22Practice Exam Answers D Optic nerve The anatomy during the transnasal transsphenoidal approach is shown in this image. MC, middle clinoid process; MCS, medial cavernous sinus; LOCR; lateral opticocarotid recess. A Central neurocytoma The MRI scans accompanying the question show a heterogeneous intraventricular mass attached to the septum pellucidum that has solid components and areas of cystic change, with a bubbly or spongiform appearance. Of the given options, the features are most consistent with a central neurocytoma, although ependymomas can sometimes have a similar appearance. Central neurocytomas are WHO grade II neuroepithelial neoplasms that occur most commonly in patients between 20 and 40 years of age. Enhancement is variable and may be minimal, as seen in this case. Patients typically present with headaches, seizures, or symptoms of increased intracranial pressure. (B) Most intraventricular meningiomas are solid appearing and enhance avidly, although they can be heterogeneous and show cystic changes, calcifications, and even hemorrhage. (C) Intraventricular metastases are rare and usually demonstrate moderate to marked contrast enhancement. (D) Choroid plexus papillomas enhance avidly and typically show a frond-like margin with a texture that is similar to that of the normal choroid plexus. (E) Subependymal giant cell astrocytomas are seen almost exclusively in the setting of tuberous sclerosis. They almost always enhance avidly, and most commonly occur in the frontal horns in or around the foramina of Monro. A Neurosecretory vesicles-neurophysin complex Several studies support neurosecretory granules (particularly antidiuretic hormone) as being the cause of the expected T1 shortening (hyperintensity) in the posterior pituitary gland. Specifically, antidiuretic hormone generally is accepted as the source, although oxytocin has been implicated by some sources. Neurosecretory granules form a complex with neurophysins, which are carrier proteins for transportation from the supraoptic and paraventricular nuclei of the hypothalamus. The presence of hyperintensity indicates the functional integrity of the posterior pituitary gland. It can be absent in diabetes insipidus or surgical or traumatic transection of the stalk. It also can be absent in about 10% of the population. (B) Calcification most typically is associated with signal intensity loss on T1; however, at lower concentrations of calcium, T1 shortening effects (hyperintensity) predominate, whereas at higher concentrations there usually is signal loss due to susceptibility effects. This is not the cause of the posterior pituitary bright spot. (C) Ferritin-bound iron has T1 shortening effects and can look bright; however, this is not the source of the posterior pituitary hyperintensity. Hemosiderin-bound iron does not have a significant T1 shortening effect. (D) Manganese has T1 shortening effects such as in the basal ganglia in liver disease, but this is not present in sufficient concentrations in the pituitary gland to result in significant hyperintensity. D Contralateral subthalamic nucleus The basal ganglia are composed of the caudate nucleus, putamen, globus pallidus (GP), subthalamic nucleus (STN), and substantia nigra. These structures connect to other areas of the brain and are involved in numerous functions, including motor control. The STN is located just inferior to the thalamus and makes glutamatergic, excitatory connections to the globus pallidus and the substantia nigra. This is the only purely excitatory pathway among the intrinsic pathways of the basal ganglia. Injury to the subthalamic semilunar nucleus of Luys or its efferent or afferent connections can induce hemiballismus. The STN itself is a regulator of motor function and is involved in associative and limbic functions. It traditionally was thought that hemiballismus was only caused by injury to the STN, but new studies are showing that it can occur with damage to other areas of the brain. Hemiballismus arising from the STN is more severe than other forms of the disorder. Recent studies show that hemiballistic movements also may be associated with a decreased output from the GP. Decreased activity in the GP prevents inhibition of the motor portion of the thalamus, leading to characteristic large, irregular hemiballistic movements. Finally, the caudate nucleus helps control voluntary movement, and damage to this area may result in hemiballismus due to its involvement with voluntary movement. (A, B) The putamen projects to the premotor cortex through the globus pallidus. Damage to the putamen also can cause hemiballistic movements. D Ventral intermediate nucleus of the thalamus Stimulation of the ventral intermediate nucleus of the thalamus offers the best control of essential tremors and “tremor dominant” Parkinson disease. (A) The globus pallidus pars externa is not a standard target for deep brain stimulation. (B, E) Stimulation of both the subthalamic nucleus and globus pallidus pars interna produces similar symptom relief with regard to the motor symptoms of parkinsonism (e.g., bradykinesia, tremor, and rigidity). Stimulation of the globus pallidus interna is effective especially at relieving symptoms of dystonia. (C) Stimulation of the head of the caudate nucleus is used for symptom relief in obsessive-compulsive disorder. C Cytokeratin AE1/AE3 The meninges shown in the image accompanying the question are marked by increased cellularity. Many of the cells appear to have eccentric nuclei and cytoplasm, with more cytoplasm present than is usually seen with lymphoid cells. The pathology is that of leptomeningeal carcinomatosis. Keratin antibody stains such as cytokeratin AE1/AE3 best highlight these cells. D Thalamostriate vein, as shown in this image. E It may be associated with SDHx gene mutations. The images accompanying the question show an avidly enhancing mass in the left jugular foramen that is compatible with a glomus jugulare, given its high uptake on the 111In-DTPA-pentetreotide scan. These lesions are highly vascular masses that may show a “salt-and-pepper” appearance on noncontrast T1 images due to areas of hemorrhage and small vascular flow voids, respectively. About one third of paragangliomas may be part of a germline mutation particularly related to the succinate dehydrogenase gene group. Other associations include von Hippel-Lindau and multiple endocrine neoplasia type 2 syndromes. (A) Only 3% of paragangliomas are multicentric except for familial lesions, which may be multiple in 25% of patients. (B) It is believed that vestibular schwannomas arise at the glial–Schwann cell (Obersteiner-Redlich) transition zone. (C) Sporadic paragangliomas are much more common in females. Hereditary paragangliomas have a more or less equal distribution across the genders. (D) The majority of paragangliomas are benign, with malignant tumors being rare. D Vestibular schwannoma Chemotherapy has shown some promise in treating neurofibromatosis type 2-related vestibular schwannomas with demonstrated progressive growth. (A–C) Most meningiomas, epidermoids, and choroid plexus papillomas are WHO grade I lesions and are not treated with chemotherapy. (E) Ependymomas do not respond well to chemotherapy, although there are some newer protocols that show some promise. In addition, chemotherapy may be used in children under 3 years of age in an attempt to delay radiotherapy. C Systems-based practice Systems-based practice describes multidisciplinary approaches to patient care and the ability to optimize care by involving multiple teams in patient management. (A) Medical knowledge describes the ability to acquire and apply current medical knowledge and use advanced search engines to stay current on medical knowledge and data. (B) Professionalism describes the ability to demonstrate the principles of ethical behavior. (D) Practice-based learning and improvement describes the ability to appraise information critically on a daily basis and to analyze it in a way that improves patient care. (E) Interpersonal skills and communication skills refer to a resident’s ability to communicate effectively among colleagues in his and in other specialties. It also refers to the ability of a resident to share his research and demonstrate leadership skills. B B The American Spinal Injury Association (ASIA) impairment scale indicates the completeness of a spinal cord injury. An A classification represents a “complete” injury, whereas classifications B through D represent “incomplete” injuries. With a B classification, there is preservation of sensation in the S4 and S5 dermatomes but no motor function below the level of injury. A C classification indicates that more than half of the muscles below the level of injury have a motor grade less than 3. Classification D indicates that more than half of the muscles below the level of injury have a motor grade of at least 3. The E classification is reserved for full motor and sensory function and is used to describe patients with spinal cord injuries (i.e., it is not a way to document a normal neurologic exam in a patient without injuries). A Induction agent, paralytic agent, intubation Rapid sequence intubation (RSI) is designed to intubate patients who are at risk of vomiting and thus aspiration. Its use does not require preventilation with a bag valve mask. RSI involves administration of an induction agent (typically etomidate) followed by a paralytic agent (succinylcholine or rocuronium). The goal is to render the patient unconscious and paralyzed within 1 minute. This then is followed by intubation. E No additional nuclei (A–D) The dentate, emboliform, globose, and fastigial nuclei are the deep cerebellar nuclei and can be remembered by the mnemonic “Don’t eat greasy food.” E Number of transmembrane channels specific for the diffusing molecule Facilitated diffusion requires transmembrane channels to allow molecules to diffuse across an otherwise impermeable membrane along a concentration gradient. This process thus is limited by the number of transmembrane channels. (A) A molecule undergoing facilitated diffusion must have a binding site on its transmembrane channel. More binding sites mean that more molecules can diffuse across the membrane. (B) Cell membranes with their phospholipid bilayer are lipophilic and prevent the simple diffusion of certain molecules across the membranes. These hydrophilic molecules are the ones that require the use of transmembrane channels; thus, the actual process of facilitated diffusion avoids the membranes’ limitations and is not affected by cell membrane composition. (C) Large concentration gradients assist with facilitated diffusion. (D) ATP is involved in active transport. Facilitated diffusion requires no direct energy input. C Predictor of mortality Although other uses for the intracranial hemorrhage (ICH) score have been extrapolated, the ICH score was designed to predict mortality. An ICH score of 0 is associated with a 0% 30-day mortality, whereas patients with a score of 5 or 6 have a 100% 30-day mortality. Scores of 1, 2, 3, and 4 are associated with 30-day mortalities of 13%, 26%, 72%, and 97%, respectively. E XII All tongue muscles except the palatoglossus are innervated by the hypoglossal nerve. Fasciculations of the tongue indicate injury to the hypoglossal nerve and denervation of the tongue. Such findings are presumed to occur secondary to acetylcholine hypersensitivity at the denervated neuromuscular junction. Atrophy also occurs when the tongue is denervated. Lesions of the hypoglossal nerve typically are secondary to amyotrophic lateral sclerosis. (A) The lingual branch of the mandibular division of the trigeminal nerve provides sensation to the anterior two thirds of the tongue through special visceral afferent fibers. (B) The chorda tympani of the facial nerve carries taste from the anterior two thirds of the tongue. (C) The glossopharyngeal never carries taste and sensation from the posterior one third of the tongue. (D) The vagus nerve innervates the palatoglossus muscle. A Scheuermann disease Scheuermann disease is defined by the presence of anterior vertebral wedging measuring 5 degrees or greater involving at least three adjacent vertebrae. It usually presents in early adolescence. The etiology is not certain, but there may be a genetic component. (B) Osteopoikilosis is a rare, inherited sclerosing dysplasia characterized by multiple enostoses that may involve the spine. (C) Baastrup disease occurs due to chronic apposition of spinous processes in the lumbar spine, with resultant sclerosis and degenerative change. Back pain tends to improve with flexion and is exacerbated with extension of the spine. (D) Alkaptonuria (also known as ochronosis) can result in widespread calcification of the intervertebral disks. (E) Osteopetrosis is caused by deficient osteoclastic activity and leads to diffuse sclerosis of the bones. In the spine, thick sclerotic bands can be seen paralleling the end plates. D Sweat glands Cocaine would cause an activation of the sympathetic nervous system, whereas atropine administration would block the parasympathetic nervous system. Sweat glands are unique in that they are the only organs with sympathetic but no parasympathetic innervations. Although the kidneys have parasympathetic input, they also rely mainly on the sympathetic nervous system. D 4 to 6% per year The patient likely has an arteriovenous malformation (AVM) that has hemorrhaged. AVMs are thought to have a consistent yearly hemorrhage rate of approximately 4%, which may be slightly higher in patients who have had a previously hemorrhage, deep-seated hemorrhage, or deep-draining veins. AVMs usually do not receive emergent surgical intervention given these re-hemorrhage rates, unless there is significant mass effect reduction expected from resection of the hematoma. Note the classic appearance of the hemorrhage tapering toward the ventricle in the image. (A–C) These figures are consistent with re-hemorrhage rates following aneurysmal subarachnoid hemorrhage. (E) Cavernous hemangiomas have a less than 1% risk of re-hemorrhage over a lifetime, although documented hemorrhage and re-hemorrhage rates are very inconsistent in the literature. A Diffuse idiopathic skeletal hypertrophy Ankylosing spondylitis starts in the sacroiliac joints and progresses rostrally, whereas diffuse idiopathic skeletal hyperostosis (DISH) spares the sacroiliac joints and primarily involves the thoracic spine. Both conditions may predispose to fractures and spinal cord injuries from minor trauma. (D, E) Rheumatoid arthritis and gout can affect the sacroiliac joints as well as numerous other joints throughout the skeleton. B Cat Toxoplasmosis is the most common opportunistic infection found in an individual with HIV/AIDS. Its definitive host is a cat. (A) Cryptococcus is the second most common opportunistic infection found in an individual with HIV/AIDS. Its definitive host is a bird. D Double vision, ocular deviation, and postural imbalance (A) Increased akinesia with reduced rigidity might be seen if the lead was positioned caudal to the target and hit the substantia nigra. (B) Reduced tremor with persistent akinesia might be seen with a lead placed superficially to the target in the zona incerta. (C) Tetany and dysarthria are seen with laterally placed leads in the internal capsule. (E) Perspiration, mydriasis, and dysesthesias are seen with leads placed too far posteriorly in the hypothalamus. A Epidermoid The description of this sequence corresponds to diffusion-weighted imaging (DWI). Epidermoid