The Incidence and Risk Factors Associated with Destructive Spondyloarthropathy (DSA)
The Incidence and Risk Factors Associated with Destructive Spondyloarthropathy (DSA)
Norimitsu Wakao
Makoto Yanase
Naoki Ishiguro
Yukihiro Matsuyama
Shiro Imagama
Zenya Ito
Recent advances in hemodialysis have prolonged the life span of renal failure patients. However, the incidence of complications has increased as well. Several complications, for example, bone cyst, tenosynovitis, renal osteodystrophy, synovitis, and soft tissue calcification, occur in the musculoskeletal tissues of these patients. Destructive spondyloarthropathy (DSA) is among this group of complications.
DSA was reported as a serious complication of longterm hemodialysis by Kunz et al. (1) for the first time in 1984. It is radiographically characterized by severe narrowing of the intervertebral disk space and erosions and cysts of the adjacent vertebral plates, with minimal osteophyte formation. DSA often causes severe neurologic deficits with a commensurate negative impact on the patients’ quality of life.
The pathogenesis and natural history of DSA are not fully understood, but it is well known that amyloidosis, which consists of β2-microglobulin, plays an important role in the development of DSA (2, 3, 4, 5, 6 and 7). In addition, prior reports suggest that the DSA lesions are predominantly detected in highly mobile areas, such as C5-C7 and L3-L5 (8). Ohashi et al. (9) explained this phenomenon by noting that the collagen that has been injured by mechanical stress has a high affinity for β2-microglobulin. Therefore, it is presumed that a prior disorder of spine alignment facilitates progression of DSA in hemodialysis patients. This chapter describes the relationship between the type of DSA and cervical spine alignment, as well as the incidence of DSA and associated risk factors.
OBSERVATIONS
The authors investigated cervical plain radiographs of 616 patients who underwent hemodialysis. One hundred and twenty-three patients had DSA lesions, while 493 had no evidence of DSA
DSA GROUP
The DSA patients averaged 62.2 years of age and included 50 females and 73 males. Patients averaged 52.3 years of age when hemodialysis had begun and were dialyzed for a mean duration of 9.9 years. DSA patients were assigned to stages 1 to 3 according to the severity of the disease using Maruo’s criteria: Stage 1 is defined as a case exhibiting only vertebral erosion, stage 2 is defined as a case exhibiting intervertebral disk space narrowing without osteophyte, and stage 3 is defined as a case exhibiting destruction of the vertebra and instability of the spine; 8 had stage 1, 46 had stage 2, and 69 had stage 3 disease (define). Fifty-four of DSA patients required hospitalization, while 69 were treated as outpatients with conservative modalities. Among those hospitalized, 10 patients required surgical procedures and 44 patients were treated conservatively with medications, physiotherapy, or cervical brace.
NON-DSA GROUP
Of 493 patients without DSA, the average age was 60.9. This group included 290 males and 203 females. Patients averaged 52.7 years of age when hemodialysis was begun and were dialyzed for a mean duration of 8.2 years. No patients had spine surgery, but 65 patients required orthopaedic operations, consisting of 13 shoulders, 36 hips, and 16 knees surgery, while 428 were managed conservatively.
The lumbar spine bone mineral density (BMD) was measured by dual energy x-ray absorptiometry. Osteoporosis was defined as BMD less than 2 SD.
Patients in both populations were classified into four groups according to the duration of dialysis (group 1, <5 years; group 2, from 5 to 10 years; group 3, from 10 to 15 years; group 4, more than 15 years).
Multiple factors were evaluated to determine whether significant differences existed between the DSA and non-DSA populations. These included the average age when hemodialysis was begun, the average duration of hemodialysis, the existence of osteoporosis, BMD, serum β2-microglobulin level, main lesion of DSA, amyloidosis except for the spine, and the disease that required hemodialysis.
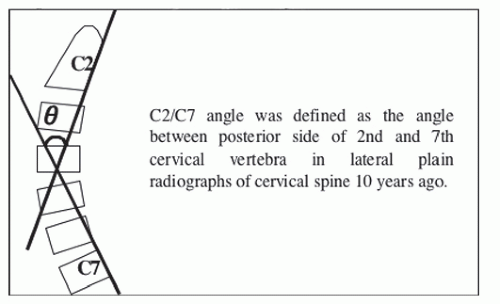
Figure 66.1. Global cervical alignment (C2/C7 angle). C2/C7 angle was defined as the angle between dorsal side of the second and seventh cervical vertebra in lateral plain radiographs (obtained 10 years prior).
