♦ Preoperative
Operative Planning
- Imaging
- Magnetic resonance imaging (MRI)
- Computed tomography myelogram if MRI is inconclusive
- Flexion/extension x-rays
- Magnetic resonance imaging (MRI)
- Patient counseling regarding surgical risks
- Postoperative pain
- Potential joint instability
- Postoperative pain
Equipment
- Basic spine tray
- High-speed drill (Midas Rex with AM-8 bit)
- One- and 2-mm Kerrison punches
Operating Room Set-up
- Headlight
- Loupes
- Microscope
- Bipolar cautery and Bovie cautery
- Intraoperative x-ray
- Intraoperative fluoroscopy
- Mayfield head holder
Anesthetic Issues
- Consider awake fiberoptic intubation to avoid passive neck extension
- Assess patient’s pulmonary function for ability to tolerate prone position
- Prophylactic intravenous antibiotics (cefazolin 2 g for adults) 30 minutes prior to incision
- Foley catheter for prolonged surgery
♦ Intraoperative (Fig. 100.1)
Positioning
- Prone position with appropriate padding to prevent pressure neuropathies
- Arms tucked at sides
- Mayfield head holder or tongs with traction to secure head in capital flexion
- Mild reverse Trendelenburg position for venous drainage
- Intraoperative fluoroscopic imaging used to confirm cervical alignment
Planning of Minimal Shave
- Use disposable razor
Planning of Sterile Scrub and Preparation
- Betadine detergent scrub with sterile gloves for 5 minutes
- Alcohol to remove Betadine scrub
- Sterile towel to dry
- Incision is marked
Mark Incision
- Localization using C2 and C7 landmarks
- Intraoperative x-ray
- Mark the midline incision
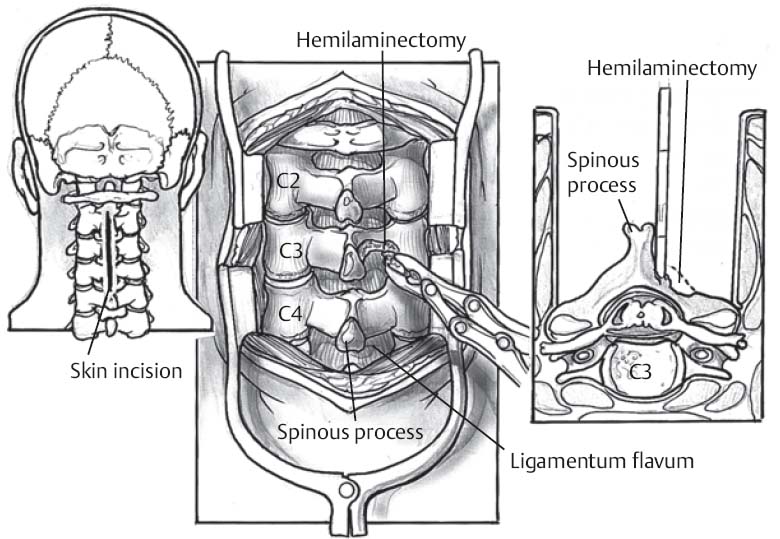
Fig 100.1 Schematic of the posterior cervical approach.
Only gold members can continue reading. Log In or Register to continue
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