tumors may be cystic appearing on T1- and T2-weighted sequences (sometimes appearing similar to cerebrospinal fluid) but are characteristically markedly bright on DWI. This latter feature can be particularly useful in differentiating epidermoid tumors from arachnoid cysts. In addition, in contrast to arachnoid cysts, epidermoids do not suppress their signal on FLAIR sequences, on which they typically show a “dirty” appearance. (B) Lymphomas show restricted diffusion of DWI due to their dense cellularity, although they usually are not as bright as epidermoid tumors. Untreated lymphomas enhance avidly and homogeneously, except in patients with HIV/AIDS, who commonly present with necrotic changes. (C) Meningiomas may show some degree of diffusion restriction on DWI, but their appearance is variable. Atypical and malignant meningiomas tend to show greater restricted diffusion with lower apparent diffusion coefficient values. These tumors enhance. (D) Marked hyperintensity on DWI is not a usual characteristic of craniopharyngiomas, which also would enhance. These tumors are heterogeneous with 90 to 95% showing calcifications. (E) Arachnoid cysts have the same signal appearance as cerebrospinal fluid on all sequences and do not show restricted diffusion. A Tuberculosis Tuberculosis in the vertebral bodies (Pott disease) classically is associated with back pain, a low-grade fever, and destruction of the vertebral bodies with disk preservation. (B) Staphylococcus aureus infection (often from hematogenous spread) can result in vertebral body osteomyelitis or diskitis. The latter is seen radiographically as disk space destruction, whereas both the former and latter are characterized by more substantial signs of infection and fever relative to Pott disease. (D) Vertebral body hemangiomas often are asymptomatic, but may cause vertebral body collapse and associated pain. (E) An osteoid osteoma is a benign osteoblastic bone tumor characterized by a dull, nonradiating pain often relieved by nonsteroidal anti-inflammatory medications. B PaO2 < 90 The prerequisites for determination of brain death include the absence of reversible causes of coma (e.g., hepatic, diabetic, and uremic causes); imaging supporting the clinical exam findings; lack of respiratory effort; lack of severe acid-base, electrolyte, or endocrine abnormalities; PaO2 > 90 for at least 30 minutes; systolic blood pressure > 100 mm Hg for at least 30 minutes; negative drug screen; no residual paralytics; and core body temperature > 35°C. D Posterior inferior cerebellar artery The patient’s clinical symptoms are consistent with Wallenberg syndrome due to a lateral medullary infarction, which can be confirmed on the diffusion-weighted image. Infarction of the lateral medulla can occur secondary to occlusion of the posterior inferior cerebellar artery or one of its branches with or without involvement of the vertebral artery. (A) The pontomesencephalic segment belongs to the superior cerebellar artery and supplies part of the pons and mesencephalon. (B) The anterior inferior cerebellar artery supplies the anterior and inferior portions of the cerebellar hemispheres as well as the inferolateral aspect of the pons and flocculus. (C) The superior cerebellar artery supplies the superior cerebellum, superior vermis, dentate nuclei, and part of the midbrain. C GABA GABA is released by Purkinje cells in the cerebellum as they make inhibitory projections to the deep cerebellar nuclei and supply the sole motor coordination output of the cerebellar cortex. (A) Glutamate is the most abundant excitatory neurotransmitter in the central nervous system and is the primary neurotransmitter released by cerebellar granule cells. (B) Glycine is an inhibitory neurotransmitter found most predominantly in the brainstem, retinae, and spine. In the spine, it is released by Renshaw cells. (D) Acetylcholine is found throughout the nervous system but is a prominent neurotransmitter in the autonomic nervous system and at neuromuscular junctions. (E) Substance P is a neuropeptide that acts as a neurotransmitter for transmitting pain to the central nervous system. A Diabetes insipidus Preoperative central diabetes insipidus has been reported in 8 to 35% of patients affected by a craniopharyngioma. The condition occurs in 70 to 90% of patients after surgery. C Increase urine calcium excretion Urine calcium excretion is increased by steroids, resulting in a lower serum calcium concentration and promotion of parathyroid hormone to induce bony reabsorption. (A) Steroids inhibit osteoblast function to slow bony modeling. (B) Steroids promote osteoclast reabsorption of the bony matrix. (E) Gastrointestinal calcium absorption is decreased by steroids. B Iris hamartomas Iris hamartomas (Lisch nodules) are seen in neurofibromatosis (NF) type 1. This patient has NF type 1, as she has two of the diagnostic criteria, which include family history, Lisch nodules, optic gliomas, café-au-lait spots, axillary or groin freckling, multiple neurofibromas or a single plexiform neurofibroma (a cluster of neurofibromas involving multiple nerves), and skeletal abnormalities (e.g., sphenoid dysplasia). (A) Bilateral acoustic neuromas are found in NF type 2. (C) An increased risk of meningiomas and other intracranial tumors (e.g., ependymomas) is associated with NF type 2. (D) Pigmented spots encircling the iris is descriptive of Kayser-Fleischer rings seen in Wilson disease. (E) Multiple schwannomas are seen in schwannomatosis, which results from mutations on both chromosomes 17 and chromosome 22. A Unaffected Sensory nerve action potentials (SNAPs) are unaffected with lesions proximal to the dorsal root ganglion (e.g., nerve root avulsions, herniated disks) because the cell bodies are unaffected. Postganglionic lesions reduce the SNAP amplitude and/or slow the velocity. A Ependymomas This patient has avidly enhancing masses in his internal auditory canals bilaterally, with extension into the cerebellopontine angle cistern on the right, consistent with vestibular schwannomas. The presence of bilateral vestibular schwannomas satisfies the modified NIH criteria for NF type 2, which also may present with schwannomas and ependymomas, the latter usually in the brainstem and spinal cord. Schwannomas usually are hyperintense on T2 sequences, and larger tumors commonly have cystic changes. (B) Sphenoid wing dysplasia is a distinctive osseous lesion of NF type 1 and constitutes a major criterion for diagnosis. (C) Calcified subependymal nodules are seen in tuberous sclerosis and show calcification in the majority of patients, except in early life. (D) Leptomeningeal angiomatosis is a capillary venous malformation seen in Sturge-Weber-Dimitri syndrome, usually accompanied by a port-wine stain along the ophthalmic and maxillary trigeminal nerve distributions. (E) Endolymphatic sac tumors are seen in 10% of patients with von Hippel–Lindau syndrome and are not a feature of neurofibromatosis. D Demeclocycline Demeclocycline is a tetracycline that can be used to treat chronic syndrome of inappropriate antidiuretic hormone secretion, in that it is a partial antagonist of the actions of antidiuretic hormone on the distal renal tubules. It can be given orally every 6 hours. E Rabies The image accompanying the question shows Negri bodies, which are intracytoplasmic eosinophilic collections of ribonucleoproteins seen in rabies. (A) Alzheimer disease is characterized histologically by intracellular neurofibrillary tangles (silver staining and immunoreactive for tau protein) and extracellular senile plaques (silver staining with a core of protein amyloid). Hirano bodies can be seen, and these are rod-shaped eosin inclusions. There also can be diffuse cortical vacuolization where the vacuoles appear glassy or eosinophilic. (B) Parkinson disease is characterized by intracellular Lewy bodies that derive from neurofilaments and are laminated with an eosinophilic core and a clear halo. (C) Lafora bodies are seen in Lafora disease, and these are round, basophilic polyglucosans. (D) Creutzfeldt-Jakob disease displays diffuse cortical vacuolization as sometimes seen in Alzheimer disease. A Langerhans cell histiocytosis Langerhans cell histiocytosis is characterized by infiltration of the soft tissues with myeloid dendritic cells. In children, the skull is the most common site of involvement and represents 40% of cases. Lesions usually are well marginated and may have a beveled edge on skull radiographs or CT due to unequal involvement of the inner and outer tables. This also can lead to the appearance of a “hole within a hole” if viewed en face. (B) Calvarial hemangiomas are slow-growing lesions that can result in a characteristic sunburst-like trabecular thickening or radiating spicules. Margins usually are not sclerotic. (C) Primary intraosseous meningiomas are rare. They also can present with a radiating pattern but are not associated with a beveled edge. (D) Metastases can have various presentations from ill-defined and infiltrative to relatively well marginated. They usually are not associated with a beveled edge. C A-delta and C fibers A-delta and C fibers are nociceptive fibers that are thought to be the cause of pain in trigeminal neuralgia, and these are the theoretical targets of lesioning procedures. In reality, it is impossible to select completely for these fibers, but creating a retrogasserian lesion tends to reduce pain while best avoiding hypesthesia. (A) A-alpha and beta fibers are sensory (fine touch) fibers that should be preserved during a percutaneous trigeminal rhizotomy. B Anterior nuclei The anterior nuclei are part of the limbic system and project to the cingulate gyrus. (A) The centromedian nuclei are part of the intralaminar nuclei and project to the putamen and subthalamic nuclei. They receive input from multiple structures including the cerebral cortices. They are involved in attention and arousal. (C) The ventral lateral nuclei are involved in motor coordination and receive projections from the cerebellum and basal ganglia. (D) The lateral posterior nuclei are associated with the pulvinar nuclei and have similar inputs and outputs. They are part of the visual pathways. (E) The medial dorsal nuclei receive inputs from the olfactory cortices and amygdalae and project to the limbic system and prefrontal cortices. C Right trochlear nerve palsy A right trochlear nerve palsy results in a right pupil that deviates superiorly and extorts in primary gaze as the superior oblique muscle (supplied by the nerve) has the action of moving the eye inferiorly when adducted and intorting the eye. A tilt of the head to the side contralateral of the palsy and a slight tilt downward enables the contralateral eye to align its sight with the paretic eye when looking at objects on a level plane. When looking downward, the ipsilateral eye fails to align the gaze with the contralateral eye. (A) A left trochlear nerve palsy typically results in the patient compensating with a head tilt to the right due to the loss of the intorsion action of the superior oblique. (B) A left oculomotor nerve palsy results in the left pupil being directed downward and laterally due to the unopposed action of the lateral rectus and superior oblique muscles. A patient should have no difficulty aligning her gaze when looking downward. (D) A right oculomotor nerve palsy results in the right pupil being directed downward and laterally. (E) Internuclear ophthalmoplegia results from a medial longitudinal fasciculus lesion and does not cause convergence deficits but does manifest in an adduction deficit in the ipsilateral eye when gaze is directed contralateral to the lesion. Abduction nystagmus also appears in the contralateral eye when gaze is directed contralateral to the lesion. A Anterior atlanto-occipital dislocation The basion-axial interval (BAI) represents the distance measured between a line drawn along the dorsal aspect of the dens (posterior axial line) and the tip of the basion. Studies have demonstrated that this distance measures less than 12 mm in more than 95% of adults, and this is considered to be the upper limit of normal. A BAI greater than 12 mm is indicative of anterior atlanto-occipital dislocation where the cranium is displaced anteriorly in relation to the spine. (B) Atlantoaxial instability would present as an abnormally increased distance between the anterior surface of the dens and the posterior tubercle of C1 (the atlantodental interval). This distance normally measures 3 mm or less in adults and 5 mm or less in children. (C) Longitudinal dislocation can present with a normal BAI if there is no anterior translocation of the cranium. (D) A BAI greater than 12 mm is abnormal. (E) Atlanto-occipital dislocation results from traumatic injury to the alar and apical ligaments and tectorial membrane, which allows the cranium to move with respect to the cervical spine. Injury to the transverse ligament would result in atlantoaxial instability. E Tongue fasciculations, atrophy of the hands, and lower extremity hyperreflexia Amyotrophic lateral sclerosis (ALS) classically is an upper and lower motor neuron disease with sparing of cognition and autonomic function. Classically, there is sparing of the eye muscles, sensation, and urinary sphincter control. ALS is due to the degeneration of the anterior horn α-motor neurons in the spinal cord and brainstem nuclei. The condition often is sporadic; however, familial forms are associated with the superoxide dismutase gene (SOD) mutation. (A) Tongue fasciculations, atrophy of the hands, and lower extremity hyporeflexia are lower motor neuron findings. (B) Forehead-sparing facial weakness, spasticity of the hands, and lower extremity hyperreflexia are signs of pure upper motor neuron disease. (C) Progressive weakness (proximal more than distal), areflexia, and bilateral facial weakness with little to no sensory involvement may be seen in Guillain-Barré syndrome. This condition may occur after Campylobacter jejuni enteritis. Cerebrospinal fluid analysis shows albuminocytologic dissociation. (D) Central cord syndrome classically results in a motor deficit worse in the upper than lower extremities, with varying degrees of sensory findings and myelopathy (usually urinary retention) that occurs with hyperextension injury or central cervical canal stenosis. D 90% Dandy-Walker variant is a less severe posterior fossa anomaly characterized by partial agenesis of the cerebellar vermis as compared with the more severe, classic Dandy-Walker malformation, in which there is complete agenesis of the cerebellar vermis. Hydrocephalus is present and typically symptomatic in 90% of children with a Dandy-Walker malformation compared with 25% of children with a Dandy-Walker variant. C 80 Gy in a single dose directed at the center of the lesion During stereotactic radiosurgery for trigeminal neuralgia, 70 to 80 Gy of radiation in a single dose should be directed at the center of the lesion in such a way as to keep the 80% isodose curve away from the brainstem. Pain relief usually occurs 3 months after treatment but is highly variable. A Follow the ex-wife’s orders, and do not provide any further medical care. There are two types of power of attorney: (1) immediate and (2) springing. An immediate power of attorney becomes effective as soon as it is signed, whereas a springing power of attorney becomes effective when the principal becomes incapacitated. In most states, a divorce decree does not revoke a financial or health care power of attorney in favor of the ex-spouse. Exceptions to this rule