Six orthopaedic spine surgeons (experience >8 years) evaluated the radiographs and regarded the presence of erosions and destruction of the vertebrae, intervertebral disk space narrowing, and spondylolisthesis without apparent osteophyte formation as DSA. All cases with DSA were classified into three stages according to Maruo’s criteria as follows (10): Stage 1, defined as a case exhibiting only vertebral erosion; stage 2, defined as a case exhibiting intervertebral disk space narrowing without osteophyte; and stage 3, defined as a case exhibiting destruction of the vertebra and instability of the spine. In addition, stage 3 was divided into four subtypes as follows: type A, defined as a case exhibiting kyphosis due to vertebral destruction; type B, defined as a case exhibiting instability of spine due to spondylolisthesis; type C, defined as a case exhibiting canal stenosis due to amyloid deposition; and type D, defined as a case exhibiting stability of spine due to spontaneous fusion of vertebras. Type C is excluded in the data presented herein because it is not identifiable by plain radiography alone. MRI is required.
TABLE 66.1 Summary of all Patients
With DSA
Without DSA
Total
n
123
493
616
Sex(male/female)
73/50
290/203
363/253
Age (mean ± SD years)
52.3 ±14.0
52.7 ±13.3
52.5 ± 13.4
The period of hemodialysis (mean ± SD years)
9.9 ± 6.8*
8.2 ±5.9
9.0 ±6.1
Osteoporosis
83(67.5%)**
282(57.2%)
365(59.3%)
BMD (mean ± SD mg/cm2)
549.9 ±138.5***
610 ±140.2
592. ± 139.8
The period of hemodialysis was statistically longer in patients with DSA (*p < 0.01). The incidence of osteoporosis was statistically higher in patients with DSA (**p < 0.05). The bone mineral density was statistically less in patients with DSA (***p < 0.01). DSA, destructive spondyloarthropathy.
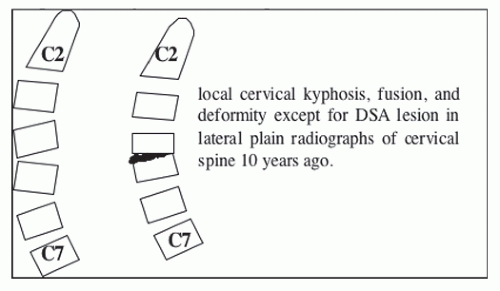
Figure 66.2. Abnormality of focal cervical alignment. Local cervical kyphosis, fusion, and deformity (except for DSA lesion in lateral plain radiographs of cervical spine from 10 years prior).
Cervical alignment is from C2 to C7 is defined as the angle between dorsal margin of the second cervical vertebra and seventh cervical vertebra in lateral plain radiographs of the cervical spine (Fig. 66.1). Cervical alignment, fusion, and deformity are presented, excluding DAS lesions (Fig. 66.2).
FINDINGS
The mean age of the patients with DSA was 52.3 years when hemodialysis was begun, while that of the patients without DSA was 52.7 years. The mean period of hemodialysis was 9.9 years for the patients with DSA and 8.2 years for those without DSA at the end of the study (p < 0.01). Osteoporosis was found in 83 patients (67.5%) with DSA and in 282 (57.2%) patients without DSA (p< 0.05). The mean BMD was 549.9 mg/cm2 for the patients with DSA and 610.4 mg/cm2 for those without DSA (p < 0.01) (Table 66.1). The mean serum β2-microglobulin level was 33.3 mg/L in the patients with DSA and 32.5 mg/L in those without DSA. In the cervical spine, the DSA lesions were predominantly detected in the C5/C6 intervertebral space (80 patients, 65%). In the lumbar spine, the lesions were mostly detected in the L4/L5 intervertebral space (12 patients, 9.8%) (Table 66.2).
TABLE 66.2 Localization of DSA Lesion
Cervical Spine
Lumbar Spine
C2/C3
3 (2.4%)
L1/L2
6 (4.9%)
C3/C4
11 (8.9%)
L2/L3
5 (4.1%)
C4/C5
26(21.1%)
L3/L4
4 (3.3%)
C5/C6
80 (65.0%)
L4/L5
12 (9.8%)
C6/C7
46 (37.4%)
L5/S1
1 (0.8%)
Amyloidosis, except for the spine, was detected in 20 patients (16.3%) with DSA and 65 patients (13.2%) without DSA (Table 66.3). Diseases that induced hemodialysis were detected in 75 patients with DSA and 278 patients without DSA. These included chronic glomerulonephritis (CGN), diabetes mellitus (DM) nephritic syndrome, polycystic kidney, systemic lupus erythematosus (SLE), and so on (Table 66.4). According to the duration of hemodialysis, the incidence of DSA was as follows: group 1—30 patients (10.2%); group 2—38 patients (25.9%); group 3—21 patients (23.9%); and group 4—34 patients (38.6%) (Table 66.1, 66.2, 66.3, 66.4, 66.5).
Only gold members can continue reading. Log In or Register to continue