9 Primary CNS Lymphoma
Introduction
Primary CNS lymphomas (PCNSL) are extranodal malignant lymphomas arising within the brain, eyes, leptomeninges, or spinal cord in the absence of systemic lymphoma at the time of diagnosis. The incidence of PCNSL in western countries is 5 per 1 million person-years. Currently PCNSL are estimated to account for up to 1% of non-Hodgkin lymphomas (NHL) and 3% to 5% of all primary brain tumors. After a continual increase over the past two decades,1 epidemiologic data suggest a recent decrease in the incidence of PCNSL, particularly among young patients suffering from acquired immunodeficiency syndrome, and probably associated with the development of new active antiviral drugs. In contrast, the incidence remains high among older patients (over 60 years), most of whom are immunocompetent.2 The reason for the rising incidence of PCNSL among the immunocompetent population is obscure. PCNSL is also of interest because it is one of the only primary malignant brain tumors whose prognosis has improved considerably over the past two decades due to advances in treatment strategy. Although the prognosis remains poor for the majority of the patients, a substantial minority, representing approximately 20% to 30% of cases, can hope to be cured. Because long-term survivors are at increased risk of developing severe delayed cognitive dysfunction, future treatment should be aimed at improving the efficacy of treatment while limiting the risk of neurotoxicity. This review focuses on PCNSL in the immunocompetent population.
Pathology and Pathogenesis
In immunocompetent patients, all but 5% of PCNSLs are diffuse large B-cell lymphomas (DLBCL).3 Since they are morphologically indistinguishable from systemic DLBCL, the WHO classification of tumors of hematopoietic and lymphoid tissues does not recognize PCNSL as a separate entity.4 The remaining cases of PCNSL are T-cell lymphomas (2% to 5%)5 or, in rare instances, low-grade B-cell lymphomas of the lymphoplasmocytic (Waldenström macroglobulinemia), fol-licular, or mucosa-associated lymphoid tissue (MALT) type.6 Little is known about the tumorigenesis of PCNSL. In contrast to immunocompromised patients, the Epstein-Barr virus (EBV) does not appear to be involved in the pathogenesis of PCNSL in immunocompetent patients. The site of origin of lymphoma cells, the biological mechanisms involved in the neoplastic transformation of the lymphoid cells, and their intriguing confinement within the CNS during the course of the disease have yet to be elucidated. Indeed, the CNS does not contain resident lymphocytes under normal circumstances and lacks lymphatic vessels. However, recent evidence suggests that T and B cells enter the CNS under physiological conditions, and it has been hypothesized that PCNSL may originate from B cells derived from systemic lymphoid tissues and normally trafficking in and out of the CNS.7 PCNSL could derive from a benign CNS inflammatory process through a monoclonal proliferation of B cells. Another hypothesis is that PCNSL might represent the metastasis of an occult systemic lymphoma, eradicated by an intact immune system but escaping within the immune-privileged CNS. Analysis of clonally rearranged immunoglobulin heavy chain (IgH) genes revealed identical dominant PCR products in bone marrow aspirates, blood samples and tumor specimens from some PCNSL patients, suggesting that subclinical systemic disease can be detected at initial diagnosis, which supports a systemic origin of the tumor in these cases.8 In addition, B cell tropism for CNS might be acquired (before or after the oncogenic events) through specific interactions between selective homing receptors and their ligands expressed on CNS endothelial cells, as suggested by the distinctive angiotropism of CNS lymphoma cells.9,10
It also remains unclear whether the dismal outcome of PCNSL compared to systemic DLBCL is attributable to the immune-privileged cerebral location or reflects a specific aggressive intrinsic biologic behavior. Recently, expression profiling and genomic screening have provided new insights into understanding the poor prognosis of PCNSL. Based on lymphochip cDNA microarrays, two distinct gene expression profiles have been identified among systemic DLBCLs, indicative of different stages of B-cell differentiation. One subgroup expressed genes characteristic of germinal center B cells (GCB subgroup) whereas the other expressed genes normally induced during in vitro activation of peripheral blood B cells (ABC subgroup). Interestingly, patients with the GCB signature had a significantly better outcome than those with the ABC profile.11 PCNSLs have been shown to frequently expresses BCL612 and to carry an extremely high load of somatic mutations of immunoglobulin genes and in several oncogenes demonstrating aberrant ongoing hypermutation.13–15 Since such an ongoing hypermutation and BCL6 expression are considered as germinal center markers, it has been postulated that the cell of origin of PCNSL passed through the GC microenvironment and that these neoplasms correspond to the GCB subgroup as defined for DLBCL. However, recent immunoprofiling16 and gene expression studies using cDNA microarrays17,18 demonstrated that PCNSL may exhibit characteristics associated with both ABC and GCB subtypes. Thus, PCNSL may correspond to an overlapping B-cell differentiation time slot, i.e., late GC/early post-GC stage.
