Pineal Region Mass, General
Gregory L. Katzman, MD, MBA
DIFFERENTIAL DIAGNOSIS
Common
Pineal Cyst
Less Common
Cavum Velum Interpositum (CVI)
Meningioma
Pineocytoma
Arachnoid Cyst
Tectal Plate Glioma
Neurocysticercosis
Lipoma
Intracranial Hypotension
Medial Atrial Diverticulae (Obstructive Hydrocephalus)
Rare but Important
Germinoma
Epidermoid Cyst
Dermoid Cyst
Vein of Galen Malformation
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Quadrigeminal cistern (QC)
Bounded by quadrigeminal plate, splenium, vermis, & tentorial margin
Extends between layers of 3rd ventricle tela choroidea
Contents: Caudal internal cerebral veins → vein of Galen, distal parts of quadrigeminal artery, PCA P4 segment, & CN9 exit
Synonyms: Cisterna quadrigeminalis, cistern of great cerebral vein, cisterna venae magnae cerebri, Bichat canal, cisternal quadrigeminalis, & superior cistern
Helpful Clues for Common Diagnoses
Pineal Cyst
Homogeneous fluid-filled mass above & clearly distinct from tectum
55-60% slightly T1 hyperintense to CSF; FLAIR doesn’t suppress; 60% enhance (partial/complete rim, nodular)
Cystic expansion of pineal in some females begins in adolescence, decreases with age
Can’t distinguish from pineocytoma on basis of imaging studies alone
Helpful Clues for Less Common Diagnoses
Cavum Velum Interpositum (CVI)
Axial MR/CT shows triangular-shaped CSF space between bodies of lateral ventricles
FLAIR suppresses completely; no enhancement
Dilatation of velum interpositum, precise etiology unknown
Common in early infancy, rare in adults
Meningioma
Avidly enhancing mass, trapped pools of CSF common, focal calcification may represent displaced pineal
Arise from posterior portion of the velum interpositum, falx, or tentorium
Velum interpositum meningiomas: M = F, in both pediatric & adult populations
May be symptomatic from compression of quadrigeminal plate
Pineocytoma
Enhancing, circumscribed pineal mass which “explodes” pineal Ca++
May mimic pineal cyst or pineoblastoma
May compress but does not invade adjacent structures
˜ 45% of pineal parenchymal tumors
Arachnoid Cyst
Sharply demarcated extra-axial cyst that follows CSF attenuation/signal
Quadrigeminal arachnoid cysts (AC) are 3rd most common infratentorial AC
Symptoms depend on compression of brain stem, cerebellum, & aqueduct
Elevated ICP & sudden death have been reported
Tectal Plate Glioma
Tectal distortion or thickening by localized mass
T1 hypointense, T2 hyperintense, ± enhancement
Onset aqueductal stenosis often without associated brain stem signs
Reported as indolent lesions often remaining stable in size for many years
Neurocysticercosis
May involve cisterns > parenchyma > ventricles
Basal cistern cysts may be racemose
Cysts variable, typically 1 cm, range from 5-20 mm and contain a 1-4 mm scolex
Cystic lesion isointense to CSF, may see discrete, eccentric scolex
Lipoma
Well-delineated lobulated extra-axial mass with fat attenuation/intensity
40-50% interhemispheric fissure (over corpus callosum)
Ca++ varies from none to extensive
Fat-suppressed MR is diagnostic
Intracranial Hypotension
Corpus callosal descent can efface QC
Sagittal shows brain descent in 40-50%
Diffusely, intensely enhancing dura in 85%
Bilateral subdural fluid collections in 15%
Medial Atrial Diverticulae (Obstructive Hydrocephalus)
Mechanism
Massive ventricular dilatation causes stretching & dehiscence of fornix → unilateral or bilateral diverticula of inferior medial atrial wall
Enlargement of pial pouch creates subarachnoid cyst that may herniate through incisura into QC
Imaging
Focal dehiscence of medial atrial wall
Draping of medial atrial wall over free margin of tentorium with continuity of CSF around tentorial edge
Contralateral internal cerebral vein displaced
Presence of septa separating diverticulum from 3rd ventricle
Helpful Clues for Rare Diagnoses
Germinoma
Pineal region mass that “engulfs” the pineal gland
T1/T2 iso- or hyperintense to gray matter
Strong uniform enhancement, ± CSF seeding
Epidermoid Cyst
Lobulated, irregular, CSF-like mass with “fronds” insinuates cistern
FLAIR usually doesn’t completely null; diffusion yields high signal restriction
0.2-1.8% of all primary intracranial tumors
Congenital inclusion cysts; rare malignant degeneration into squamous cell CA
Dermoid Cyst
Fat appearance: Use fat suppression sequence to confirm
Rupture → fat droplets in subarachnoid spaces with extensive enhancement possible from chemical meningitis
< 0.5% of primary intracranial tumors
Rare malignant degeneration into squamous cell carcinoma
Vein of Galen Malformation
Dilated arteries feeding into large midline venous pouch
Thin sagittal images define anatomy & relationship to cerebral aqueduct
< 1% cerebral vascular malformations at any age
Neonatal > infant presentation most common; rare adult presentation
Image Gallery
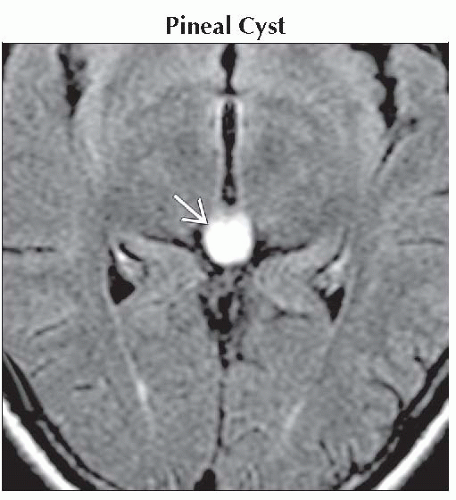 Axial FLAIR MR shows the classic finding of a presumed pineal cyst  that does not suppress and is moderately hyperintense. that does not suppress and is moderately hyperintense. |
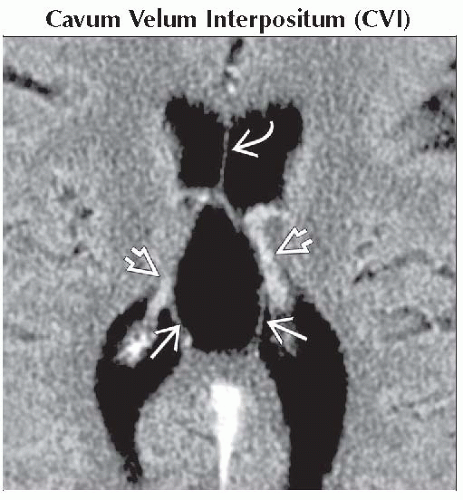 Axial CECT shows a CSF collection between the fornices
 , splaying the internal cerebral veins & choroid plexus inferolaterally , splaying the internal cerebral veins & choroid plexus inferolaterally  . Note the septum pellucidum . Note the septum pellucidum  is intact. is intact.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
