♦ Preoperative
Operative Planning
- Review imaging (sagittal magnetic resonance imaging is the study of choice)
- Assess level of descent of posterior fossa structures; this determines the level of spinal exposure that will be necessary
- Note level of transverse sinus, which will be low in Chiari II
Special Equipment
- Dural substitute if performing dural opening procedure (the authors use bovine pericardium in children, but pericranium, autologous fascia, cadaveric dura, Gore-Tex [W. L. Gore & Associates, Inc., Elkton, MD], etc., are acceptable)
- Ultrasound for nondural opening technique
Operating Room Set-up
- Mayo stand at head of bed
- Prone table with bolsters
- Room should be warm to ensure normothermia (heat lamps for infants)
- Intravenous antibiotics with skin flora coverage (cefazolin 2 g for adults, 30 mg/kg in pediatrics) should be given 30 minutes prior to incision
- Single preoperative dose of dexamethasone
Intraoperative Neurophysiologic Monitoring
- Somatosensory evoked potential (SSEP) and brain stem auditory evoked response (BAER) monitoring (institutional evidence to support its use)
- Obtain baseline prior to positioning
- Repeat potentials after positioning to ensure that the neck is not excessively flexed
- Continuous monitoring during case
♦ Intraoperative
Positioning (Fig. 160.1A)
- Patient prone
- Head supported in neutral position on padded horseshoe in children up to age 2 to 3 years, and in either padded horseshoe or three-pin Mayfield fixation in older children and adults
- Neck flexed until two fingers can just fit between chin and upper sternum
- Eyes are checked to prevent compression by horseshoe
- All pressure points are padded (adhesive foam rubber may be placed on bony prominences prior to turning; this is particularly important in thin children)
Planning of Minimal Shave
- Use disposable razor
- Occipital protuberance to hairline in midline
Drape
- 3M drapes placed along sides of neck to prevent prep solutions from threatening the security of the endotracheal/nasotracheal tube in young children with uncuffed tubes or causing corneal damage
- Four towels and Steri-Drape
- Split or fenestrated sheet
Planning of Sterile Scrub
- Betadine detergent scrub and sterile gloves for 5 minutes
- Sterile towel to dry
Mark Incisions (Fig. 160.1B)
- Inion to C2 spinous process
- In patients with short hair, may attempt to keep incision above hairline
< div class='tao-gold-member'>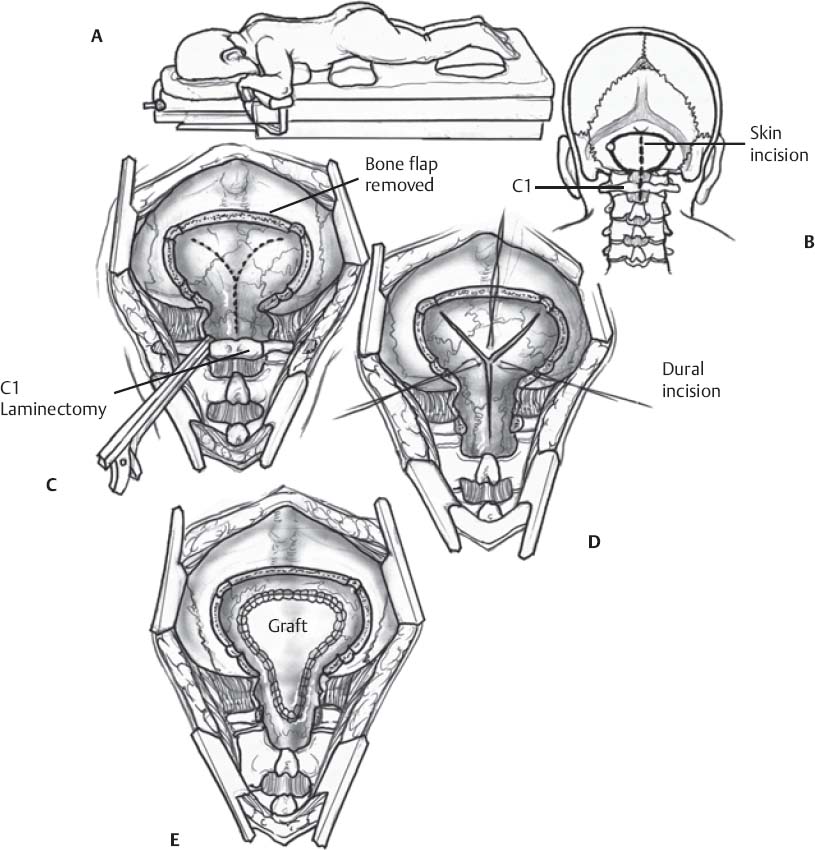
Fig. 160.1 Schematic of posterior fossa decompression for Chiari malformations. (A) Patient postioning. (B) Incision marking. (C) Bony decompression. (D) Dural opening is performed via Y-shaped incision. (E) Closure of the dura.
Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel






Full access? Get Clinical Tree