occur in Alabama, California, Colorado, Illinois, Indiana, Kansas, Minnesota, Missouri, Ohio, Pennsylvania, Texas, Washington, and Wisconsin, where divorce does revoke such a designation. In these states, or when there is not someone available with the legal right to make medical decisions for the patient, the physician should act in the best interests of the patient, providing all reasonable care that is not considered futile. (B, C) Consulting the hospital’s ethics committee and obtaining a court order require a substantial amount of time and are difficult to do in emergent situations. (D) Regardless of who has the legal right to make medical decisions, if time permits it always is prudent to attempt to obtain a family consensus regarding care plans, as this tends to mitigate any potential legal implications and unrest within a family. C Carotid canal The structure indicated by the arrow in the image accompanying the question corresponds to the carotid canal, which transmits the internal carotid artery and sympathetic plexus. (A) The petroclival fissure is seen more posteriorly, coursing somewhat parallel to the petrous carotid canal. (B) The pars nervosa is the smaller anteromedial component of the jugular foramen and is separated from the larger pars vascularis by the jugular spine. It carries cranial nerve IX and the inferior petrosal sinus. (D) The foramen rotundum courses anteriorly along the medial aspect of the middle cranial fossa and transmits the maxillary branch of cranial nerve V, artery of the foramen rotundum, and emissary veins. (E) The foramen ovale is seen in the right greater wing of the sphenoid bone. It contains the mandibular branch of cranial nerve V, accessory meningeal artery, otic ganglion, emissary veins, and sometimes the lesser petrosal nerve. B 3.2 L The estimated water deficit is either 3.1 or 3.3 L depending on which of the following equations is used: or D Osteopetrosis Osteopetrosis is secondary to defective osteoclastic function, with a resultant dense appearance of the bone. In the spine, thick and dense bands of sclerosis can be seen paralleling the end plates as in this case. (A) Ochronosis may result in widespread calcification of the intervertebral disks. (B) Paget disease usually is more focal, and characteristically results in expansion of the involved bone. A “picture frame” appearance of the vertebra with a squared morphology often is seen. (C) Blastic metastases can be diffuse, particularly in patients with breast cancer. They would not be as densely homogeneous as in this case. C Commissural myelotomy Commissural myelotomies are used for either unilateral or bilateral pain below the thoracic levels. They are not the ideal choice for visceral pain, as they work through disruption of the lateral spinothalamic tract fibers as they cross in the anterior commissure. (A) A bilateral cervical cordotomy carries a risk of an Ondine curse, with a loss of respiratory automaticity. Bilateral procedures should be staged in selected patients, with cordotomies as a whole being reserved mostly for terminally ill patients due to a variety of complications. In addition, a unilateral cordotomy often accentuates contralateral pain. (B) Punctate midline myelotomies are used best for visceral and pelvic pain and can be used in non–terminally ill patients. (D) Spinal cord stimulation is an excellent choice for bilateral lower extremity pain but has a poor response on pain secondary to cancer. It is not a good procedural choice for a patient with a short life expectancy. (E) Dorsal root entry zone (DREZ) lesioning typically helps with noncancer pain that can be isolated to specific nerve roots. It is used often following nerve root avulsions. In the patient described, there seems to be pain involving numerous nerve roots. B Optic nerve gliomas tend to be low grade in children and high grade in adults. Optic nerve gliomas tend to be of a higher grade with advancing age of presentation. (A) Optic nerve gliomas can occur at any age but appear earlier in life, when they are associated with neurofibromatosis type 1. (C) Rosenthal fibers occur in optic nerve gliomas, especially when they are low-grade pilocytic tumors. They are more common in childhood. (D) Optic nerve gliomas typically are not a manifestation of neurofibromatosis type 2 in children or adults. B Gorlin syndrome The image accompanying the question shows a medulloblastoma. Gorlin syndrome (autosomal dominant inheritance) occurs in approximately 1 to 2% of medulloblastomas and is characterized by the propensity to develop multiple invasive basal cell carcinomata. Other syndromes associated with medulloblastomas are Li-Fraumeni and Turcot syndromes. (A) Von Hippel-Lindau (VHL) disease results from an autosomal dominant mutation of the VHL gene on chromosome 3. VHL disease is associated with central nervous system hemangioblastomas; retinal hemangioblastomas; renal cell carcinomas; pheochromocytomas; cysts in the liver, pancreas, and kidneys; and epididymal cystadenomas. (C) Tuberous sclerosis can be an autosomal dominant disease but usually occurs sporadically. The associated mutation is located on chromosomes 9 and 16. Tuberous sclerosis can be characterized by the classic triad (in less than 50% of cases) of mental retardation, seizures, and adenoma sebaceum. The condition is associated with cortical tubers; subependymal giant cell astrocytomas; cardiac rhabdomyomas; renal angiomyolipomas; cysts in the lungs, liver, and spleen; pancreatic adenomas; and retinal hamartomas. (D) Lynch syndrome is a cancer syndrome primarily involving the colon, but may affect many other organ systems including the brain. It is formerly known as hereditary nonpolyposis colon cancer syndrome. A Extensor carpi radialis longus The extensor carpi radialis longus is innervated by the radial nerve itself but may occasionally have innervations from the superficial sensory branch of the radial nerve. (B–E) These muscles are innervated by the posterior interosseous nerve, a terminal branch of the radial nerve. C Day 15 The primitive streak appears around day 15 of embryogenesis due to signaling from the notochord, and it marks the initiation of gastrulation. During this process, the bilaminar disk becomes trilaminar with the development of the endoderm, mesoderm, and ectoderm. The primitive streak defines the various axes of the embryo and continues to transform into the primitive groove. This groove further develops into the neural tube during neurulation. (A) The bilaminar disk forms during the first part of the second week of embryogenesis. (B) Around or before the start of the second week of embryogenesis, the notochord forms. (D) Primary neurulation (the creation of the neural plate to create the neural tube) begins around the start of the third week of embryogenesis. The notochord plays an integral role in this process through signaling and mechanical support. (E) In secondary neurulation, the neural tube arises from a solid cord that then cavitates, resulting in a hollow tube. This tube eventually forms the medullary and spinal cords that then connect to the cord arising from primary neurulation. This process begins around day 26 of embryogenesis. B Arteriovenous fistula The presence of longitudinally extensive signal abnormality in the spinal cord associated with vascular flow voids (which are best seen on the T2 image) is compatible with a spinal dural arteriovenous fistula. These typically occur in older males who present with progressive myelopathy and sometimes neurogenic claudication (thought to be related to venous hypertension and vascular congestion). As in this case, ill-defined contrast enhancement may be present. (A) Acute spinal cord ischemia can result in longitudinally extensive intramedullary signal abnormalities, but usually has a hyperacute presentation and would not explain the presence of vascular flow voids. (C) Infiltrating neoplasms such as astrocytomas usually result in more focal spinal cord expansion than shown in the image accompanying the question. They may show variable degrees of contrast enhancement, which tends to be more heterogeneous. (D) Demyelination related to neuromyelitis optica can lead to longitudinally extensive signal abnormalities in the spinal cord, with a central gray matter pattern with possible patchy enhancement. This would not explain the patient’s clinical presentation, as attacks in neuromyelitis optica usually occur over days with variable degrees of recovery over weeks to months on the flow voids on the MRI scan. The lesions in multiple sclerosis are more focal and peripheral in the white matter, although they may coalesce over time in severe disease. (E) The most common etiology of infectious myelitis is viral. This would have a more rapid clinical course and would not be associated with vascular flow voids. B AEDs decrease the rate of acute but not delayedonset seizures. Phenytoin has been demonstrated to decrease the risk of early posttraumatic seizures by fourfold; however, it has this effect on seizures only within the first week after injury. D Foramen magnum tumor Foramen magnum tumors (most commonly meningiomas) classically present with rotating paralysis as described in the vignette presented in the question. Other symptoms may include craniocervical pain, myelopathy, and intrinsic hand muscle atrophy (lower motor neuron findings from venous infarction). Another classic sign of cervicomedullary compression is downbeat nystagmus. C Glasscock The Glasscock triangle (posterolateral) contains the middle meningeal artery in the floor of the triangle as it exits the foramen spinosum, the horizontal petrous internal carotid artery, and the infratemporal fossa. The triangle is useful, as it enables the surgeon to gain proximal control of the internal carotid artery for more distal vascular procedures. Approximately 10 mm of the carotid artery is accessible through this triangle. (A) The oculomotor triangle, also known as the medial or Hakuba triangle, contains the oculomotor nerve and horizontal segment of the internal carotid artery. It is the triangle by which access to most intracavernous aneurysms and tumors is gained. (B) Historically, the Parkinson triangle was accessed to treat carotid-cavernous fistulas. It also contains the abducens nerve. (D) The Kawase (posteromedial) triangle contains the petrous apex, internal carotid artery, cochlea, and vertebrobasilar junction. It can be used to perform an anterior petrosectomy so that the posterior fossa, anterior brainstem, and root of the trigeminal nerve can be visualized. (E) The porus trigeminus is the entrance to the Meckel cave and is contained within the inferolateral triangle. C Hypertension, bradycardia, and respiratory irregularity The Cushing reflex is a physiological response to an increase in intracranial pressure. It manifests with an increase in blood pressure, decrease in heart rate, and irregular breathing. The proposed mechanism for the Cushing triad is an increase in intracranial pressure leading to decreased cerebral blood flow, and the sympathetic system causes peripheral vasoconstriction to elevate the mean arterial pressure in an attempt to restore normal cerebral blood flow. As this happens, baroreceptors in the aortic arch detect the blood pressure increase, and trigger a parasympathetic response to decrease the heart rate. Increased intracranial pressure leads to brainstem compression and irregular breathing. A Gross total resection Approximately 85% of ependymomas present as localized disease. Gross total resection is the most important predictor of outcome. (C) Conformal field radiotherapy is recommended as an adjuvant therapy in most patients with ependymomas. (D) Early chemotherapy for ependymomas is recommended in infants to delay or avoid the need for radiotherapy, which can be very detrimental to brain development. D Cutaneous bruising In the images accompanying the question, the MRI scan on the left shows hemispheric subdural hematomas bilaterally, with different signal intensities and therefore likely different ages. The susceptibility-weighted image on the right shows a dark focus of signal drop along the posterior aspect of the left globe compatible with retinal hemorrhage. Together, these findings are highly concerning for nonaccidental trauma. Subdural hematomas are associated significantly with nonaccidental trauma compared with unintentional trauma, and retinal hemorrhages have a specificity of approximately 94%. Cutaneous bruising may be present and should raise suspicion for trauma in a nonambulatory child. (A) An abdominal mass would not explain the findings of this case. (B) Opisthotonos is abnormal rigidity with arching of the body and may be seen in infants with meningitis. (C) Fever may be seen in infectious meningitis. D Visual flashes If a deep brain stimulating electrode contacts the optic tract (inferomedial to the globus pallidus), a patient can experience phosphenes, which are flashes or sparkles of light in the contralateral visual field. (A) To cause perspiration and mydriasis, a lead would have to be inserted significantly medial to the globus pallidus to contact the hypothalamus. (B, C) If a deep brain stimulating electrode is passed too medially to the globus pallidus, stimulation of the internal capsule can cause contractions of the tongue, face, and throat as well as dysarthria, gagging, and visible muscle contractions. B Sodium ions would enter the neuron, and membrane potential would become more positive. Even at maximal sodium conductance at the peak of an action potential, the neuronal membrane potential is not equal to the equilibrium potential for sodium ions. This is due to the baseline conductance of other ions including chloride and potassium. Additional open sodium channels would allow more sodium ions to enter the cell, increasing the relative concentration of sodium ions, and bringing the cell to a more positive membrane potential (closer to the sodium equilibrium potential). A Labyrinthitis Labyrinthitis (as opposed to vestibular neuritis) involves the vestibular nerve as well as the cochlea and thus also affects hearing. (B) Vestibular neuronitis presents with acute vertigo without hearing loss, usually after an upper respiratory tract infection. (C) Benign positional vertigo is associated with nystagmus and vertigo without hearing loss that are associated with positional changes. (D) Meniere disease includes vertigo and prominent tinnitus with hearing loss that classically is fluctuating and episodic, lasting minutes to hours. (E) Stroke (Wallenberg or lateral medullary syndrome) causing vertigo, nystagmus, and hearing loss also would produce prominent nonvestibular symptoms such as loss of pain/temperature sensation in the contralateral body, Horner syndrome, and brainstem findings such as dysphagia, ataxia, diplopia, and dysarthria. C Cerebral angiopathy In cerebral angiopathy, there is a deposition of β-amyloid protein into hyalinized cerebral vessels. Congo red stains the amyloid protein red. (A) Arteries in moyamoya disease display varying degrees of stenosis due to thrombosis, luminal collapse, and fibrous intimal thickening. (B) Cavernous hemangiomas (cavernomas) appear as dilated, thin-walled capillaries without normal intervening brain tissue. There can be surrounding hemosiderin. (D) Mucormycosis is a family of invasive fungal infections typically associated with diabetes. Histologically, thin-walled hyphae appear arranged and folded haphazardly and branching from the parent hyphae at right angles. (E) Radiation necrosis