Pangenomic analyses of chromosomal imbalances by comparative genomic hybridization (CGH) have shown frequent chromosome 6 q loss (60% to 75%) in PCNSL.19–21 Nakamura et al.22 refined the candidate region suspected to contain a lymphoma-related tumor suppressor gene in the 6q22–23 locus by a fine LOH deletion mapping of 6 q in PCNSL. The PTPRK gene seems a relevant candidate gene, since it is involved in the regulation of cell contact and adhesion, and a loss of protein expression was observed in most (76%) of the PCNSLs tested. It belongs to the protein tyrosine phosphatase superfamily of enzymes. Further studies to identify gene mutations and/or rearrangements are needed to ascertain the involvement of PTPRK in PCNSL tumorigenesis. Interestingly, the authors showed that chromosome 6 q loss was found at a significantly higher rate in PCNSL than in systemic DLBCL and was correlated with shorter survival.22 An independent study of 75 newly diagnosed HIV-negative PCNSLs investigated by interphase FISH analysis has confirmed the frequent 6q22 chromosome deletion, with a prevalence of 45%, and its negative impact on overall survival.23 Chromosome 6 q loss would therefore represent a prognostic marker in PCNSL. Otherwise, the BCL6 gene has been found mutated and its chromosomal locus (3q27) recurrently involved by translocations (20%), suggesting that BCL6 activation through genomic rearrangements may play a role in PCNSL pathogenesis.23–25 BCL6 is frequently expressed in PCNSL, but there are conflicting data on its prognostic value as an immunohistochemical marker.16,26–29 These results provide evidence for an alternative pathogenesis in PCNSL compared to DLBCL explaining, in part, differences in clinical behavior and prognosis.
Diagnosis and Workup
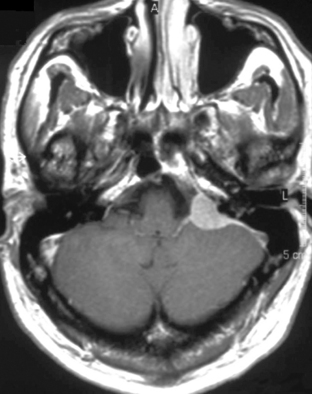
The clinical presentation of PCNSL includes focal symptoms and raised intracranial pressure. Changes in behavior and personality as well as confusion frequently occur in the elderly. The deep location of PCNSL explains why seizures are less frequent than in other brain tumors.30,31 CT scans and MRI typically show solitary (two thirds of cases) or multiple (one third of cases) periventricular, homogeneously-enhancing lesions (Figures 9-1 and 9-2).32–34 PCNSL is potentially associated with a large spectrum of radiological presentations and can simulate inflammatory (sarcoidosis, multiple sclerosis) or postinfectious diseases (ADEM) or other brain tumors (meningiomas, malignant gliomas, gliomatosis cerebri, brain metastases).35–37 The diagnosis may be difficult to establish, especially with the presence of nonenhancing infiltrating lesions (occurring in about 10% of cases) (Figure 9-3),38,39 or dural-based masses (Figure 9-4)40,41; perfusion MRI shows a much lower relative cerebral blood volume than that seen in malignant gliomas, and distinct signal-time intensity curves reflecting rapid leakage of contrast medium into the interstitial space.42 Similarly magnetic resonance spectroscopy at short echo times show massive elevations of lipid resonances in PCNSL, not usually seen in high-grade gliomas.43,44 Steroid-induced response, observed in approximately 40% of cases, is classic but not the rule and should not be used as a diagnostic test since it may prevent a pathological confirmation of the diagnosis. Rarely, spontaneous disappearance of lesions has been reported, hence the term “ghost tumors.”45,46 Ring enhancement, frequently seen in immunodeficient patients, is a pattern rarely seen in immunocompetent patients. However, none of these signs are specific, and diagnosis relies on the pathological study of a tumor sample. Cerebral biopsy can be avoided when lymphomatous cells are discovered in the cerebrospinal fluid (10% to 30% of patients) or in a vitreous-body biopsy (uveitis, sometimes asymptomatic, is present in 10% to 20% of cases at diagnosis). The current recommended staging evaluation for PCNSL includes body CT scans and bone marrow biopsy.47 In fact, systemic involvement is so rare at onset that extensive staging is not recommended by some authors, the only required examinations being HIV testing, chest radiography, analysis of cerebrospinal fluid, ocular slit-lamp examination, and a careful clinical assessment. However, in a recent retrospective study, 7% of patients were found to have systemic NHL by staging FDG body PET when body CT scans and bone marrow biopsies were negative.48 This higher incidence of systemic lymphoma than reported in prior series suggests that occult lymphoma may be more common than recognized previously. These findings warrant prospective validation, since the identification of a systemic site of the lymphoma has important implications in the management of PCNSL.
