Occipital Fixation Techniques: Keel Plate versus Screws through Connectors versus Wire versus Bolt
Occipital Fixation Techniques: Keel Plate versus Screws through Connectors versus Wire versus Bolt
Mukund I. Gundanna
The occipitocervical junction is a challenging region to approach due to anatomical constraints, both osseous and neurovascular. The region can also be daunting to the surgeon who does not commonly perform surgery in this area. However, the dorsal approach is a reliable way to obtain fixation of the occiput to the dorsal elements of the cervical spine. It involves standard dissection and techniques that are familiar to the spine surgeon. There are some anatomical differences in neurovascular anatomy compared to the subaxial spine, but with careful dissection, the potential for injuries to these structures can be decreased.
The occipitoatlantoaxial (OAA) articulation is highly mobile. It is held together more by ligamentous and capsular attachments than by geometrical bony articulation. As such, trauma and disorders of soft tissue structures can cause significant mechanical instability, leading to neurologic instability. In cases of instability, it is often best to achieve a solid, bony fusion. The dorsal approach is well suited for this because of the extensile nature of the approach and the relative ease of access to osseous structures for spinal fixation and for decortication and bone grafting.
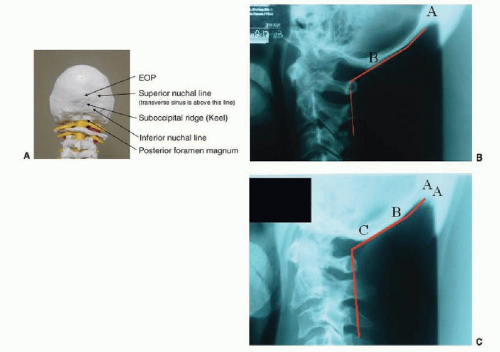
The occiput has a very strong osseous structure. Fixation in the occiput is almost always reliable. The exposure is relatively straightforward and is described later in this chapter. The key landmark is the foramen magnum inferiorly and ventrally and the external occipital protuberance (EOP) centrally and superiorly. The superior nuchal line extends laterally from this point. Approximately 2 cm below the superior nuchal line, and 15 mm above the dorsal foramen magnum, is the inferior nuchal line. The suboccipital ridge (occipital keel) can be seen on the outside surface of the occiput, extending down from the EOP, connecting the nuchal lines (Fig. 137.1A-C). On the inside of the occiput, superior and lateral to the EOP, in close approximation to the inner occipital table, lies the transverse sinus. At the confluence in the midline, and going superiorly, is the superior sagittal sinus. These structures are best left unviolated. The internal occipital protuberance (IOP) lies on the opposite side of the occiput from the EOP. Above it lies the venous sinuses described above (Fig. 137.2).
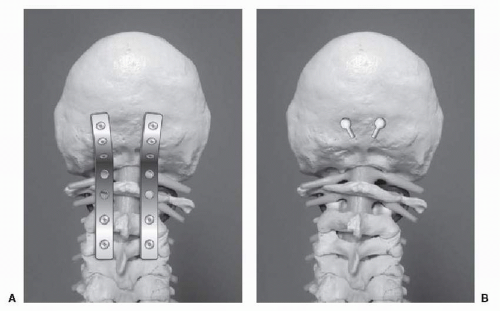
To avoid nomenclature confusion, the term wire-rod (or wire-loop) refers to occipital and sublaminar wiring connected to a U-shaped rod (or a Hartshill-type loop) (Fig. 137.3). Screw-plate refers to screw fixation of the cervical spine, connected by a long plate on each side, which extends into the occipital region for fixation (Fig. 137.4A). Bolt fixation refers to the “inside-outside” technique of using a flat-head screw and bringing it out of a drill hole from inside the occiput out and screwing it into the plate (1). The “inside-outside” technique is a type of screw-plate fixation (Fig. 137.4B). Screw-rod refers to cervical screws attached to a rod on each side. A single, separate keel plate is attached to the occiput and accepts both rods (Fig. 137.4). Regardless of whether it is screw-plate or screw-rod, this type of fixation can be called “screw-based.”
This chapter highlights some of the progress we have had with types of OAA arthrodesis with instrumentation, from rod and wires to screw-plate fixation and screw-rod (keel) fixation.