appears as areas of anuclear brain tissue with reactive astrocytes. Arteriosclerosis (vessel thickening) also can be seen. B Tibial and common peroneal nerves The sural nerve is composed of contributions from the lateral and medial sural cutaneous nerves. The lateral sural cutaneous nerve arises as a terminal branch of the tibial nerve, whereas the medial sural cutaneous nerve is a branch of the common peroneal nerve before it bifurcates into the deep and superficial peroneal nerves. C Dandy-Walker malformation The combination of a large posterior fossa cyst in communication with the fourth ventricle, elevation of the torcular, and vermian hypoplasia is compatible with Dandy-Walker malformation, in this case resulting in obstructive hydrocephalus. Associated findings may include corpus callosum agenesis and lipomas, neuronal migration anomalies, and cephaloceles. (A) An arachnoid cyst rarely occupies the entire posterior fossa and is not accompanied by vermian hypoplasia. (B) A Blake pouch cyst develops due to failure of regression of the embryonic Blake pouch, which then balloons posteriorly into the cisterna magna. The vermis is not hypoplastic. (D) A mega cisterna magna has an intact vermis and normal fourth ventricle, and would not result in this degree of posterior fossa expansion. B Engorgement of the extraocular muscles This patient has a cavernous-carotid fistula characterized by exophthalmos and possibly an optic bruit when a stethoscope is placed over the ipsilateral closed eye. This type of arteriovenous fistula increases the venous pressure in the cavernous sinus, resulting in inhibited drainage of blood from the extraocular muscles. (A) An orbital mass can produce exophthalmos but would not produce an orbital bruit. (C) It is the ophthalmic vein and not the artery that becomes enlarged in a cavernouscarotid fistula as the venous pressure increases. (D) A cavernous sinus aneurysm produces the described symptoms only if it ruptures and results in a carotid-cavernous fistula. (E) In conditions such as elevated intracranial pressure there can be flattening of the posterior aspect of the globe. A carotid-cavernous fistula is not expected to produce global elevations in intracranial pressure. B Septal and thalamostriate veins (A) The internal cerebral vein joins with the basal vein of Rosenthal to form the vein of Galen. (C) The vein of Galen joins the inferior sagittal sinus to form the straight sinus. (D) The caudate vein drains into the thalamostriate vein. D Partially compensated respiratory acidosis A low pH indicates acidosis, whereas a high PCO2 is indicative of a respiratory origin. There is partial metabolic compensation as indicated by the rise of the bicarbonate level above normal. Compensatory mechanisms never fully reverse the primary acid/base abnormality. C Combined respiratory and metabolic alkalosis A high pH indicates alkalosis, whereas a combined low PCO2 and high bicarbonate level is indicative of a combined respiratory and metabolic origin. (A) A high pH indicates alkalosis, whereas a low PCO2 and normal bicarbonate level is indicative of a respiratory origin. (B) A low pH indicates acidosis, whereas a low bicarbonate level and a relatively normal PCO2 is indicative of a metabolic origin. Normal target labs values are as follows: pH: 7.40 PCO2: 40 mm Hg HCO3−: 24 mEq/L C This disease typically is inherited in an X-linked fashion. The patient has underproduction of the pituitary hormone gonadotropin, resulting in Kallmann syndrome (hypogonadotropic hypogonadism). It is an X-linked (typically) condition that is more common in men (incidence of 1:10,000) than in women (incidence of 1:50,000). Imaging would be expected to demonstrate aplasia/hypoplasia of the olfactory bulbs. Of note, there are some reported forms of Kallmann syndrome inherited in an autosomal dominant pattern. A Bicoronal sutures Crouzon syndrome first was described in 1912. Inheritance is autosomal dominant with virtually a complete penetrance. It is due to multiple mutations in the fibroblast growth factor receptor 2 gene (FGFR2). Features of the skull are variable, but the skull may have associated brachycephaly, trigonocephaly, or oxycephaly. These conditions occur with premature fusions of the sagittal, metopic, or coronal sutures, with bilateral coronal sutures being the most commonly affected. In addition, the orbits are shallow, with resulting exorbitism due to anterior positioning of the greater wing of the sphenoid. The middle cranial fossa is displaced anteriorly and inferiorly, which further shortens the orbit anteroposteriorly. D Bacterial endocarditis Conditions associated with aneurysms include autosomal dominant polycystic kidney disease, fibromuscular dysplasia, arteriovenous malformations, Ehlers-Danlos syndrome type 4, Marfan syndrome, familial intracranial aneurysm history, aortic coarctation, Osler-Weber-Rendu syndrome, and endocarditis. Intracranial aneurysms also are associated with hypertension, smoking, alcohol, trauma, obesity, and advancing age. Bacterial endocarditis can cause mycotic aneurysms mainly in the distal, smaller arteries. (A) Radiation exposure is more likely to cause meningiomas than aneurysms. (B) Ehlers-Danlos syndrome is a connective tissue disorder with six types. Each type shares features of joint laxity and soft skin. Types 1 and 2 are the classic types with hypermobile, stretchy skin. Type 3 is the most common and is marked by joint hypermobility. Type 4 is vascular and makes those affected prone to aneurysm development. Type 6 is characterized by a progressive kyphoscoliosis, thin conjunctiva, and severe muscle weakness. Types 7A and B comprise the arthrochalasia types and are characterized by very loose joints and bilateral hip dislocations. These types can be considered severe forms of the hypermobility type. Type 7C is the extremely rare dermatosparaxis type characterized by extremely fragile and sagging skin. Note that the six subtypes are not numbered consecutively. (C) Illicit drug use indirectly can cause mycotic aneurysms in rare cases if a patient has bacterial endocarditis. (E) There is no gender predisposition for aneurysm development. B Aneurysmal bone cyst Aneurysmal bone cysts are expansile, tumor-like, osteolytic lesions often occurring in the posterior elements of the spine. There is a high recurrence rate if they are not excised completely. (C, D) Osteoid osteomas (less than 1 cm) and osteoblastomas (1 cm and larger) characteristically respond well to aspirin. (E) Eosinophilic granulomas often present with an osteolytic defect and progressive vertebral collapse (vertebra plana) most commonly affecting the cervical spine. B Desmoplastic infantile ganglioglioma The tumor shown in the image accompanying the question best fits with a desmoplastic infantile ganglioglioma. (A) Desmoplastic infantile astrocytomas lack the ganglion cell component highlighted with synaptophysin staining. (E) Pleomorphic xanthoastrocytomas also are reticulin rich but show more atypia and are rare in the frontal lobe. C Progressive supranuclear palsy Progressive supranuclear palsy (PSP) causes paresis of primary vertical gaze, with preservation of the vertical doll’s eyes maneuver, pseudobulbar palsy, and axial dystonia. PSP may be distinguished from Parkinson disease in that patients with PSP walk upright (not bent forward), have no tremor, and have a short-lived response to anti-Parkinson medications. B 2 Hunt and Hess grade 2 indicates a severe headache, nuchal rigidity, and cranial nerve palsies. Of note, serious systemic disease can increase the Hunt and Hess grade of the patient. (A) Grade 1 indicates an asymptomatic patient or one with only a mild headache. (C) Grade 3 indicates focal neurologic deficits, lethargy, and confusion, and should be an indicator for possible external ventricular placement. (D) Grade 4 indicates stupor, hemiparesis, and decorticate posturing. (E) Grade 5 indicates coma, decerebrate posturing, and a moribund appearance. D Cerebellar infarcts This patient has a minimally displaced fracture of the left lateral mass of a cervical vertebra extending to the foramen transversarium. These patients are at an increased risk of vertebral artery injury, which may be complicated by posterior circulation infarcts. This finding warrants additional evaluation with CT or MR angiography. (A) Intraabdominal injuries are a common finding with Chance type fractures of the thoracolumbar spine, particularly in children. (B) Spinal cord transection may be present with more severe cervical spine injuries, although patients with underlying spinal canal stenosis are at an increased risk of spinal cord injury with relatively minor trauma. (C) Anterior circulation infarcts can result from carotid artery dissection or other injury. B 3 to 5%; 64% reduction The CHADS2 score is used to assess the annual risk of stroke in patients with atrial fibrillation, and it increases for patients with congestive heart failure, hypertension, diabetes, previous transient ischemic attacks (TIAs) or strokes, and an age greater than 75 years. When calculating a CHADS2 score, each of these variables receives 1 point, except for previous TIAs/strokes, which receives 2 points. A CHADS2 score of 2 imparts a 4% annual stroke risk, which is a three- to fivefold increase in the risk of stroke compared with non–atrial fibrillation patients. Warfarin use increases complications related to bleeding (0.4% per year risk of bleeding complications, with a 0.2% per year risk of intracranial hemorrhage), but decreases the relative risk of stroke by 64% and the absolute risk of stroke by 2.7% per year. Warfarin also performs better than antiplatelet agents with regard to stroke risk reduction. D Autosomal recessive microcephaly Mutations in the MCPHi or cyclin-dependent kinase 5 regulatory associated protein 2 are associated with autosomal recessive microcephaly (microcephaly vera). Microcephaly refers to a head circumference more than two standard deviations below the mean for age and gender after factoring in intrauterine growth retardation and low birth weight/body length. D Calcification and hemorrhage are common. The microscopic and staining properties of the lesion shown in the images accompanying the question as well as its imaging characteristics are compatible with an ependymoma. On the MRI, this lesion shows cystic or necrotic changes and avid enhancement, and extrudes through the foramen magnum (sagittal image) and right foramen of Luschka (axial image) in a “toothpaste” configuration. Calcification and hemorrhage are common and contribute to the heterogeneity of these lesions. Ependymomas most commonly are found in children but can occur at any age. (A) Ependymomas can occur anywhere but typically arise from the floor of the fourth ventricle. Medulloblastomas classically arise from the roof of the fourth ventricle but also can occur in the cerebellar peduncles and cerebellar hemispheres. (B) Ependymomas are associated with neurofibromatosis type 2 and not type 1. (C) Hemangioblastomas are tumors that most commonly occur in the posterior fossa and spinal cord and may be complicated by polycythemia due to their production of erythropoietin. E Diencephalon, basal ganglia, and cerebral hemispheres The Cheyne-Stokes respiration pattern originates in telencephalic and diencephalic structures. C Administration of meperidine Meperidine is an opioid agonist that can lower the seizure threshold. (A) Cerebral hypotension causes postural headaches rather than seizures. (B) The vasovagal response to pain causes bradycardia rather than tachycardia. (D) A recurrent disk herniation reproduces radicular symptoms rather than seizures. (E) Chemical meningitis is theoretically possible but very unlikely in this case. D It may present with acute brain herniation and death. The displayed sagittal, noncontrast T1 sequence shows a bright lesion in the anterior aspect of the third ventricle compatible with a colloid cyst. Note a brighter spot within it (known as “fried egg” appearance) and enlargement of the lateral ventricles with thinning and bowing of the corpus callosum. Patients with a colloid cyst may present with rapid brain herniation, hydrocephalus, and death if there is acute ventricular obstruction. (A) Colloid cysts are derived from embryonic endoderm. (B) Symptoms in colloid cysts are related to ventricular obstruction (intermittent or acute), and patients may present with headaches, nausea, and vomiting. Patients with acute obstruction, herniation, and hydrocephalus can have mental status changes and deteriorate rapidly. (C) In colloid cysts, MR spectroscopy may show a large peak that resembles N-acetylaspartate; however, normal brain metabolites are absent. Elevated levels of alanine at short TE are seen in meningiomas and not in colloid cysts. (E) Calcification and regions of nodular enhancement are features of craniopharyngiomas. Calcification in colloid cysts is rare, and they do not enhance. A Oculomotor The oculomotor triangle, also known as the medial or Hakuba triangle, contains the oculomotor nerve and horizontal segment of the internal carotid artery. It is the triangle by which access to most intracavernous aneurysms and tumors is gained. (B) Historically, the Parkinson triangle was accessed to treat carotid-cavernous fistulas. It also contains the abducens nerve. (C) The Glasscock triangle (posterolateral) contains the middle meningeal artery in the floor of the triangle as it exits the foramen spinosum, horizontal petrous internal carotid artery, and infratemporal fossa. The triangle is useful, as it enables the surgeon to gain proximal control of the internal carotid artery for more distal vascular procedures. Approximately 10 mm of the carotid artery is accessible through this triangle. (D) The Kawase (posteromedial) triangle contains the petrous apex, internal carotid artery, cochlea, and vertebrobasilar junction. It can be used to perform an anterior petrosectomy so that the posterior fossa, anterior brainstem, and root of the trigeminal nerve can be visualized. (E) The porus trigeminus is the entrance to the Meckel cave and is contained within the inferolateral triangle. C Craniopharyngioma Craniopharyngiomas are benign histologically, extra-axial, and slow-growing tumors that predominantly involve the sella and suprasellar space. On CT, the adamantinomatous-type tumor appears as a predominately cystic mass with a solid component in more than 90% of cases. On MRI, the tumors predominantly are cystic suprasellar masses with a solid, contrast-enhancing component as well. Characteristic calcifications commonly are seen. B Pleomorphic xanthoastrocytoma The patient’s age and history as well as the imaging characteristics of this intra-axial mass strongly favor pleomorphic xanthoastrocytoma (PXA). PXAs usually are supratentorial, occur most commonly in the temporal lobes, and have areas of mixed cystic change and enhancing nodules. They typically show extension peripherally to the dura, which may be thickened, and sometimes a dural tail is present. These tumors are seen in children and young adults who usually have a long-standing history of epilepsy with or without headaches or other focal neurologic symptoms. PXAs are slow-growing tumors categorized as WHO grade II. (A) Primary central nervous system lymphoma is very rare in children. It would show avid homogeneous enhancement in immunocompetent individuals, but tends to have areas of necrosis and hemorrhage in the immunocompromised. Primary central nervous system lymphoma favors the deep and