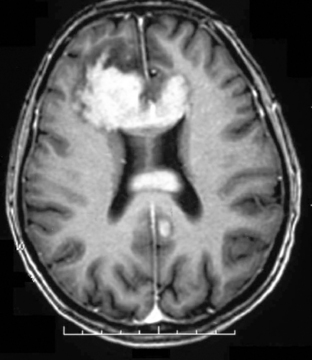
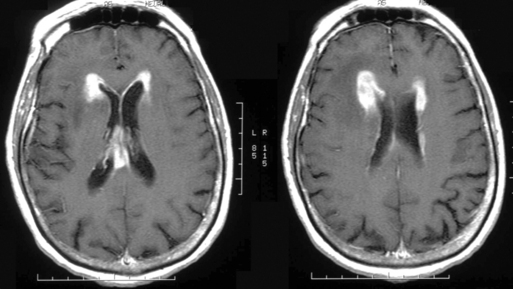
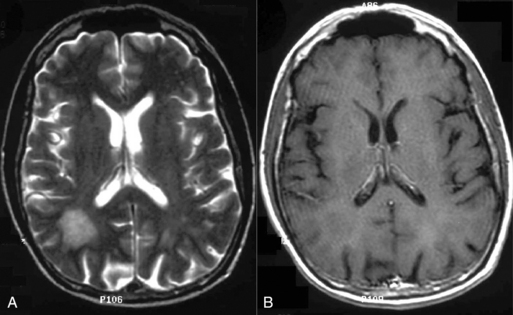
Figure 9-3 A, MRI T2-weighted sequence. B, T1-weighted sequence with gadolinium: Non enhancing PCNSL.
Treatment Options
TREATMENT OF NEWLY DIAGNOSED PCNSL
Age and performance status are the main independent prognostic factors consistently identified in a large number of studies.49–51 As PCNSL is a highly radiosensitive and chemosensitive infiltrative tumor, surgery is therefore restricted to diagnostic biopsy. Although the tumor appears on MRI as a unique contrast-enhancing lesion in the majority of the immunocompetent patients, whole-brain radiotherapy (WBRT) is recommended based on the microscopically diffuse nature of PCNSL. Despite a high rate of response, RT alone has shown a limited survival benefit in PCNSL with a median overall survival (OS) duration of 10 to 18 months and a 5-year survival rate of less than 5%.52 The only phase II trial of radiotherapy (conducted by the RTOG) delivered a total dose of 40 Gy with an additional 20-Gy boost to contrast-enhancing lesions and reported an overall survival of 11.6 months.53 Interestingly, most of the relapses occurred in sites that had received the maximum RT dose. These disappointing results have led to the use of chemotherapy in combination with WBRT. Since the 1990s, numerous convergent phase II studies have shown that the addition of high-dose methotrexate (MTX)-based chemotherapy to RT substantially improves survival compared with RT alone (median survival: 2 to 4 years; 5-year survival rate: 20% to 40%).54–69 In contrast, adding the CHOP regimen (standard chemotherapy for systemic lymphoma) to RT did not appear to improve survival compared with RT alone. This may reflect the poor central nervous system penetration of the chemotherapy agents included in these regimens. The optimal dose of irradiation postchemotherapy has never been prospectively investigated. Doses between 20 and 50 Gy to the whole brain (WB) with or without a tumor bed boost are currently used, with most of the protocols using a total dose of 40-45 Gys without a boost. For patients who achieve a complete response after high-dose MTX-based chemotherapy, it still remains unclear whether consolidation with WBRT improves disease control or survival. A subset analysis from a phase II trial that included 25 patients aged less than 60 years who achieved CR after initial chemotherapy and received either 45 Gy or 30.6 Gy as consolidation treatment showed a significantly higher recurrence and lower overall survival rate in the reduced dose RT group.61 Other studies did not share this observation. In two multicenter retrospective analyses, no differences were noted regarding disease-free or overall survival between patients in CR receiving WBRT as consolidation treatment or at the time of relapse.70,71 In the Memorial Sloan Kettering Cancer Center (MSKCC) experience, consolidation treatment with WBRT improved failure-free survival but not overall survival in complete-responding patients after MTX-based therapy, but increased the rates of neurotoxicity.72
In order to reduce neurotoxicity, several groups have explored the efficacy of various high-dose MTX-based chemotherapy regimens as initial treatment for newly diagnosed PCNSL. These studies converge to suggest that chemotherapy alone and deferred radiotherapy strategy allows comparable results in terms of survival to those reported for combined chemoradiotherapy, with better neurocognitive and quality of life outcomes.73–79 This supports the comparison of these approaches in a prospective randomized trial. While high-dose MTX is undoubtedly a key drug for PCNSL chemotherapy, interest in adding other agents to MTX exists in the scientific community. Two prospective phase II trials have