INDICATIONS
There are a number of indications for fixation of the occiput to the cervical spine. The most common reason is cranial settling leading to basilar invagination in rheumatoid arthritis (RA). There have been many radiographbased systems established to quantify basilar invagination. Generally speaking, 5 mm of cranial settling with radiographic compression is generally considered an indication to stabilize the occiput to the cervical spine (1). It is generally accepted that a dorsal atlanto-dens interval (PADI) of less than 14 mm is cause for concern (2). Less important, but still a consideration, is an atlanto-dens interval (ADI) change of 4 mm on flexion/extension. Any more than 8 mm of ADI indicates potential severe stenosis (3). Although arthrodesis can be limited to C1-C2 for pure atlantoaxial instability, fixation of the occiput is sometimes needed for better structural stability or for anatomical reasons. Traumatic atlanto-occipital dislocation, essentially an internal decapitation, is an emergent indication for OAA fixation. There are other, more unusual, situations that could cause instability and/or stenosis and are listed in Table 137.1.
Figure 137.1.A: Relevent dorsal occipital anatomy. B: Relevant physiologic lateral OC anatomy. (A) represents the EOP. (B) represents the foramen magnum. The two white lines form the bend of a typical O-C rod. The angle is 61 degrees. Note that a slight forward bend would be needed to contour the proximal portion of the plate. C: A different occipital morphology still creates similar angles. (A) the EOP. (B) the IOP that corresponds to the inferior nuchal line. The occipital ridge lies between them in the midline. C the foramen magnum. The rod angle here is 63 degrees.
Typically, an arthrodesis of the occipitocervical (O-C1) junction will eliminate approximately 30 degrees of flexion and extension. Atlantoaxial (C1-C2) fixation will eliminate approximately 40 degrees of rotation (3). As such, significant loss of range of motion should be expected. Unfortunately, this is one of the disadvantages of this procedure.
It is clear that instrumentation is highly recommended for more successful outcomes and more stability. This chapter reviews instrumentation techniques for achieving fixation of the occiput to the cervical spine in an effort to promote occipitocervical fusion.
Figure 137.2. Anatomy of the inner occipital table.
Figure 137.3. Craniectomy (7 to 15 mm resection at midline, tapering resection 1 cm in either direction) for dorsal decompression (black). Four possible 6- to 8-mm trephines for wires (lines). Alternatively, a double loop through drill holes in the EOP (gray).
Figure 137.4. A: Generic screw-plate system for O-C3 arthrodesis. B: Inside-outside technique of drilling hole and track for head-in insertion and slide.
OCCIPITOATLANTOAXIAL ARTHRODESIS TECHNIQUES
OAA arthrodesis can be performed using a variety of techniques. These have evolved over the years with technologic advances in implants and grafts. Initially, there was rib or iliac crest autograft. Later, there was cable and wire fixation through a loop placed through the occipital bone. Plate and screw fixation came next. Currently, it is often keel plate and rod fixation with segmental atlantoaxial and subaxial screw fixation that is the method of choice. Sublaminar wiring and hooks can also be used when screw placement is not possible.
PREOPERATIVE EVALUATION
A thorough preoperative evaluation is essential to maximize fixation and minimize complications. Flexion and extension laterals are important to quantify instability in patients with chronic pathology, such as rheumatoid subluxation. CT and MRI studies will help delineate the anatomy. In cases where occipital screws are contemplated, a CT scan is especially valuable to help plan the length of screws and to minimize penetration into the cranium. In cases of trauma where vertebral artery injury is suspected, MR or CT angiography will help to define vessel anatomy and pathology.
In certain situations where the cervical pathology may benefit from traction, placement in halo traction before imaging would help determine reducibility of the pathology. Patients may arrive in some sort of fixation, such as a halo or cervical collar, or may have chronic pathology and not be wearing any supportive devices.