periventricular white matter and corpus callosum as opposed to the cortical/subcortical location of the tumor in this case. Secondary lymphoma usually is leptomeningeal or dura based, although it rarely may be parenchymal. (C) The mass in the current case is intra-axial. Anteriorly it clearly abuts the white matter directly without intervening cortex. The cyst along the posterior and medial aspect of the mass also is clearly intraparenchymal. This feature rules out a meningioma, which otherwise also can show variable morphology with cystic and hemorrhagic changes and necrosis. Additionally, meningiomas are rare in children except when they are syndromic (e.g., in neurofibromatosis type 2). (D) Dysembryoplastic neuroepithelial tumors (DNETs) constitute another cause of epilepsy in young patients. These tumors are most common in the temporal lobes. They are cortically based, well circumscribed, and usually have a bubbly appearance. In contrast to PXAs, DNETs usually do not enhance, although 20% may have punctate or ring-like contrast-enhancement patterns. (E) The classic pilocytic astrocytoma presents as a cystic mass with an avidly enhancing mural nodule. They rarely occur in a supratentorial location except in adults, in whom they are most common in the cerebral hemispheres. Supratentorial pilocytic astrocytomas in children tend to favor the optic chiasm (particularly in patients with neurofibromatosis type 1) and hypothalamic region. B Level 2 Level 2 evidence consists of randomized clinical trials. (A) Level 1 evidence consists of meta-analyses of multiple level 2 studies. (C) Level 3 evidence consists of quasi-experimental studies (e.g., large observational/cohort studies). (D) Level 4 evidence consists of nonexperimental studies (e.g., small observational studies). (E) Level 5 evidence consists of case reports and narrative literature reviews. Of note, level 6 evidence consists of the opinions of respected authorities. A Malingering/inability to participate in the exam (A–E) Although the patient may have any of these diagnoses, Goldman visual field testing in this patient is inaccurate and unreliable as evidenced by the spiraling result. This indicates that the patient is guessing at what is and is not in his visual field, as patients almost never can indicate consistently and falsely where their visual fields end. D Less than −2.5 Osteoporosis is evaluated by assessment of bone mineral density and reported as a T-score. This value represents the number of standard deviations from normal. Osteoporosis is determined by a T-score of less than −2.5 (meaning that the bone mineral density is less than normal by 2.5 standard deviations). (B) T-scores of −1 to +1 are normal, expected values. (C) A T-score of −1 to −2.5 corresponds to low bone mineral density (osteopenia) without osteoporosis. (E) The definition of osteoporosis is not age dependent, as all individuals are compared to a reference healthy 30-year-old adult of the same sex when it comes to evaluating for osteoporosis. C Extensive intervertebral disk calcification The patient’s clinical presentation and elevated homogentisic acid levels in his urine are diagnostic of alkaptonuria (ochronosis). Widespread calcification involving multiple intervertebral disks may be seen in the spine along with osteoporosis. (A, B) Wedging of at least three adjacent vertebrae associated with thoracic or thoracolumbar kyphosis is a finding seen in Scheuermann disease. (D) H-shaped vertebrae result from infarction and increased pliability of the end plates in patients with sickle cell disease. C Pedunculopontine nucleus The pedunculopontine nucleus is a newer target of deep brain stimulation as it plays a role in the postural instability seen in Parkinson disease that is not addressed well with other stimulation targets. (A) Stimulation of the subthalamic nucleus or globus pallidus internus can relieve the Parkinson disease symptoms of tremor, bradykinesia, and rigidity. (B) Stimulation of the ventralis intermedius nucleus of the thalamus is used for tremor reduction. (D) Stimulation of the globus pallidus internus is often performed for primary dystonias. C Hypoxia/anoxia As shown in the image accompanying the question, the CA1 region of the hippocampus is highly vulnerable to hypoxic insults and subsequent necrosis, whereas the CA3 region and dentate gyrus are more resistant. The CA2 region is the most resistant to hypoxic insults. The hippocampal regions are shown in this image. B Limbic encephalitis Limbic encephalitis (also known as autoimmune limbic encephalitis or paraneoplastic limbic encephalitis) is an autoimmune condition that arises mostly in patients with non–central nervous system tumors. It rarely is limited only to the limbic system and usually extends to other areas of the brain. Clinically, it is almost identical to herpes simplex encephalitis. The most recent system for diagnosis of herpes simplex encephalitis is the Graus and Saiz criteria, all of which need to be met to make the diagnosis: (1) subacute onset (less than 12 weeks of symptoms) of seizures, short-term memory loss, confusion, and psychiatric symptoms; (2) neuropathological or radiological evidence of involvement of the limbic system; (3) exclusion of other possible etiologies of limbic dysfunction; and (4) demonstration of a cancer within 5 years of the diagnosis of neurologic symptoms or the development of classic symptoms of limbic dysfunction in association with a well-characterized paraneoplastic antibody (e.g., antibodies to Hu, Ma2, CV2, amphiphysin, Ri). (A) Herpes simplex encephalitis is indistinguishable clinically from limbic encephalitis; however, cerebrospinal fluid PCR sensitivity has been reported to exceed 98%. In light of the concomitant diagnosis of a lung lesion, limbic encephalitis is more likely. (C) Pontine stroke is more acute in onset and would include dysfunction of the lower cranial nerves. (D) Paraneoplastic cerebellar degeneration is a paraneoplastic syndrome associated with lung, ovarian, and breast cancers as well as with Hodgkin lymphoma. It is a rare condition that occurs in less than 1% of patients with these conditions and usually affects middleaged women. Symptoms include dysarthria; truncal, limb, and gait ataxia; nausea; vomiting; and diplopia. (E) Multiple sclerosis is not associated with psychiatric symptoms, and imaging findings are localized to white matter structures. B Germinal matrix hemorrhage In the images accompanying the question, there are germinal matrix hemorrhages bilaterally seen as echogenic (bright) foci along the inferior aspect of the lateral ventricles on the coronal image (left) and focally expanding the caudothalamic groove on the sagittal image (right). (A) Acute infarction presents as edema in a distinct arterial territory or in a nonarterial distribution (in the case of a venous infarction), which may be accompanied by hemorrhage. (C) Hypoxic-ischemic injury may be seen in ultrasound as increased echogenicity of the deep gray nuclei and brainstem or accentuated gray-white matter distinction peripherally due to edema. (D) Periventricular leukomalacia presents with increased echogenicity in the periventricular regions and more characteristically in the periatrial white matter. D Maxillary division of the trigeminal nerve The maxillary division of the trigeminal nerve passes through the foramen rotundum. E Nicotinic Nicotinic receptors on the target cells are an exception to the rule that adrenergic receptors are the primary postganglionic sympathetic receptors. (A) Muscarinic receptors are the only postganglionic parasympathetic receptors. D C7 to sacrum Global sagittal balance is a reflection of the position of the head in relationship to the pelvis and is most commonly measured on a standing, fulllength lateral scoliosis radiograph by drawing a plumb line that extends from the mid–C7 vertebra to the sacrum. Such a measurement also is known as the sagittal vertical axis and should course anteriorly to the thoracic spine and intersect the L1 vertebra when neutral. A neutral sagittal vertical axis also intersects the posterosuperior corner of the S1 vertebra and, by convention, a spine with a plumb line that falls anterior or posterior to this point (the sagittal vertical axis offset) is said to be in positive or negative balance, respectively. There is no consensus on normal values. Sagittal imbalance may be compensated to a certain extent (depending on the degree of deformity) through mechanisms such as hip or knee flexion or hyperlordosis and hypokyphosis through muscular effort. Children tend to have negative imbalance compared with adults. D Superior oblique myokymia Superior oblique myokymia is a condition with adult onset that manifests as contractions of the superior oblique that are most intense and pronounced when the eye is in the position of the action of the superior oblique (looking downward and medially). Patients describe a shaking of their vision, a feeling of a trembling eye, or tilted vision. The condition often is treated with carbamazepine. (A) Hemifacial spasm is a unilateral spasm/tonic contraction of the muscles innervated by the facial nerve. Although it can be caused by compression of the facial nerve by the anterior inferior cerebellar artery and thus corrected with microvascular decompression, patients often opt for the less invasive botulinum toxin injections into the affected muscles. (B) Duane syndrome is a congenital strabismus with three subtypes. The most common subtype involves an inability to abduct the affected eye due to maldevelopment of the abducens neural pathway. (C) Although patients with myasthenia gravis can present with variable ophthalmoplegia, the unilateral symptoms described and the isolation of the symptoms to action of the superior oblique make superior oblique myokymia more likely. C C C represents the portion of the primary motor cortex most devoted to control of the hand. Due to the many fine motor movements required in the hand, the precentral gyrus tends to be wider in this region as supported by functional MRI studies. (A) A represents the inferior frontal gyrus. (B) B represents the precentral gyrus and primary motor cortex, but an area most likely devoted mostly to control of the facial musculature. (D) D represents the postcentral gyrus and primary somatosensory cortex. (E) E represents part of the supramarginal gyrus. A Conjugate gaze to the right, plegia of right eye adduction, and left eye nystagmus with left gaze The median longitudinal fasciculus (MLF) is the main connection between the nuclei of cranial nerves III, IV, and VI. A lesion in the MLF causes internuclear ophthalmoplegia, and the affected eye shows impaired adduction. The contralateral eye abducts with nystagmus. This leads to horizontal diplopia when looking opposite the affected eye. C Myxopapillary ependymoma This tumor shows the classic presentation of a myxopapillary ependymoma as an avidly enhancing intradural extramedullary mass at the level of the conus medullaris and filum terminale. Although a large mass filling the lumbosacral spinal canal (three or more vertebral segments) is highly suggestive, the imaging appearance is otherwise nonspecific, and other neoplasms such as peripheral nerve sheath tumors and paragangliomas may look similar. Myxopapillary ependymomas tend to be well circumscribed and lobulated, and sometimes show intrinsic T1 hyperintensity presumably due to the presence of mucin or hemorrhage. These tumors rarely can constitute a cause of subarachnoid hemorrhage and superficial siderosis. They are classified as WHO grade I lesions, usually are indolent, and are more common in males with a median age of 35 years at presentation. (A) Schwannomas can be solitary and may be found in this location, where they can mimic a small myxopapillary ependymoma. Both of these tumors can show cystic changes. (B) A solitary leptomeningeal metastasis of this size is a relatively rare presentation, particularly in the absence of systemic disease. Histological features in this case are consistent with a myxopapillary ependymoma. (D) Neurofibromas usually show heterogeneous enhancement. Central hypointensity and peripheral hyperintensity on T2 images (“target sign”) are suggestive of a neurofibroma, although they are not entirely specific. (E) Myxopapillary ependymomas are much more common than paragangliomas in this region; however, both may be indistinguishable by imaging. Histological features in this case are consistent with a myxopapillary ependymoma. C Grade 4 House-Brackmann grading ranges from 1 (normal) to 6 (no movement of the face). Grade 4 is moderate to severe facial weakness with obvious asymmetry. People with grade 4 function are not able to close their eyes fully. (A) Grade 2 is mild dysfunction with slight facial weakness noticeable on close inspection with normal resting tone. (B) Grade 3 is moderate, with obvious but not disfiguring asymmetry with complete eye closure with effort. (D) Grade 5 is severe with barely perceptible facial motion. (E) Grade 6 is complete facial paralysis. C Neurofibromatosis type 1 The lesion shown in the image accompanying the question represents a neurofibroma characterized by a loose arrangement of spindled cells with tapered nuclear ends and scant cytoplasm. Neurofibromas most commonly are associated with neurofibromatosis type 1. (A) Pituitary adenomas are the primary central nervous system manifestation of multiple endocrine neoplasia type 1. (D) Schwannomas are more commonly seen with neurofibromatosis type 2. (E) Subependymal giant cell astrocytomas are the hallmark of tuberous sclerosis. B A larger internal resistance The time constant (Ʈc) is a measure of the amount of time required to change the voltage of the neuron (its potential). A larger time constant favors temporal summation of a signal, as a shorter time constant means that the potential will change more quickly with spatial summation. The equation is as follows: where rm is the neuronal membrane resistance, ri is the internal neuronal resistance, and Cm is the membrane capacitance. A larger intracellular space lowers internal resistance. D Intravenous slow continuous infusion The usual route of administration of vitamin K is oral, which has been shown to be faster than the subcutaneous route in reversing and abnormal INR. The risk of administering vitamin K intravenously is anaphylaxis, and therefore intravenous administration should be limited strictly to patients with life-threatening bleeding. In such cases, administration is not recommended at a rate faster than 1 mg/minute. D 73% The question is asking for the positive predictive value (PPV) of the test which can be calculated using this formula: C Pericellular clearing is an artifact of delayed formalin fixation. The tumor shown in the image accompanying the question is typical for a low-grade oligodendroglioma (WHO grade II). Calcifications are a frequent finding. Like fibrillary astrocytomas, oligodendrogliomas are infiltrative neoplasms. Oligodendrogliomas are either WHO grade II or III lesions. Tumors with necrosis are usually WHO grade III lesions. E Critical carotid artery stenosis with intraluminal thrombus Carotid artery atherosclerosis usually is most severe within 2 cm of the bifurcation and arises opposite to the external and internal carotid artery flow divider. This lateral angiographic view shows near-complete occlusion at the level of the carotid bulb due to an atherosclerotic plaque. There is near-complete critical stenosis (> 99%) with a small amount of contrast material in the