Pediatric Neuroangiography: Technical Aspects
Key Points
Adults are big children, but children are not small adults.
With modification of basic techniques, the risks of endovascular procedures in children should not be any greater than that in adults, and probably less in most instances.
Neuroangiographic procedures in children are not necessarily more difficult in some ways than in adults, but the prospect of causing a complication or injury to a little one raises the operator’s anxiety. In many ways, a diagnostic or interventional endovascular procedure is similar, in miniaturized form, to that of an adult. The craniocervical vessels are almost always straighter in children, which makes vessel catheterization much easier in fact. However, the differences between pediatric and adult procedures are in other ways substantial and must be considered.
Arteriotomy and Sheath
Quite apart from the issue of size of sheath that a pediatric femoral artery will take, the delicacy of the tissue must be taken into account (Figs. 4-1 and 4-2). A rough or forceful technique in the groin could end in a disastrous tearing or transection of the vessel. Gentle sequential dilation of the vessel to stretch the arteriotomy site is safer. Once access to the vessel is obtained, a small injection of intra-arterial calcium blocker, for example, verapamil (0.01 mg/kg), might be considered to alleviate spasm. Intra-arterial heparin and/or systemic heparinization (30–60 U/kg) are highly advised to prevent vessel thrombosis or occlusion during or following the procedure.
Groin Compression
Pediatric arteries are easy to compress, certainly compared with many expansive groins that the beginning fellow has to confront. Too easy, in fact. The difficulty is that one does not necessarily want to actually compress the artery completely to the point of sustained occlusion after the first minute or two, following removal of the sheath. The priority is to encourage the re-establishment of antegrade flow in the artery as soon as possible. Therefore, a very light compression with the left hand only is usually sufficient, while the right hand palpates the distal pedal pulse or checks with a Doppler device (Fig. 4-3). A reassuring thrill under the left hand throughout the groin compression procedure is optimal, in contrast to the forceful ordeal of the adult groin.
Radiation Protocol
The long-term consequences of the current patterns of medical x-ray use are unknown and discussed at length in Chapter 6. In all likelihood children are more sensitive to the deterministic and stochastic effects of even modest doses of radiation, and every effort should be made to reduce the dose inherent in neurovascular procedures. Furthermore, because of their small body size, an adult radiation protocol is completely unnecessary and probably counterproductive. Several pediatric specific precautions, including use of a pediatric radiation protocol, should be incorporated into the “Time-Out” checklist at the beginning of each procedure. Attention should be paid to minimizing the source image distance (SID) and consideration should also be given to removing the grid (a huge payoff—>40% reduction in radiation dose—for a small price in image quality). The greatest savings in radiation reduction are always to be had through minimization of the DSA cumulative image count. Modulation of the “frame rate per second” during the DSA run can reduce exposure by a factor of a third to a half. With reference to fluoroscopy, the biggest savings are to be made through modulation of dose per pulse, modulation of pulse rate per second, and particularly by maximal use of copper filtration options. These are all subject to manipulation in the password-protected software of the machine, but will require sitting down with the vendor engineer to change them. Vendors have an incentive to present you with images that are aesthetically pleasing and competitive. From a radiation-savings point of view, images should not be optimized; they should be adequate for the purpose in hand (1).
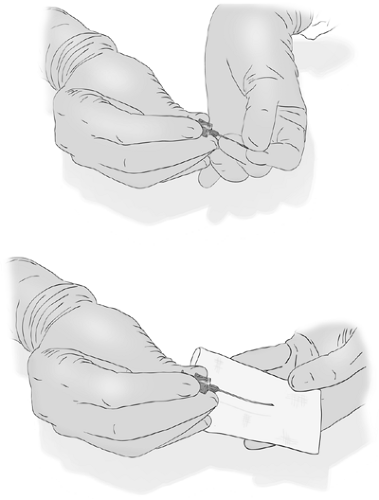 Figure 4-1. Pediatric needle technique. Safe access into and out of the pediatric common femoral artery is frequently the major challenge of pediatric neuroangiography, particularly for smaller children. Ultrasound guidance probably has much to recommend it, particularly when the artery is too small to palpate. Spasm, even under general anesthesia, is a big challenge, meaning that any kind of false or failed puncture will leave the operator standing there for exactly 20 minutes before the pulse normalizes and a repeat attempt can be made. A very steady hold on the needle while an assistant gently passes the wire is the best protection against losing an opportunity. A shorter 5-cm pediatric size needle is easier to hold steadily, and access of the wire to the lumen seems to be much facilitated by putting a slight bend in the distal needle by folding the needle in a piece of gauze (omitted from the diagram for illustration purposes) and bending very slightly with the left thumb.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
