♦ Preoperative
Operative Planning
- Assess extent of lesion on imaging studies; assess size and location of frontal sinus
- Allow optimal exposure and alternative trajectories to the anterior, middle, and posterior fossae (not appropriate for extensive lesions of the posterior fossa)
Equipment
- Craniotomy tray
- Mayfield head holder
- High-speed drill
- Microscope
- Neurophysiologic monitoring for aneurysm cases
Anesthetic Issues
- Arterial and central venous lines
- Intravenous antibiotics and steroids
- Mannitol (0.5 to 1.0 g/kg) for large tumors
- Anticonvulsants
♦ Intraoperative
Positioning
- Head fixation using the Mayfield head holder with double pins low at ipsilateral retromastoid region and single pin in sagittal plane of contralateral midpupillary line just behind the hairline
- The head is turned 30 to 60 degrees to the contralateral side with the malar eminence at the highest point of the surgical field
- Place an ipsilateral shoulder roll to ensure good jugular venous return
- The skin incision is marked: the preauricular end starts at the inferior border of the zygoma 1 cm anterior to the tragus and curves medially to end, just lateral to the midline on the contralateral side
Phase I: Frontosphenotemporal (Pterional) Craniotomy (Fig. 6.1A)
- Scalp flap is reflected anteriorly
- Superficial layer of the temporalis fascia is incised and reflected anteriorly with fat pad to preserve the frontalis branch of the facial nerve
- Blunt subperiosteal dissection of the superior and lateral aspects of the orbit to expose the orbital roof and lateral wall, respectively, and zygoma inferiorly until visualization of the inferior orbital fissure (IOF), with careful identification and preservation of the supraorbital nerve
- The periorbita is carefully dissected away from the superior orbital rim down to the level of the malar eminence. The supraorbital nerve is easily reflected with the periorbita if a supraorbital notch is present. A small chisel or narrow side cutting burr may be used to release the nerve if a true foramen is present.
- Temporalis muscle is incised to leave a myofascial cuff along the superior temporal line. The muscle is separated with blunt dissection, and bleeding controlled with bipolar cautery to preserve blood supply from the deep temporal artery and prevent temporalis muscle atrophy.
- The masseter muscle is dissected away from the inferior border of the zygomatic arch
- The number of burr holes is contingent on surgeon preference. Usually, a burr hole is placed in the temporal squamosa above the temporal root of the zygoma. A second burr hole is placed at the keyhole that is located over the frontosphenoidal suture ~1 cm behind the frontozygomatic suture line.
- The craniotome is used to perform the frontosphenotemporal craniotomy
Phase II: Orbitozygomatic Osteotomy (Fig. 6.1B)
- Make an oblique cut with a narrow side cutting burr at the root of the zygomatic process
- The second cut is made starting at the posterolateral edge of the body of the zygoma and ending halfway toward the orbit.
- For the third cut, start in the IOF intraorbitally, and then extend the cut in an oblique fashion to meet the second cut. Stay above the zygomaticofacial fissure to avoid the maxillary sinus, and ensure protection of the periorbita. Oblique cuts are made for cosmetically appealing reapproximation.
- The orbital roof and lateral wall of the orbit are exposed by elevating the frontal dura over the sphenoid ridge and the dura off the anterior temporal fossa.
- The fourth cut is made through the superior orbital rim just lateral to the supraorbital notch, extending through the orbital roof toward the superior orbital fissure
- The fifth cut is made by starting in the IOF extraorbitally and extending the cut through the lateral wall to meet the fourth cut in the orbital roof
- The orbitozygomatic flap (Fig. 6.1C) can be elevated to remove the orbital roof. Place miniplates along the flap prior to elevation to ensure a good cosmetic closure.
< div class='tao-gold-member'>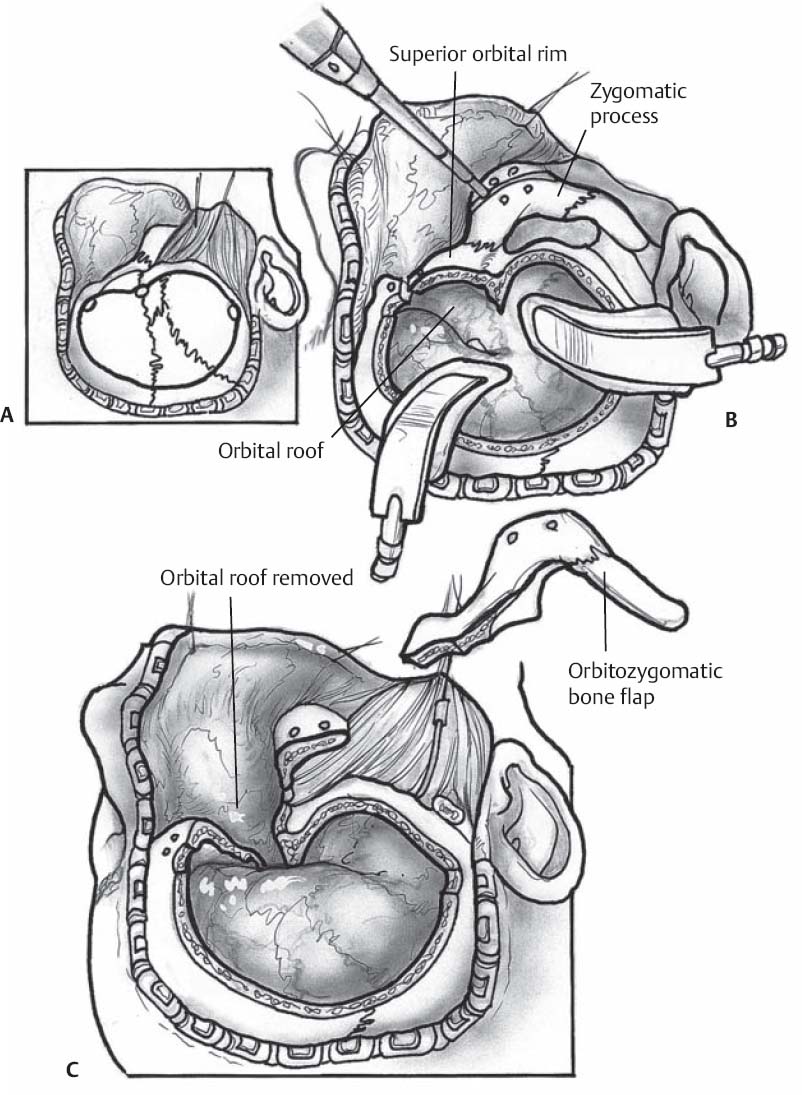
Fig. 6.1 Burr holes are placed in the temporal squamosa above the temporal root of the zygoma and the keyhole that is located over the frontosphenoidal suture ~1 cm behind the frontozygomatic suture line for the pterional craniotomy (A). Five cuts (B) are made in the zygomatic process, superior orbital rim, and orbital roof to complete the orbitozygomatic osteotomy (C).
Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel






Full access? Get Clinical Tree