proximal internal carotid artery. There is a large, elongated filling defect within the internal carotid artery due to thrombosis. This patient also had thrombosis of the intracranial internal carotid artery, which was seen on the MRI of the brain. (A) Carotid artery dissection usually spares the carotid bulb, occurring 2 to 3 cm above this level. Dissections typically show abrupt tapering of the contrast column, resulting in a “flame-shaped” configuration in the acute phase and also may demonstrate an intimal flap with true and false lumina. (B) Although there is critical stenosis of the internal carotid artery in this case (> 99%), there is no complete occlusion, as there is still some contrast material going through the stenotic bulb and staining the proximal internal carotid artery. (C) The most common type of fibromuscular dysplasia classically presents with a beaded appearance. It can also look corrugated with small diverticula and less commonly may present with long segment stenosis (not the short segment narrowing in this case). Atypical (carotid bulb or septal type) fibromuscular dysplasia can present with a wedge-shaped defect in a nonatheromatous bulb, but this is rare. (D) Although pseudoaneurysms can thrombose due to stagnation of flow, there is no vascular dilatation or outpouching to suggest this. D 4 The described arteriovenous malformation (AVM) is grade 4. AVMs are graded on a scale of 0 to 5. AVMs less than 3 cm score 1 point, AVMs of 3 to 6 cm score 2 points, and AVMs more than 6 cm score 3 points. AVMs in eloquent areas score 1 point (0 points for non-eloquent area involvement), and 1 point is given for deep venous drainage (0 points for superficial drainage). Grading is related to surgical morbidity. A Vagus nerve Although sympathetic input to the kidneys decreases the glomerular filtration rate through vasoconstriction, there are no definitive data to support the idea that parasympathetic activation has the reverse, vasodilatory effect. Renal activity mostly is increased through hormonal mechanisms. The parasympathetic response mainly is concerned with renal inflammatory reflexes. (B, C) The lumbar and thoracic splanchnic nerves provide sympathetic innervations to the kidneys. (D, E) The inferior and superior mesenteric plexuses provide sympathetic innervations to the various abdominal organs. B Haemophilus influenzae Haemophilus influenzae is the most common cause of viral meningitis in nonvaccinated children and is uncommon among vaccinated populations. Neurologic symptoms usually are preceded by gastrointestinal symptoms such as diarrhea. (A) Cryptococcus is a cause of meningitis in immunosuppressed individuals. (C) Neisseria meningitidis is a leading cause of bacterial meningitis. (D) Streptococcus pneumoniae is a leading cause of viral meningitis. (E) Herpes simplex virus usually causes temporal encephalitis. C Sepsis This child has meningitis and ventriculitis complicated by hydrocephalus. In the images accompanying the question, the postcontrast T1-weighted MRI (left) shows marked ventriculomegaly and enhancement of the ependymal surface, consistent with ventriculitis as well as diffuse leptomeningeal enhancement. The diffusion-weighted MRI (right) shows very bright material layering in the occipital horns of the lateral ventricles, which likely represents pus in this context (although blood also can show restricted diffusion). (A) Recurrent nonaccidental trauma potentially can result in ventriculomegaly related to intracranial hemorrhage. It would not explain the presence of layering debris within the occipital horns (unless there is intraventricular hemorrhage), leptomeningitis, or ventriculitis. (B) Congenital aqueductal stenosis can result in variable degrees of obstructive hydrocephalus but would not explain the other findings in this case. (D) A medulloblastoma in the posterior fossa potentially can result in obstructive hydrocephalus and leptomeningeal spread of disease. It would not explain the presence of layering material in the occipital horns unless there is associated hemorrhage or superimposed infection and ventriculitis. A Disruption of the transverse ligament There are three types of C1 fractures: type 1, fracture of a single arch; type 2, burst fracture (Jefferson fracture); type 3, involves the lateral mass(es) of C1. The most important factor for the stability of the atlanto-occipital joint is ligamentous integrity, mostly from the integrity of the transverse ligament. Disruption of the transverse ligament can be determined by MRI or radiograph. Integrity can be determined by the rule of Spence (on an AP radiograph, the total overhang of the C1 lateral masses over C2 should be less than 7 mm, or a ligamentous disruption is likely) and by the atlantodental interval (ADI) (an ADI more than 3 mm in adults and 4 mm in children suggests ligamentous disruption). B Parkinson (infratrochlear) Historically, the Parkinson triangle was accessed to treat carotid-cavernous fistulas. It also contains the abducens nerve. (A) The oculomotor triangle, also known as the medial or Hakuba triangle, contains the oculomotor nerve and the horizontal segment of the internal carotid artery. It is the triangle by which access to most intracavernous aneurysms and tumors is gained. (C) The Glasscock triangle (posterolateral) contains the middle meningeal artery in the floor of the triangle as it exits the foramen spinosum, the horizontal petrous internal carotid artery, and the infratemporal fossa. The triangle is useful as it enables the surgeon to gain proximal control of the internal carotid artery for more distal vascular procedures. Approximately 10 mm of the carotid artery is accessible through this triangle. (D) The Kawase (posteromedial) triangle contains the petrous apex, internal carotid artery, cochlea, and vertebrobasilar junction. It can be used to perform an anterior petrosectomy so that the posterior fossa, anterior brainstem, and root of the trigeminal nerve can be visualized. (E) The porus trigeminus is the entrance to the Meckel cave and is contained within the inferolateral triangle. C Rotatory subluxation with inflammation of the C1/C2 facet capsule Grisel syndrome is seen in pediatric patients often after an upper respiratory tract infection or otolaryngology procedure with subsequent infection/inflammation of the C1/C2 facet joint and/or transverse atlantal ligament causing rotatory subluxation/torticollis. (A) The Power ratio (used to identify atlanto-occipital dislocation) is the ratio of the distance from the basion to opisthion (BC) divided by the distance from the opisthion to anterior arch of the atlas (OA). A ratio of 1 or less is normal, whereas a ratio of more than 1 may indicate atlanto-occipital dislocation. (B) According to the rule of Spence (a method to determine instability of the transverse ligament), an overhang of the C1 lateral masses on C2 of at least 7 mm is abnormal. (D) Baastrup syndrome is described as “kissing” spinous processes, with contact of adjacent spinous processes with enlargement/flattening/sclerosis of apposing interspinous surfaces. (E) Significant anterior cervical “flowing” osteophytes describe Forestier disease, which is characterized by dysphagia or the sensation of a lump in the throat due to compression of the esophagus between osteophytes and the larynx. This condition is part of the spectrum of diffuse idiopathic skeletal hyperostosis (DISH). B Acute left-sided hemiplegia This is an acute, right middle cerebral artery territory infarct. On the images accompanying the question, note the loss of the gray matter–white matter distinction and the blurriness of the right basal ganglia region (left image) compared with the contralateral side where the caudate nucleus head and lentiform nucleus are seen well. Also shown is a hyperdense, right middle cerebral artery due to the presence of clot (right image). (A) Rapid-onset dementia may be seen in Creutzfeldt-Jakob disease (CJD) where the CT often is normal. The MRI in CJD may show increased cortical signal, particularly on diffusion-weighted sequences, with or without involvement of the basal ganglia and thalami. (C) The triad of fever, altered mental status, and nuchal rigidity may be seen in patients with bacterial meningitis; however, the triad is present in only 44% of bacterial meningitis patients. (D) Progressive encephalopathy is a very nonspecific presentation and is not consistent with an acute stroke. A Lateral ventricles The majority (75%) of choroid plexus tumors arise in the lateral ventricles (usually in the atrium). The second most common (30%) location is in the fourth ventricle, which is a more common site of choroid plexus tumors in adults. B Hypokalemia Manifestations of hypokalemia include nausea, vomiting, weakness, muscle cramps, rhabdomyolysis, polyuria, U waves on an electrocardiogram, a prolonged QT interval, and ventricular ectopy. C Hypercalcemia Manifestations of hypercalcemia vary widely and can include polyuria, dehydration, mental status changes, nephrolithiasis, abdominal pain, anorexia, nausea, vomiting, constipation, pancreatitis, confusion, coma, and decreased deep tendon reflexes. D Hypomagnesemia Manifestations of hypomagnesemia include weakness, muscle cramps, irritability, tremors, nystagmus, hallucinations, depression, epileptic fits, and torsade de pointes. A Hyperkalemia Manifestations of hyperkalemia include weakness, nausea, paresthesias, palpitations, peaked T waves on an electrocardiogram, increased PR interval, increased QRS width, and loss of P waves on an electrocardiogram. (E) Manifestations of hypophosphatemia include weakness, mental status changes, white blood cell dysfunction, hemolytic anemia, rhabdomyolysis, and increased pulp chambers in teeth. It often is seen in refeeding syndrome. A Choroid plexus papilloma The images accompanying the question show an avidly enhancing mass with frond-like margins (resembling a cauliflower), most consistent with a choroid plexus papilloma; 80% of these tumors are benign (WHO grade I), and 85% occur before age 5. The most common location is the atrium of the lateral ventricles; in adults, these tumors more frequently occur in the fourth ventricle. Twenty percent have calcifications. (B) Meningiomas are very rare in children unless they are syndromic or in patients with a prior history of radiation. (C) Ependymomas in children are much more common in the fourth ventricle. Half of supratentorial ependymomas are intraventricular, and the rest are parenchymal. Ependymomas are more heterogeneous than choroid plexus tumors and commonly show areas of calcification, cystic change, or hemorrhage. (D) Subependymomas are seen in older patients and are most common in the fourth ventricle. They characteristically do not enhance, although some may show variable degrees of enhancement. (E) Central neurocytomas most commonly occur in patients between 30 and 40 years of age. Their typical location is in a lateral ventricle abutting the septum pellucidum, but they can occur at other sites. They usually are more heterogeneous and do not enhance as avidly when compared with choroid plexus tumors. E Injury to the posterior ligamentous complex Markers for unstable burst fractures include more than 50% loss of height, canal stenosis from retropulsion over 50%, kyphotic angulation of more than 20 degrees, increased interpediculate distance when upright, neurologic deficits, and progressive kyphosis. The Thoracolumbar Injury Classification and Severity (TLICS) score was designed to identify surgical patients. There is heavy emphasis on the integrity of the posterior ligamentous complex, as this often identifies a significant injury and is associated with excessive kyphotic angulation and/or progressive chronic kyphosis. B Bitemporal hemianopsia The condition described is seesaw nystagmus, which can be a manifestation of a hypothalamic lesion, with a craniopharyngioma being the most common cause. Due to the association of these lesions with optic chiasmal involvement, a bitemporal hemianopsia might be present. Of note, the pathophysiology underlying seesaw nystagmus is understood poorly. (A) Loss of peripheral vision is a hallmark symptom of glaucoma. (C) A central scotoma results from such etiologies as nutritional deficiencies and methyl alcohol poisoning. (D) Binasal hemianopsia is rare in that the tracts providing vision in the nasal fields are far lateral and separated from one another. It can, however, be seen in some instances of hydrocephalus and falsely diagnosed in individuals with large, protruding noses. (E) Unilateral inferior hemianopsia is due to pathology involving the superior arcuates. Remember that pathologies in the brain create visual field deficits that tend to respect the vertical midline, whereas pathologies in the eye produce horizontal-respecting deficits. C Intracellular methemoglobin In the early subacute stage, iron atoms are oxidized to the ferric state with resultant formation of methemoglobin, which has five unpaired electrons and is more strongly paramagnetic than deoxyhemoglobin. Because methemoglobin remains confined to the intracellular space, local susceptibility effects persist, and the hematoma appears hypointense on T2 and GRE sequences. The change in the configuration of hemoglobin enables access of water molecules to the iron atoms, and the dipoledipole interactions result in T1 hyperintensity. (A) Freshly extravasated erythrocytes in hyperacute hematomas contain a large proportion of oxyhemoglobin, which has no unpaired electrons and is weakly diamagnetic. Hyperacute hematomas appear isointense on T1- and hyperintense on T2-weighted sequences, sometimes with a hypointense rim on T2 and GRE sequences due to early deoxyhemoglobin formation. (B) Within several hours, acute hematomas show progressive conversion of oxyhemoglobin to deoxyhemoglobin, which proceeds centripetally. Deoxyhemoglobin has four unpaired electrons per iron atom and is strongly paramagnetic. Because deoxyhemoglobin remains restricted to the intracellular compartment, local distortions of the magnetic field lead to signal loss that appears hypointense on T2 and GRE sequences. The three-dimensional configuration of deoxyhemoglobin does not allow access of water molecules to the paramagnetic iron atoms, which prevents the dipole–dipole interactions that would increase T1 signal; therefore, both hyperacute and acute hematomas remain isointense on T1-weighted sequences. (D) In the late subacute stage, the release of methemoglobin into the extracellular compartment removes local susceptibility effects, and the hematoma now appears hyperintense on T2 while remaining hyperintense on T1-weighted images. (E) Hemosiderin in chronic hematomas appears hypointense on both T1- and T2-weighted sequences due to formation of ferritin by phagocytosing macrophages, the excess of which is accumulated as hemosiderin. Both of these substances are superparamagnetic. B Hypertension increases the relative risk by 3.9 to 5.4%. Hypertension is a controversial cause of intracranial hemorrhage (ICH), as both ICH and hypertension are inherently more common with age. The relative risk of developing an ICH is increased by hypertension by 3.9 to 5.4%. (C) Acute surges in blood pressure not related to sympathomimetics or preeclampsia can precipitate ICH. (D) Hypertension is considered primarily a risk factor for the development of a pontine/cerebellar ICH. C TP53 gene mutations TP53 gene mutations are seen more commonly with malignant degradation of low-grade gliomas than with de novo