♦ Preoperative
Special Equipment
- Spinal drain
- 1-mm or 2-mm diamond burr drill for drilling of the clinoid; 5-mm burr for removing lateral wing of sphenoid bone
- Irrigating suction
- Cervical carotid exposure instruments
- Radiolucent Mayfield head holder for intraoperative angiography
- 18-gauge angiocatheter, extension set, three-way stopcock, and 7 French suction tube for retrograde suction decompression technique if necessary
Operating Room Set-up
- Groins prepped for femoral access for intraoperative angiography
- Neck exposed and prepped for cervical carotid exposure
♦ Intraoperative
Positioning
- The patient is initially positioned laterally for placement of the spinal drain
- After placement of the spinal drain, the patient is positioned supine with head fixed in radiolucent Mayfield head holder
- Neck is slightly extended (10 degrees) and elevated to promote venous drainage
- Head is rotated 45 degrees away from the approach; exact angle dependent on the direction/location of aneurysms
- Groins prepped for femoral access for intraoperative angiography
- Neck exposed and prepped for cervical carotid exposure
Pterional Craniotomy (see Chapter 5, Pterional Approach)
- Control of the cervical internal carotid artery (ICA)
- Same but smaller exposure as for carotid endarterectomy
- Can be performed by assistant simultaneously while surgeon performs pterional craniotomy
- Rubber vessel loops are placed around the common carotid artery (CCA), the ICA, and external carotid artery (ECA)
- Large temporary aneurysm clips and a Fogarty vessel clamp are selected ahead of time for possible occlusion of the ICA, ECA, and CCA if needed at the time of aneurysm exposure and clipping
- Same but smaller exposure as for carotid endarterectomy
Dolenc Approach (see Chapter 7, Dolenc Approach)
- We prefer the Dolenc approach of combined extradural and intradural clinoid removal
- We perform both the extradural and intradural clinoid drilling under the microscope
- The irrigating suction facilitates irrigation cooling during drilling under the microscope
Exposure and Clipping of the Aneurysm
- We use spinal drainage for clipping of ophthalmic artery aneurysms; adequate brain relaxation is critical. Allow for slow drainage into cerebrospinal fluid (CSF) collecting system as opposed to syringe withdrawal of CSF.
- Important to identify the origin and course of the ophthalmic artery
- Important to visualize the proximal neck of the aneurysm which may be difficult to expose if buried deep in skull base or is partially extradural
- Be careful not to injure the optic nerve which lies intimately to the aneurysm and parent vessel (Fig. 23.1), often “on stretch” from mass effect from the aneurysm; critical to open dural band over the optic nerve sharply once bone is removed (allows for clip insertion under optic nerve)
- Temporary occlusion may be necessary in dissection and exposure of the full aneurysm neck, in which case, proximal occlusion is achieved by occlusion of the cervical ICA, ECA, and CCA, and distal occlusion is performed with a temporary clip placed on the ICA between the posterior communicating artery and the aneurysm
- Superior projecting aneurysms: a straight clip is preferred with clip blades along the axis of the ICA
- Medial projecting aneurysms: we prefer the J-curved clip which reconstructs the natural curvature of the ICA
- Inferior projecting aneurysm: we prefer fenestrated clips placed such that the ICA courses through the fenestration and the clip blades are on the undersurface of the ICA along the axis of the ICA. We have liked this clip configuration because full view of the aneurysm for this type of aneurysm is not always possible, and this clip allows for “blind” clip reconstruction of the artery.
< div class='tao-gold-member'>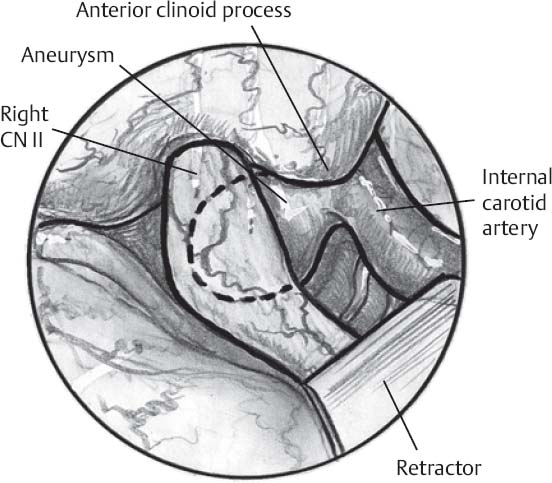 Only gold members can continue reading. Log In or Register to continue
Only gold members can continue reading. Log In or Register to continue








