Parkinson’s disease and other akinetic rigid syndromes I
In 1817 James Parkinson wrote ‘Essay on the shaking palsy’. The clinical syndrome he described, with tremor, rigidity and slowness of movement, is referred to as Parkinsonism or an akinetic rigid syndrome. The most frequent pathological cause of this syndrome is Parkinson’s disease.
Clinical features
The classical features of Parkinson’s disease are TRAP:




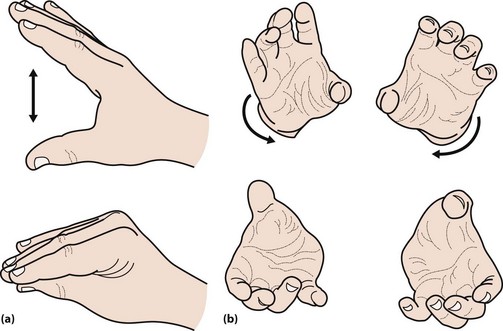
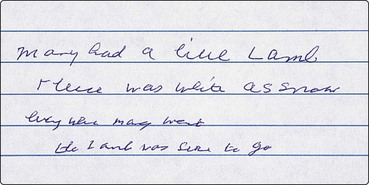
The face is immobile and the skin may appear greasy. There may be a dysarthria, with a monotonous voice that tends to trail off. Fast repeated movements tend to slow up, so-called bradykinesia. This can be tested by asking the patient to drum their fingers on a table or repeatedly bringing index finger and thumb together (Fig. 1). Writing becomes small and spidery (Fig. 2). The posture tends to become stooped and the patient stands with slightly flexed elbows (Fig. 3). On walking there is a loss of arm swing, the steps become shorter and there may be difficulty starting or stopping. The patient may be unsteady or fall on turning. This reflects the loss of postural reflexes; these can be tested by standing behind the patient and gently pulling the patient backwards. This would normally lead to a minor adjustment in posture, but a patient with altered postural reflexes may take multiple steps backwards. In more severe disease, there may be freezing – where the patient cannot start to walk – a form of akinesia. The gait may be festinant, where the patient cannot stop once started.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