glioblastomas. (A, B) EGFR and PTEN gene amplifications are seen more commonly in glioblastomas arising de novo. (D) There tends to be allelic loss of chromosomes 10q and 19q in secondary glioblastomas. (E) Both primary and secondary glioblastomas show positive staining for GFAP (glial fibrillary acidic protein). C Intertransverse ligament The exiting nerve root (L4) travels caudal to the L4 pedicle and remains intimate with the pedicle as it exits. The nerve root is found deep to the intertransverse ligament, and care must be taken to avoid electrocautery/mechanical injury to the nerve root/dorsal root ganglion at this location. (D) The disk space is anterior and medial to the exiting nerve root. D Cricothyroid (A, B) All intrinsic muscles of the larynx with the exception of the cricothyroid are innervated by the recurrent laryngeal nerve, which is a branch of the vagus nerve. Abduction of the vocal cords is performed solely by the actions of the posterior cricoarytenoid muscles. (C) The stylopharyngeus is innervated by cranial nerve IX. (E) The geniohyoid is innervated by the C1 nerve root via the hypoglossal nerve. B Phosphodiesterase As a second messenger for G-protein signaling, ATP is converted to cAMP by adenyl cyclase. In the cytosol, cAMP then activates protein kinase A that then acts on CREB, which acts as a transcription factor. cAMP is converted to AMP and thus deactivated by phosphodiesterase. (E) Phospholipase C hydrolyzes and cleaves PIP2 to IP3 and DAG in cellular signaling. The products of this reaction then act as second messengers. B Dural sinus thrombosis The “empty delta” sign originally was described on a contrast-enhanced head CT in thrombosis of the superior sagittal sinus. On axial images, the sign results from enhancement around the thrombus filling the superior sagittal sinus, which regularly has a triangular shape. Although there is no consensus on the pathophysiology of the surrounding enhancement, proposed mechanisms include enhancement of peridural and dural venous channels, clot organization, and partial recanalization of the thrombus. A similar appearance can be seen on MRI and in the transverse venous sinuses, where a triangular filling defect also may be seen. (A) Acute arterial thrombosis may present as a hyperdense vessel on a noncontrast CT or as a filling defect on CT, MRI, or conventional angiography. (C) The presence of a focus of enhancement within a parenchymal hematoma (the “spot” sign) is an independent predictor of expansion and poor outcome. (D) The “empty delta” sign is not related to impending herniation. A More antihistaminergic and anticholinergic activity Old antipsychotics often are administered with antihistamine and sedating agents to counteract the expected extrapyramidal side effects. (C, D) The primary mechanism by which antipsychotics are thought to act is by dopamine receptor (D2) blockade. More D2 blockade has been associated with side effects including tardive dyskinesia and neuroleptic malignant syndrome. Increased D2 blockade does not mean increased extrapyramidal side effects, however. The side effects emerge due to a balance between the dopamine antagonizing properties of neuroleptics and their other receptorblocking attributes. (E) The “typical” antipsychotics have more antiserotonergic properties. C 50% B Ventral lateral nucleus The ventral lateral and ventral anterior nuclei receive information from the cerebellum and basal ganglia and project to motor cortex areas. (A) The anterior nuclei group receives afferents from the mammillary bodies and projects to the cingulate gyrus in the Papez circuit. (C) The ventral posterior lateral nucleus receives information from the spinothalamic tracts and projects to sensory cortex areas. (D) The ventral posterior medial nucleus has afferents and efferents connecting to the trigeminal sensory tracts. (E) The medial geniculate body receives signals from the inferior colliculus and projects to the auditory cortex. In contrast, the lateral geniculate body receives signals from retinal ganglion cells and projects to the primary visual cortex. C Nystagmus retractorius Both convergence nystagmus and nystagmus retractorius are associated with Parinaud syndrome. (A) Downbeat nystagmus often is associated with Chiari 1 malformations and cervicomedullary lesions. (B) Seesaw nystagmus is associated with lesions in the diencephalon or chiasmal compression. (D) Abducting nystagmus is associated with lesions in the medial longitudinal fasciculus and occurs in internuclear ophthalmoplegia. D Unstable fracture exacerbated by external stabilization with potential epidural hematoma Although overmedication/oversedation and poor neurologic exams may be causes of a recorded decline in the patient’s condition, patients with ankylosing spondylitis are predisposed to unstable fractures after seemingly trivial trauma. This is in part due to the ossification of ligaments that create long lever arms, limiting the ability to absorb minor impacts. Patients are prone to developing epidural hematomas. An emergent MRI is indicated in this patient for this reason. In addition, fractures often are missed on radiographs, leading to improper treatment. Given the fixed deformities, strapping patients to backboards or inappropriate collars may exacerbate unstable fractures and cause damage to the neural elements. B Lymphoma This is an avidly enhancing solid and infiltrative periventricular mass that partially involves the corpus callosum and fornix, and reportedly has low apparent diffusion coefficient values, indicating restricted diffusion. Note the surrounding edema on the images accompanying the question. The imaging findings are most compatible with lymphoma. Areas of necrosis may be seen in patients with HIV/AIDS. (A) Glioblastoma likely would show areas of necrosis. (C) Tumefactive demyelination characteristically may have an incomplete ring of enhancement. Areas of restricted diffusion sometimes are seen along the leading edge. (D) Infection could present as leptomeningeal disease, cerebritis, or infected fluid collections, which are not present in this case. C Anterior displacement of the ipsilateral ear Positional plagiocephaly can be differentiated from lambdoid craniosynostosis (synostotic plagiocephaly) on physical examination. Lambdoidal synostosis is characterized by ipsilateral occipitoparietal flattening with the ipsilateral ear displaced posteriorly, contralateral parietal bossing, and contralateral frontal bossing. D Sweating The sympathetic nervous system uses postganglionic norepinephrine and epinephrine receptors for end-organ activation or response. The two exceptions are that the adrenal gland and sweat glands are postganglionic and activated by acetylcholine signaling. Although sweating is a sympathetic nervous system response, the postganglionic receptors are muscarinic (bind acetylcholine), just as they are in the parasympathetic nervous system. Because atropine competitively antagonizes muscarinic receptors, sweating decreases after systemic administration of atropine. (A–C, E) These actions are only affected by atropine’s blockade of the parasympathetic nervous system. Sympathetic activity remains constant with atropine administration, in that the autonomic nervous system operates by altering the relative activity of the sympathetic and parasympathetic nervous systems. B Involvement of eloquent brain The MRI studies shown in the images accompanying the question demonstrate a large arteriovenous malformation (AVM) with extensive vascular flow voids throughout the left hemisphere. Management of AVMs is complex, and open microsurgical excision usually offers the best chance for cure in patients with a high risk of hemorrhage. The Spetzler-Martin grading system was introduced to estimate the surgical risk. It allocates points according to the size of the lesion, deep versus superficial venous drainage, and involvement of eloquent brain. Several studies have correlated higher grade lesions on the Spetzler-Martin system with worse surgical outcomes. (A) Deep-seated AVMs have an increased incidence of hemorrhage and a higher surgical risk than those with superficial venous drainage; therefore, these lesions receive a higher score on the Spetzler-Martin grading system. (C) Retrograde cortical venous drainage is associated with an increased risk of hemorrhage in dural arteriovenous fistulas. (D) Venous ectasia results in a sevenfold increase in the risk of hemorrhage in dural arteriovenous fistulas and upgrades the lesions from grade 3 to grade 4 in the Cognard classification. E Fabry disease Fabry disease is a lysosomal storage disease resulting in full-body pain, renal dysfunction, and cardiomyopathy, among other manifestations. (A) Farber disease is an autosomal recessive lysosomal storage disease resulting from a deficiency in ceramidase. Death occurs by age 2. (B) Fragile X syndrome is the most frequent hereditary cause of mental retardation and results from an X-linked dominant inheritance of mutations in the FMR1 gene. (C) Rett syndrome typically results from a new mutation, occurs almost exclusively in females, and is characterized by macrocephaly, developmental delays, hand-wringing difficulties, and scoliosis. (D) Hurler syndrome is an autosomal recessive mucopolysaccharidosis due to a deficiency in αl-iduronidase and is characterized by corneal clouding, dwarfism, and mental retardation. Death occurs at ages 5 to 10 from cardiac arrest. E Granular layer The mnemonic “miles per gallon” can be used to remember the layers of the cerebellum: molecular, Purkinje, and granular. Granule cells (also found in the hippocampus, dorsal cochlear nucleus, olfactory bulb, and cerebral cortex) are the most prevalent type of neuron in the brain. Found in the granular layer, they communicate with the more superficial molecular layer neurons through parallel fibers. (B, D) There are six layers of the cerebral cortex, notably layer 3 (the external pyramidal layer containing the primary source of corticocortical efferents), layer 4 (the internal granular layer receiving afferents from the thalamus), layer 5 (the internal pyramidal layer containing pyramidal neurons and forming the corticospinal tracts), and layer 6 (the multiform layer, which sends efferent fibers to the thalamus). A Antitrust law Antitrust law regulates the conduct of organizations and business to promote fair competition for the benefit of consumers. Under the antitrust laws, hospitals are perceived as business entities offering health care services. In the case discussed in the question, the merger of the two hospitals would create a monopoly of tertiary care services in the local market and can be considered a violation of antitrust law. (B) Stark law (also known as the physician self-referral law) prohibits physicians from referring patients to institutes in which they or a close family member has financial interests. (C) The federal anti-kickback statue prevents physicians from receiving compensation for prescribing or using specific drugs or instruments. (D) The Emergency Medical Treatment and Active Labor Act (EMTALA) governs hospital transfers and what patients are obligated to receive and which patients can be refused treatment. One basic premise is that patients cannot be refused emergency, stabilizing medical care, if it is within the hospital’s ability, simply because of their lack of ability to pay. C There is weakness of foot inversion with an L5 nerve root palsy, which is spared with a CPN palsy. With a common peroneal nerve (CPN) palsy, the posterior tibialis (which enables foot inversion with innervation by the posterior tibial nerve) and gluteus medius (which enables internal hip rotation with innervation by the superior gluteal nerve) are spared. L5 nerve root deficits may include weakness in ankle dorsiflexion (anterior tibialis), foot eversion (peroneus longus/brevis), and foot inversion (tibialis posterior). B 28 The ASIA motor scale awards up to five points per side to motor function at root levels C5 to T1 (biceps, wrist extensors, triceps, grip, and hand intrinsics) and L2 to S1 (iliopsoas, quadriceps, tibialis anterior, extensor hallucis longus, and gastrocnemius), for a total of 50 possible points. This exam has two motor function tests of the C5 root level (deltoid and biceps), of which only the biceps is used. Simply add up the motor grade at each level to obtain a cumulative score. B Indirect revascularization using an encephaloduroarteriosynangiosis procedure An encephaloduroarteriosynangiosis (EDAS) procedure uses a branch of the superficial temporal artery that is laid directly on the surface of the brain without doing a direct anastomosis. Children tend to have better results with this procedure than do adults. (A) Direct revascularization using a superficial temporal artery to middle cerebral artery bypass is effective in adults. (C, D) Conservative and medical therapies result in suboptimal stroke prevention. C Glioblastoma The vascular proliferative changes seen in the background of irregularly shaped astrocytic cells is most consistent with a glioblastoma diagnosis. Vascular proliferative changes represent a proliferation of cells that normally constitute blood vessel walls (endothelial cells, smooth muscle cells, pericytes, and fibroblasts). The significance of this finding depends on the tumor type. In a pilocytic astrocytoma, there may be vascular proliferative changes that do not have the same implication in terms of grade as they do in a fibrillary astrocytoma. C Third degree The Seddon and Sunderland classification systems are the most commonly used classification schemes for peripheral nerve injuries. A third-degree injury is an interruption of the endoneurium. (A) A Sunderland first-degree injury (Seddon neurapraxia) is a physiological transection with the nerve and basement membrane intact. (B) A second-degree injury (Seddon axonotmesis) is an interruption of the axons and myelin with intact supporting structures. (D) A fourth-degree injury is an interruption of the endoneurium and perineurium. (E) A fifth-degree injury (Seddon neurotmesis) is a completely severed nerve. (A sixth-degree injury is a mixed lesion.) A FDG uptake Rapid growth on serial imaging, areas of induration on clinical exam, and persistent pain are features that raise concern about malignant transformation of a plexiform neurofibroma, which can show increased FDG uptake. (B) Both benign and malignant peripheral nerve sheath tumors may show heterogeneous enhancement. (C) The “target” sign classically is seen on T2 images in neurofibromas and is related to a fibrocollagenous core. It sometimes can be seen in schwannomas and usually is not seen in malignant peripheral nerve sheath tumors. (D) Benign plexiform neurofibromas tend to grow slowly. B Left lateral medulla Wallenberg syndrome (lateral medullary syndrome) often is attributable to vertebral artery occlusion, although classically the condition is described secondary to a posterior inferior cerebellar artery infarction. The lateral medulla essentially is the only location at which a stroke will cause an ipsilateral sensory loss in the face and a contralateral sensory loss in the body without weakness. There often are no changes in sensorium. (A) A right anterior medulla stroke (medial medullary syndrome or Dejerine syndrome) would cause deviation of the tongue to the right side, contralateral limb weakness, and loss of proprioception/vibration on the contralateral side due to occlusion of the spinal artery near its vertebral origin. (D) A stroke in the ventrocaudal