Prior to any dorsal cervical procedure with instability or spinal cord compression, it is imperative that the operative team be well-versed in prone spine surgery. Lateral fluoroscopy or image guidance during the surgery is beneficial. The anesthesiologist may want to do an awake fiberoptic intubation using regional and topical anesthesia. In this case, the intubation should be done with the patient in a hard cervical collar, and neurologic function should be assessed before they are induced and turned prone. In the case of preoperative halo fixation, the patient will arrive in the operating room with the halo on. Portions of the halo may be left connected during induction, which provides more stability and less movement of the spine during the procedure. An adjunct to this would be the placement of somatosensory evoked potential monitoring with motor evoked potential (MEP) monitoring leads in all four extremities. Baseline potentials can be obtained prior to positioning, following positioning, and during the surgery to maintain safety from positioning and through the procedure.
In those patients without a halo, there are several options for fixation during the surgery. Two-point skull tongs can be placed prior to positioning. With the head on a horseshoe headrest, traction can be set to the desired weight. Alternatively, a Mayfield three-point skull tongs system can be placed before positioning and then secured to the bed afterward. Regardless of technique, it is important to make sure that a cervical collar is on and snug prior to turning the patient. The author prefers three-point fixation with the Mayfield fixed to the table. During the procedure, if a reduction or change in alignment occurs, care must be taken to make sure that the cervical spine does not “swan neck.” If this occurs, the head may need to be repositioned.
For those with a halo, the ring alone can be attached to the traction, firmly attached to the bed. For very unstable spines that have been kept in reasonable alignment in the halo, portions of the halo can be maintained during the surgery to provide stability during the procedure.
Paralytic anesthetic agents should be avoided, especially in cases where spinal cord MEPs are being performed.
TABLE 137.1 Causes of OAA Instability
Congenital
Achondroplasia
Diastrophic dwarfism
Spondyloepiphyseal dysplasia
Larsen’s syndrome
Odontoid abnormalities
Morquio’s syndrome
Down’s syndrome
Skeletal dysplasias
Occipital condyle hypoplasia
Atlas hypoplasia
Iniencephaly
Hyperlaxity syndromes
Down’s syndrome
Familial cervical dysplasia
Basilar invagination
Chiari malformation
Syringomyelia
Occipitoatlantal fusion
Hypoplasia of the atlas
Bifid dorsal arch of the atlas
Odontoid anomalies
Achondroplasia
Developmental/acquired
Basilar invagination
Rheumatoid arthritis
Psoriasis
Gout
Anklylosing spondylitis
Grisel’s syndrome
Rickets
Osteogenesis imperfecta
Paget disease
Neurofibromatosis
Skeletal dysplasias
Malignancy (primary or metastatic)
Trauma
Guille JT, Sherk HH. Congenital osseous abnormalities of the upper and lower cervical spine in children. J Bone Joint Surg 2002;84A:277-288; Clark CR, Menezes AH. Rheumatoid arthritis: surgical indications. In: Herkowitz HE, ed. The spine, 4th ed. Philadelphia, PA: WB Saunders, 1999:1281-1301. Ref. (4); Menezes AH. Dorsal occipitocervical fusion: rod and wiring techniques. In: Kim DH, Vaccaro AR, Fessler RG, eds. Spinal instrumentation: surgical techniques. New York: Thieme, 2005:14—19.
Preoperative antibiotics should be given at least 1 hour prior to incision. The author prefers 2 g cefazolin preoperatively, with 1 g given every 6 hours afterward.
TECHNIQUE
A midline incision is made from the EOP distally. Typically, an incision down to C4 is necessary for adequate exposure and screw placement from the occiput to C2. Subperiosteal dissection can be made sharply or with electrocautery from the occipital bone to the inferior extent of the arthrodesis. If there is tremendous instability, clamps can be used to secure and stabilize the dorsal arch of C2.
