmoor)
Standard CCTV has been used routinely at Broadmoor Hospital for over a decade. There is extensive perimeter CCTV, which is part of the standard security measures for a high secure hospital. Recent years have seen the progression of its use. All higher dependency wards at Broadmoor hospital have CCTV covering communal areas (but not patients’ bedrooms). Footage from CCTV cameras is used to support usual security protocols in real time. CCTV has also been used to provide evidence toward convictions for violent behavior. For practical reasons, such as the costs of storing large volumes of footage, footage is routinely kept for six weeks only. Should any suspected offending be identified, that CCTV footage is stored longer for further potential use.
Requests can also be made to retain CCTV footage for other reasons, such as reflective practice and supervision. Footage has also been used in team reviews of particular incidents, as well as supervision of clinicians. High secure hospitals occasionally require planned responses from specially trained staff using shields, for example, to remove a weapon from a disturbed patient. These teams have been using handheld CCTV footage of their interventions for training and record-keeping purposes since 2012. In these ways, CCTV can be seen to aid risk management by securing prosecution of offending behaviors and for developing the skills of clinicians.
Body-worn video. Body-worn video (BWV; Figure 31.3) is a form of CCTV. Small cameras are attached to the front of the wearer. Sound can be recorded. Used by selected UK police force units since 2005 with a view to increasing both officer and civilian accountability, use of BWV by the police has become more widespread and will likely increase further in light of recent policing controversies in the United States [34]. In 2014, Broadmoor Hospital undertook the first trial of body-worn CCTV cameras in a UK hospital. One of the criticisms by patients in qualitative appraisal of the pre-existing CCTV system was the absence of sound recording, which they believed led to a lack of context when reviewing the visual images. BWV was introduced partly to address this issue, as well as to provide an extension of CCTV footage used for risk management in the unit.
The BWV device is not in constant use on the ward, nor is it in constant use when it is being worn. When on the ward, a member of nursing staff wears a small, clearly marked CCTV camera which is usually switched off, and has a red LED to clearly show when it is recording. It also records sound. To date, use of BWV has been judged as useful by staff members, who report a reduction in incidents when it is present. The overwhelming majority of patients supported its continued use, and the trial has been extended to other parts of the hospital.
Future potential use includes review of post-incident footage to assess the nature of the incident, quality of crisis management and contingency plans, and integration into patient clinical records to demonstrate both risk behaviors and examples of good coping skills. Qualitative and quantitative data on BWV and CCTV are being collected on an ongoing basis, with a view to publication in future articles.
Motion detector technology
Background
Motion detector or motion sensor technology refers to any instrument used to detect moving objects, particularly people. Several technologies are available, including passive infrared (PIR), microwave, ultrasonic, tomographic motion detector, and video camera software. A wide range of uses is possible, including computer game software (e.g., Wii and Xbox) and “smart lighting” systems for street, home, and office lighting. In healthcare settings, the potential applications are considerable. To date, motion sensor technology has been used in assisted rehabilitation [35], monitoring of cardiac and respiratory conditions [36], assistance of home living in the elderly and cognitively impaired [37,38], and monitoring of diabetes [39]. Personalized ambient monitoring (PAM) uses motion sensor (and other) technology, which is worn by patients in their homes, to collect physiological and environmental data. This information is then used to develop models of prodromal phases of illness, based on level of activity and physiological measures. Potential applications in mental health include monitoring of those with bipolar disorder, depression, schizophrenia, and dementia [40].
Use of motion detector technology in a high secure hospital
In forensic and general psychiatric hospitals, patients are usually subjected to regular checks during the night. This involves recording of a patient’s breathing rate, heart rate, and oxygen saturation. These checks typically require light to properly visualize the patient and his or her breathing, leading to either patients being regularly woken up or checks regularly being poorly done, neither of which is acceptable.