pons will lead to Millard-Gubler syndrome, causing contralateral weakness, ipsilateral lateral gaze weakness, and ipsilateral whole face weakness. The deficits can be remembered by noting that there are six letters in “Gubler” and seven letters in “Millard,” indicating the palsies of cranial nerves VI and VII along with the contralateral weakness. C Presence of a lucid interval Of patients with an epidural hematoma, 10 to 27% experience the classic presentation of a brief loss of consciousness followed by a lucid interval, with further progression to obtundation, hemiparesis, and a dilated pupil. This symptom progression also can be observed with intraparenchymal and subdural hemorrhages. Eighty-five percent of epidural hematomas are due to arterial bleeding, and most often are secondary to injury to the middle meningeal artery. Skull fractures are seen in 40% of epidural hematomas, and CT scans show a lenticular shape of the hemorrhage in 84% of cases due to restrictions from the cranial sutures. Indications for surgery may include a hemorrhage volume more than 30 mL or thickness more than 15 mm, midline shift more than 5 mm, Glasgow Coma Scale score of 8 or less, and focal neurologic deficits (e.g., anisocoria). D Ligation of the anterior choroidal artery Surgical ligation of the anterior choroidal artery was an early procedure for Parkinson disease. It classically produces a “triple H” syndrome of hemianesthesia, hemiparesis, and a homonymous hemianopsia. B Nerve root enhancement Enhancement of intradural nerve roots can be seen in preganglionic injuries and may indicate functional discontinuity even in the presence of a normal-appearing nerve. (A) Pseudomeningoceles (not true meningoceles) occur in more than 80% of patients with traumatic avulsion of the brachial plexus. Pseudomeningoceles may develop within the spinal canal, where they exert variable degrees of mass effect or track along the course of the nerve roots. (C) Presence of fluid within the root sleeve does not necessarily reflect avulsion injury; however, pooling of fluid and abrupt interruption of the root sleeve are findings indicative of an avulsion injury. (D) A spinal cord hematoma may be seen in the setting of trauma but does not necessarily reflect avulsion injury. Focal edema may be seen in the spinal cord at the site of the avulsion. B Beta activity over temporal areas The periodic discharges seen with herpes encephalitis typically occur over the temporal regions. Slow waves, rather than sharp waves, may be evident over the temporal lobes in many patients with severe disease. Seizures occur early in the course of herpes encephalitis, and electroencephalographic recordings can be very disrupted. (E) Periodic sharp wave complexes are seen in Creutzfeldt-Jakob disease. B Arachnoid cyst Arachnoid cysts are lined by arachnoid cells, resulting in accumulation of cerebrospinal fluid. They are extra-axial and displace the brain parenchyma away from the calvaria. The displaced cortex in this case can be seen on both T2 and FLAIR sequence images. Arachnoid cysts follow cerebrospinal fluid signal on all sequences and, therefore, suppress on FLAIR, although they may show pulsation artifacts, as in this case, particularly when they are large. Arachnoid cysts do not show contrast enhancement, and most do not grow but sometimes can enlarge. They can result in mass effect and scalloping/thinning of the inner table of the calvaria (as seen on the T2 image accompanying the question). If symptomatic, arachnoid cysts can be shunted, fenestrated/marsupialized, or resected. (A) Porencephalic cysts are intra-axial (not extraaxial as in this case), and usually present as a cavity filled with cerebrospinal fluid; therefore, they also follow cerebrospinal fluid signal on all sequences and do not enhance. They typically are surrounded by dysplastic white matter (compared with the displaced cerebral cortex in this case). (C) Neurenteric cysts are lined by endodermal epithelium. The great majority of these cysts are extra-axial, but in rare cases can be intra-axial. They do not communicate freely with the subarachnoid space; therefore, they do not necessarily follow cerebrospinal fluid signal. They usually show variable signal intensities, depending on the degree of proteinaceous contents. (D) Schizencephaly is a neuronal migration disorder resulting in a cleft extending from the ventricular (ependymal) surface to the cortical (pial) surface. The cleft is lined with dysplastic gray matter and may be filled with cerebrospinal fluid. D Hyperphosphorylated tau protein The image accompanying the question shows a neuron with a neurofibrillary tangle (NFT). NFTs are intracytoplasmic aggregates of hyperphosphorylated tau protein that can be found in various neurodegenerative processes, the most common being Alzheimer disease. E Striae medullaris thalami The striae medullaris thalami connect the anterior thalamic and septal nuclei to the habenula. The inferior layer of the tela choroidea attaches to the striae medullaris thalami and forms the floor of the velum interpositum. (C) The internal medullary lamina runs longitudinally through the thalamus, separating the medial and lateral nuclear masses. (D) The thalamic fasciculus joins the ansa lenticularis and lenticular fasciculus with the basal ganglia and the ventral lateral nucleus of the thalamus. A Lack of weakness in the deltoid and latissimus dorsi The radial and axillary nerves are terminal branches of the posterior cord. Lack of weakness in the deltoid (axillary nerve innervated) and latissimus dorsi (thoracodorsal nerve) indicates injury to the radial nerve and not the posterior cord in the presence of a wrist drop. (B) The long thoracic nerve innervates the serratus anterior and originates from the roots of C5 through C7. (C) The rhomboids are innervated by the dorsal scapular nerve, which originates from the C4 and C5 nerve roots before they form the superior trunk. (D) The medial antebrachial cutaneous nerve is derived from the C8 and T1 nerve roots and branches from medial cord. (E) Brachioradialis involvement would occur in a radial nerve injury, but this finding alone does not rule out a posterior cord injury. C Associated with atlantoaxial subluxation Periodontoid panniculi can be seen in the setting of various etiologies, including rheumatoid arthritis, calcium pyrophosphate deposition disease, and psoriatic arthritis. They frequently are associated with atlantoaxial subluxation, and it is thought that chronic craniocervical instability may play a role in their development. (A) Various reports have shown periodontoid panniculi to resolve gradually after posterior stabilization without actual tissue resection. (B) Chordomas arise from notochordal elements. Although they can occur at the tip of the clivus, they usually are very bright on T2 sequences. (D) Meningiomas arise from arachnoid cap cells. The lesion in this case is periodontoid rather than dural based. A Amoebiasis The organisms shown in the image accompanying the question morphologically are consistent with amoeba. Naegleria often is associated with primary amoebic encephalitis classically presenting in patients exposed to contaminated water. Acanthamoeba and Balamuthia can cause granulomatous amoebic encephalitis often in immunocompromised individuals. B Herpes simplex Herpes simplex causes temporal encephalitis and temporal epileptiform discharge on electroencephalogram. C Cryptococcus Central nervous system Cryptococcus infection can manifest with multiple focal mass lesions called cryptococcomas. The opening pressure during a lumbar puncture is high, cryptococcal antigen titer is positive, and cerebrospinal fluid India ink staining is also positive with this condition, which is common in patients with HIV. Treatment is with amphotericin B and flucytosine. A Tenia solium Tenia solium is a tapeworm found in pigs that causes neurocysticercosis. Symptoms include seizures, decreased vision, papilledema, and parkinsonism. Although the pork supply in the United States is free of the organism, pork in Central and South America may be colonized. (D) Toxoplasmosis is one of the most common neurologic complications of AIDS. Patients present with fever, headaches, seizures, and possibly focal neurologic deficits. Multiple ring-enhancing lesions are seen in 70% of patients with toxoplasmosis. Distinguishing toxoplasmosis from lymphoma can be difficult, but a trial of antitoxoplasmosis medications for two weeks can confirm the diagnosis. (E) West Nile virus causes poliomyelitis and meningitis, with poliomyelitis being the more common manifestation. Patients typically have fever, myalgias, and encephalopathy, along with asymmetric weakness that quickly can progress to quadriplegia. Cerebrospinal fluid studies show pleocytosis and elevated protein. (F) JC virus leads to progressive multifocal leukoencephalopathy (PML). This fatal disease has no effective treatment. Symptoms develop over several weeks, and include clumsiness, progressive weakness, and visual, speech, and personality changes. Characteristic imaging findings include multifocal hypointense T1 and hyperintense T2 lesions. B Ependymoma The tumor cells form perivascular pseudorosettes, a classic feature of ependymoma. Perivascular pseudorosettes are formed by the perivascular arrangement of tumor cells with an intervening fibrillary-rich, acellular area. D Sexual dysfunction The incidence of sexual dysfunction is reported to occur in 0.4 to 20%, whereas retrograde ejaculation occurs in 5 to 22% of patients undergoing an anterior lumbar interbody fusion (ALIF) procedure. These injuries are assumed to be due to injury to the bilateral sympathetic chains contributing to the superior hypogastric plexus. Of note, ureteral injuries, deep venous thrombosis, hernias, and lumbar sympathetic dysfunction may be more common with ALIF procedures. Other complication rates are similar between ALIF and extreme lateral interbody fusion (XLIF) procedures. (A) Vascular injuries are seen in 0.5 to 15% (average 6.6%) of patients undergoing an ALIF procedure. (B) Neurologic injuries are seen in 5% of patients undergoing an ALIF procedure. In contrast, transient neurologic complaints can occur in up to 25% of patients undergoing an XLIF. C Surgical decompression The CT scan shows tension pneumocephalus with a large amount of air underlying a left craniotomy. There is resultant mass effect on the brain, shift of midline structures, and entrapment with early dilatation of the contralateral lateral ventricle. Tension pneumocephalus is a surgical emergency. Treatment includes surgical decompression and administration of 100% oxygen. (A) A lumbar puncture would be contraindicated in an acute herniation syndrome. (B) Hypertonic saline solutions are sometimes used in the treatment of cerebral edema and may lower increased intracranial pressures acutely. (D) Mannitol is a widely used osmotic diuretic that decreases cerebral edema and intracranial pressures by reducing water content in cerebral tissue. C After the peak of sodium conductance but before hyperpolarization Potassium conductance peaks as some voltage-gated potassium channels begin to close at the peak of depolarization of the action potential (after sodium conductance peaks). (A) Before the peak of sodium conductance, the conductance of both sodium and potassium is increasing, with the former increasing at a greater rate. (B) During the peak of sodium conductance, the potassium conductance still is increasing. (D, E) Potassium conductance decreases throughout the remainder of the action potential through the hyperpolarization phase. C Miller Fisher syndrome The patient has Miller Fisher syndrome, a variant of Guillain-Barré syndrome. It is characterized by the triad of areflexia, ataxia (usually without limb weakness), and ophthalmoplegia, and can occur with ascending facial diplegia. The condition is more common in middle-aged men and often follows a viral illness. (A) Although all of the symptoms fit with multiple sclerosis, the most likely diagnosis given the patient’s symptoms and presentation is Miller Fisher syndrome. (B) A cerebellar stroke can result in an ataxic gait, but the other symptoms cited are not typical. (D) Diplopia and ataxia can be seen in ethanol intoxication, but it does not explain the facial diplegia. (E) Myasthenia gravis is characterized by muscle fatigue, which may manifest in ophthalmoplegia and facial weakness. In severe forms, there may be general muscle weakness (not found on the physical exam), resulting in an ataxic gait, but the mention of a recent viral illness makes Miller Fisher much more likely. C Somatosensory evoked potential Somatosensory evoked potentials (SSEPs) in the upper extremities measure impulses in the posterior columns, whereas in the lower extremities, SSEPs are carried by the dorsolateral fasciculi, which receive their blood supply from the anterior spinal artery. (A) Motor evoked potentials are performed by stimulating the motor cortex and recording responses in the peripheral musculature. (E) Electromyography involves three phases of testing: insertional activity, spontaneous activity, and volitional activity as recorded by needle electrodes. D Shunt externalization Shunt externalization at the chest or neck level should be the next step to allow resolution of the pseudocyst while monitoring cerebrospinal fluid content and cultures for a possible shunt infection and the need for complete shunt removal. D Neurohypophysis The tissue shown in the image accompanying the question represents neurohypophyseal tissue. The occasional round eosinophilic bodies represent Herring bodies. B Type 2 Modic type 2 and 3 changes are chronic changes. A Modic type 2 change shows high signal on T1 and iso- to hyperintensity on T2, and is thought to be due to replacement of bone marrow by fat. (A) A Modic type 1 change is associated with hypointense T1 and hyperintense T2 signals, and is thought to represent bone marrow edema from acute/subacute inflammation. (C) A Modic type 3 change is hypointense on T1 and T2 sequences due to reactive osteosclerosis. (D) There are no Modic type 4 changes. A Provides special visceral efferent fibers to the stylopharyngeus and the laryngeal, pharyngeal, and palatine musculature (B) Special visceral afferent fibers from the posterior one third of the tongue are derived from the solitary nucleus. (C) General visceral efferent fibers to the otic ganglion arise from the inferior salivatory nucleus. (D) General visceral efferent fibers going through the greater superficial petrosal nerve are derived from the superior salivatory nucleus. (E) Special visceral efferent fibers to the stylohyoid, stapedius, and posterior belly of the digastric originate in the facial motor nucleus. B The results are not clinically significant. (A–E) All of the answer choices are potential issues with the study, but only one error is obvious from the information given. Researchers often confuse clinical and statistical significance. Although statistical significance means that there is an actual mathematical difference between two groups, clinical significance determines if this difference has meaningful clinical applications. In the example study, 2 weeks of extended life is clinically insignificant when electrodes last for decades. The authors’ conclusion thus has little clinical applicability. D Shortens
Section 1

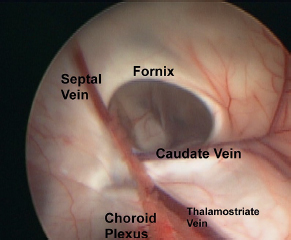


Section 2



Section 3

![]()
Stay updated, free articles. Join our Telegram channel







Full access? Get Clinical Tree