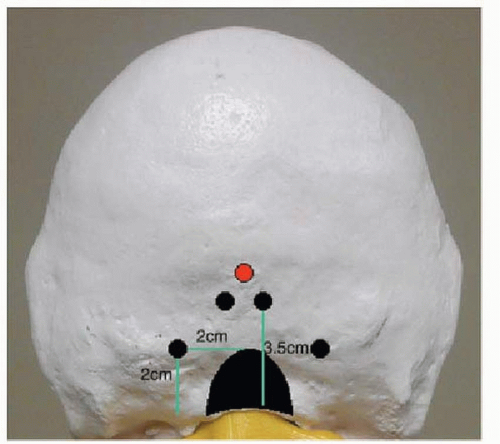
Dissection of the C1 superior arches can only proceed laterally about 10 mm in either direction to avoid injury to the vertebral arteries, which become tortuous and lie ventrally on the lateral arms of the arch at this level. As dissection on the superior aspect of C1 approaches 1 cm lateral to midline, it would be wise to not use electrocautery and instead use Penfield probes to continue dissection. The rod/loop is then brought into the field. Assuming a precontoured rod is not available, the rod can be bent to form a horseshoe. If a loop is used, it can be bent appropriately. The lateral O-C1 angle is quite significant, and the rod will have to be bent significantly in the sagittal plane. The width of the transverse arm should be about 4 cm. Ideally, this part should be placed about 3.5 cm dorsal (superior) to the foramen magnum. Each limb of the rod should extend down to at least one cervical level below the inferior extent of the arthrodesis.
After dissection with an angled instrument, the foramen magnum can be enlarged with a Kerrison punch, extending dorsally about 2 cm and laterally about 1 cm.
With the decompression complete, the wire fixation is then placed. The occiput is penetrated in two to four locations spaced equally approximately 1 cm from the foramen magnum decompression. The drill holes can be between 6 and 8 mm in diameter. Angled instruments can be use to create a safe plane over the dura to pass the wires. Wires are passed from the trephine holes through the foramen magnum opening (5). Alternatively, Wertheim and Bohlman (6) passed a loop twice through a hole drilled across at the EOP. Sublaminar wire technique can be used to fixate to C1, C2, and then distally as needed. A small laminotomy can be made laterally in C2 to keep the wires lateral at that level. Wires at C1 may need to be more medial depending on arterial anatomy. Typically, only the medial 2 cm of the arch needs to be removed to decompress the spinal cord. The lateral portions (just medial to the vertebral arteries) that remain could be wired into the construct. If more of the C1 arch has been removed for decompression, then that level will obviously not have fixation along the dorsal arch. Cables can then be tightened, starting at C2, then at the occiput. C1 arch cables cannot be tightened to the extent that the other levels can. If Songer cables are used, between 6 and 10 pounds of torque can be set on the wrench— more tension at C2 and less at C1. The occipital cables will be in the most robust bone and can be tightened more than the cervical loops (7). The surgical tools and instrumentation required for wire-rod techniques are portrayed in Table 137.2.
At this time, a thorough irrigation can be done. Next, bone and graft can be packed around the outside of the loop and over intact dorsal arches, after thorough decortication of the surrounding bone. Structural grafts can also be wired onto the bone with drill holes and wires.
Closure of the soft tissues is performed in layers. The muscle can be reapproximated with 0-Vicryl simple stitches. The fascia can be closed with O-Vicryl figure-of-eight stitches. Subcutaneous closure can be done in any standard manner.
TABLE 137.2 Wire-Rod (or Wire-Loop) Technique: Equipment and Implants
Surgical Tools and Instrumentation
4-mm titanium rod (precontoured if possible) or Hartshill loops
18- to 20-gauge titanium cables
Titanium cable clamps and crimpers
Rod bender and cutter
Rod benders, including in situ benders
Drills with guides that have stops
Surgical tools and retractors for approach, decompression, and decortication
As long as fixation was reasonable, cervical collar immobilization for 4 to 6 months would be reasonable. If fixation is suboptimal, continued halo immobilization for at least a few weeks would be prudent (5).
Only gold members can continue reading. Log In or Register to continue
Jun 29, 2016 | Posted by drzezo in NEUROLOGY | Comments Off on Occipital Fixation Techniques: Keel Plate versus Screws through Connectors versus Wire versus Bolt

 Developmental Anatomy of the Normal Cervical Spine
Developmental Anatomy of the Normal Cervical Spine
 Pediatric Spinal Cord Injury
Pediatric Spinal Cord Injury
 The Incidence and Risk Factors Associated with Destructive Spondyloarthropathy (DSA)
The Incidence and Risk Factors Associated with Destructive Spondyloarthropathy (DSA)
 Cervical Facet Prosthesis
Cervical Facet Prosthesis
 Unilateral Facet Dislocation: Surgery versus Nonoperative Treatment
Unilateral Facet Dislocation: Surgery versus Nonoperative Treatment