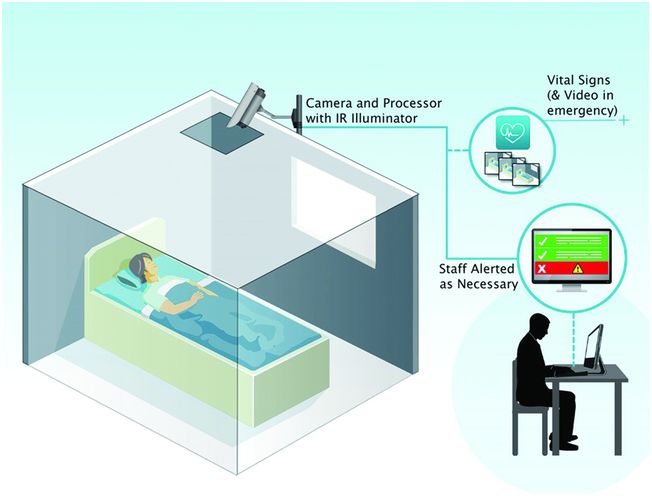
To address this problem, Broadmoor Hospital has recently collaborated with a UK medical technology company (Oxehealth) to develop an adapted CCTV system that can work in total darkness and provide constant contactless monitoring, without the need for a patient to wear any monitoring equipment or physically co-operate with the process. This could prove extremely useful, as it means the patient does not have to be woken or disturbed at night. As well as the practical benefit to the patient of not having to be disturbed at night, this can aid risk management through improving therapeutic effect of appropriate sleep patterns.
The technology involved is twofold. First, the CCTV cameras employ infrared light to detect movement. This technology has been available for some time and is commonly used in night-time CCTV or night vision security cameras. Second, to process the information, Oxehealth developed a novel set of algorithms, known as Oxecam (Figure 31.4). The algorithms use techniques such as image-based photoplethysmography and movement tracking to extract information automatically from the camera data. No manual processing is required. The system can run continuously, gathering extended sections of monitoring data rather than spot-check measurements. If the latest measured data indicate a cause for concern, the system can raise an alarm automatically for staff to review the data and intervene if necessary. Bespoke hardware is not needed, as widely available cameras can be used. As well as monitoring patients in visible light (indoor lights or sunlight), the system can operate in total darkness by using invisible infrared illumination. This camera-based technology has been demonstrated in previous clinical studies involving adults undergoing hemodialysis [41] and pre-term infants in a neonatal intensive care unit [42]. The device currently being trialed can be placed in a ceiling, in secure CCTV housing.
Broadmoor Hospital is also currently piloting a separate system, which develops algorithms based on motion sensor data to identify prodromes of aggression and violent episodes. The device tracks the movement of every person on the ward. CCTV is not involved, and individuals are not identifiable. Alongside data on movement, data about the time, nature, and location of any significant incident that occurs on the ward are collected. Algorithms will be developed with the aim of identifying early warnings of patterns of movement that are known to precede significant clinical events, alerting staff when such patterns occur, and allowing a proactive approach to be taken to any developing situation.
Conclusions
New technologies offer a broad range of benefits in forensic psychiatry services. These include less restrictive options for patients, improved accountability of both staff and patients, less invasive testing, improved automated record keeping, and better assurance reporting.
A common theme of the developments described here is the use of technology to improve the completeness and accuracy of data used by clinicians to make decisions. In the complex interplay of risk management and patient recovery, such accuracy is vital. Another common thread is that each of these strategies supports and improves current clinical approaches rather than drastically changing them. Some technologies are cost-neutral, or cost-saving, and for those that are not, the falling price and improving quality should reduce barriers to uptake.
Services that utilize technologies also need to be aware of limitations. EM may be seen as unduly restrictive by patients and advocates. Evidence for its use remains limited, and technical failures may render it ineffective in some cases. CCTV in psychiatric settings also lacks a robust evidence base, and concerns about reality distortion, “function creep,” and impact on therapeutic relationships should be borne in mind. It is important that services retain the correct balance when deciding in what ways technological advances will be used, and in what ways they will not. It is vital that the types of technological innovations described in this article should be subject to thorough evaluation that addressed cost effectiveness, qualitative analysis of patients’ attitudes, safety, and ethical considerations.
Related posts:
 Assessment of aggression in inpatient settings
The psychiatrist’s duty to protect
The psychopharmacology of violence: making sensible decisions
Implementing an ecological approach to violence reduction at a forensic psychiatric hospital: approaches and lessons learned
Serotonin and impulsive aggression
Crime, violence, and behavioral health: collaborative community strategies for risk mitigation
Assessment of aggression in inpatient settings
The psychiatrist’s duty to protect
The psychopharmacology of violence: making sensible decisions
Implementing an ecological approach to violence reduction at a forensic psychiatric hospital: approaches and lessons learned
Serotonin and impulsive aggression
Crime, violence, and behavioral health: collaborative community strategies for risk mitigation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


