Chapter 33 Occipitocervical Region
Surgical Anatomy
Dorsal Surgical Anatomy of the Occipitocervical Region
Dorsal approaches to the OC area are most commonly used for OC fusions. During the approach, dissection through several muscular layers is required. The trapezius muscle constitutes the first superficial layer. The trapezius arises from the external occipital protuberans, the ligamentum nuchae, and the spines of the seventh cervical and all thoracic vertebrae.1 The upper fibers insert into the lateral third of the clavicle and form the curve of the shoulder. The middle fibers insert into the medial edge of the acromion and the superior margin of the spine of the scapula, and the lower fibers ascend also onto the scapular spine (Fig. 33-1). The nerve supply of the trapezius muscle is the accessory nerve.
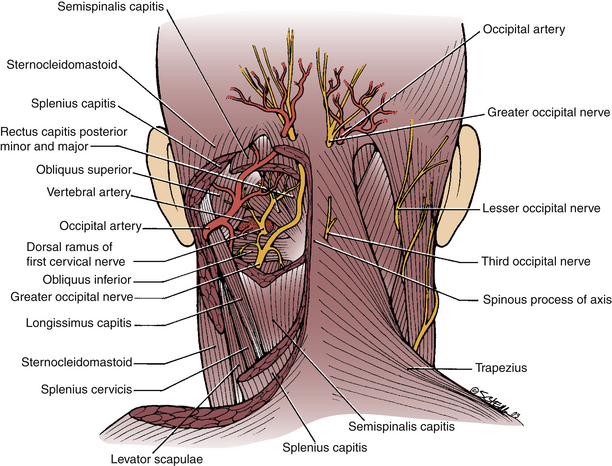
FIGURE 33-1 Dorsal surgical anatomy of the occipitocervical region. Superficial (right) and deep (left).
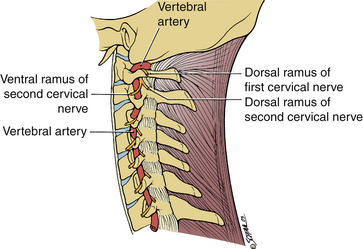
The main vessels in the dorsal OC area are the occipital artery and the vertebral artery. The occipital artery arises from the external carotid artery in the front of the neck and runs dorsally and rostrally deep to the mastoid process and then courses dorsally immediately deep to the muscles attached to the superior nuchal line. It then pierces the trapezius muscle 2.5 cm from the midline to ramify on the back of the head (see Fig. 33-1). As for the vertebral artery, only the third part of this artery is significant during the approach. It emerges from the foramen and the transverse process of the atlas and hooks dorsomedially around the dorsal surface of the lateral mass of the atlas (see Fig. 33-1). It is partly separated from the arch of the atlas by the first cervical nerve (Fig. 33-2; see also Fig. 33-1). It then passes ventromedially in front of the thickened lateral edge of the dorsal atlanto-occipital membrane, which forms an arch over the artery. Occasionally, this arch may be ossified and is referred to as the ponticulus posticus.2 This condition must be recognized preoperatively because failure to do so can lead to catastrophic results if the lateral mass C1 screws are placed through the vertebral arteries. The artery then pierces the dura mater and enters the vertebral canal. The suboccipital plexus of veins is a network of veins that drains into the deep cervical vein and into the vertebral venous plexus around the vertebral artery. The greater occipital nerve is the medial branch of the dorsal ramus of the second cervical nerve, which is the thickest cutaneous nerve in the body. It appears at the middle of the lower border of the inferior oblique muscle and curves superior medially across the suboccipital triangle. It runs rostrally on that muscle and then pierces the trapezius muscle about 2 cm lateral to the occipital protuberans (see Fig. 33-1).
Ventral Anatomy of the Occipitocervical Junction
Three muscles originate from the ventral aspect of the atlas: longus colli, rectus capitis anterior, and rectus capitis lateralis (Fig. 33-3).
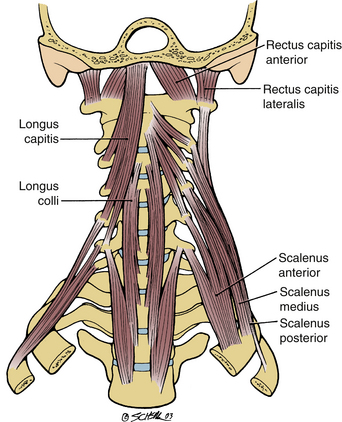
1. The longus colli muscle is the longest and most medial of the muscles. It extends from the anterior tubercle of the atlas to the lower part of the body of the upper thoracic vertebrae. Between these points it is attached to all the vertebral bodies and into the third to sixth cervical transverse processes.
2. The rectus capitis anterior is a short, wide muscle that originates from the ventral surface of the lateral mass of the atlas and is inserted into the base of the skull ventral to the occipital condyle.
3. The rectus capitis lateralis is a short muscle that runs vertically between the rostral surface of the transverse process of the atlas and jugular process of the occipital bone. It lies dorsal to the jugular foramen and is separated from the rectus capitis anterior by the ventral ramus of the first cervical nerve, which supplies both muscles. The function of these muscles is to stabilize the skull on the vertebral column (see Fig. 33-3).
Vertebral Artery
The anatomy of the vertebral artery must be understood because injury to this artery may have dire consequences. The artery starts as a branch of the subclavian artery and passes to the transverse process of the sixth cervical vertebra.1 The artery then ascends vertically through the foramina transversaria accompanied by the vertebral veins and plexus of sympathetic nerve fibers derived from the cervicothoracic ganglion of the sympathetic trunk. Between the transverse processes, it lies medial to the intertransverse muscles and ventral to the ventral rami of the cervical nerves. Upon entering the axis it turns laterally under the superior articular facet in the foramen transversarium and enters the foramen transversarium of the atlas, which is placed farther laterally than the others. Therefore at this level, the artery takes a lateral course (see Fig. 33-2). The artery then emerges on the rostral surface of the atlas between the rectus capitis lateralis muscle and the superior articular process of the atlas. Here it lies with the ventral ramus of the first cervical nerve and curves with it horizontally around the lateral and dorsal aspect of the superior articularis process. It then traverses the articular process and the dorsal arch of the atlas, where it lies rostrally to the dorsal ramus of the first cervical nerve. The artery then turns rostrally and pierces the dura and arachnoid mater. It enters the cranial cavity through the foramen magnum. It then runs ventrally and rostrally over the ventral surface of the medulla oblongata to meet and join the opposite vertebral artery at the inferior border of the pons to form the basilar artery. Through the branches of these vessels, blood is supplied to the hindbrain, midbrain, and dorsal aspect of the cerebrum and the rostral aspect of the spinal medulla. The vertebral vein originates from a plexus of veins that is formed by the union of veins from the internal venous plexus and suboccipital triangle. It accompanies the vertebral artery through the foramina transversaria and exits the sixth cervical transverse process. It passes ventral to the subclavian artery and ends by entering the dorsal surface of the brachiocephalic vein near its origin.
Atlanto-Occipital Joint
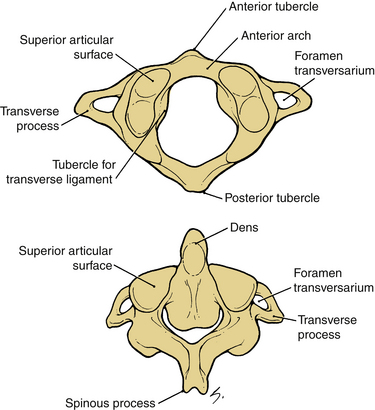
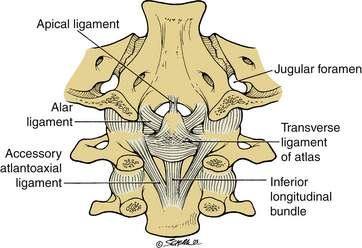
The atlas is a ring of bone with a lateral mass on each side (Fig. 33-4, top).1 The lateral masses are articulated rostrally with the occipital condyles and caudally with the superior articular facets of the axis. Each has a transverse process projecting laterally from it. The atlas is attached to the occiput by strong ligaments, which hold these bones together. However, the articular surfaces, which the atlas has with the skull and axis, are of two different configurations. The kidney-shaped occipital condyles lie on the ventrolateral aspect of the foramen. They fit into the superior articular facets of the atlas, which are also kidney shaped (see Fig. 33-4). The joint allows flexion and extension and slight side-to-side rocking of head motion, but no rotation. The stability of these joints depends on the aid of ligaments, the tectorial membrane, and the longitudinal bands of the cruciate ligament, which all bind the skull to the axis. The ligaments of the joints of the atlas include the anterior longitudinal ligament, which tapers rostrally to be attached to the tubercle of the axis and continues as a narrow band to the base of the skull. The dorsal atlanto-occipital membrane is a rostral continuation of the ligamentum flavum. This membrane passes from the dorsal arch of the atlas to the margin of the foramen magnum dorsal to the atlanto-occipital joint. The lateral margins of the membrane arch over the corresponding vertebral artery and the first cervical nerve. In some cases, these margins may be ossified. The tectorial membrane is a broad ligamentous sheet, which is the rostral continuation of the posterior longitudinal ligament. It passes from the dorsal surface of the body of the axis to the cranial surface of the occipital bone, and it holds the axis to the skull and covers the dorsal surfaces of the dens with its ligaments and the ventral margin of the foramen magnum. The cruciate ligament is formed by rostral and ventral longitudinal bands, which pass from the transverse ligament to the cranial surface of the occipital bone and the body of the axis, respectively. The apical ligament of the dens is a cordlike ligament, which stretches from the apex of the dens to the cranial surface of the occipital bone, immediately above the foramen magnum. The alar ligaments are strong ligaments that arise from the sloping sides of the dens (Fig. 33-5). They pass laterally and upward to the medial sides of the occipital condyle and tighten when the atlas, carrying the skull, rotates around the dens. They are the main factor in limiting rotation of the atlantoaxial joint. The first and second cervical spinal nerves pass dorsally to the OC and C1-2 joint capsules, respectively, and not ventral to the articular facets, as is the case with the remaining subaxial cervical vertebrae.
Related posts:
 Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