investigated the efficacy of high-dose MTX (8 g/m2) as a single drug therapy,77,78 and similarly demonstrated a clearly shorter PFS (13 months) than that achieved with a polychemotherapy regimen. This suggests that other cytotoxic agents should be used with high-dose MTX in a chemotherapy-alone approach. However the optimal combination remains to be established. Alkylating agents able to effectively penetrate the CNS would be preferred. Concerning the optimal “high dose” of MTX to deliver, although there is no clear evidence of a dose response, a dose of greater than 3 g/m2 in a rapid infusion is recommended.80 In addition, this dose generally yields cytotoxic levels in the cerebral spinal fluid, thus theoretically avoiding the need to administer intrathecal chemotherapy for leptomeningeal coverage. In practice, when intravenous high dose MTX (>3 g/m2) is used, several authors recommend adding intrathecal CT only in cases of positive CSF cytology and withholding it in the absence of detectable subarachnoid disease.81
DELAYED NEUROTOXICITY
WBRT, high-dose MTX chemotherapy, and the combination of both treatments expose the patients to delayed neurotoxicity. This complication can occur as early as 3 months after the treatment and is characterized by attention deficit, memory impairment, ataxia, and urinary incontinence, potentially ultimately leading to dementia. Imaging shows confluent diffuse white matter changes and later cortical-subcortical atrophy. The physiopathology of this complication remains poorly understood; loss of oligodendrocyte progenitors and oxidative stress have been suggested as potential mechanisms. Lai et al.82 reported a well-documented series of five autopsied cases who died of treatment-related leukoencephalopathy. All had combined treatment and were in tumor remission. In addition to white matter rarefaction and spongiosis, fibrotic thickening of small vessels in the deep white matter and atherosclerosis of intracranial large vessels were systematically found, suggesting that a vascular process may be also an important component of this white matter injury. The risk of neurotoxicity increases sharply with patient age. In the elderly population (patients over age 60), virtually all long-term survivors will develop delayed neurotoxicity with its devastating consequences on quality of life and mortality.83 In the younger population (patients under age 60), the exact incidence of this complication is more difficult to determine. Cognitive dysfunctions are usually less severe and occur later than in the elderly population, although they may interfere with quality of life.64 An update of the MSKCC experience providing long-term data (median follow-up of 115 months) reported a 26% rate of neurotoxicity in surviving patients younger than 60 years (versus 75% in the elderly).68 However, this should be regarded as a minimum estimate in the absence of a psychometric evaluation. A series of 19 consecutive young patients (median age: 44 years) treated in a European clinical trial and in complete remission for a mean time of 24 months after combined therapy were investigated by an extensive neuropsychological evaluation.84 Cognitive impairments were found in 63% of patients (including 21% with severe cognitive deficits); only 42% of the patients had resumed work, and 67% had white matter abnormalities and cortical atrophy detectable by MRI. Although this study suffers from the absence of available baseline data at the completion of the treatment to assess the potential contribution of the tumor to cognitive dysfunction, it suggests that the incidence of delayed neurotoxicity after combined therapy is largely underestimated in young patients, albeit less severe than in the elderly. These results contrast sharply with a prospective neuropsychological study performed by Fliessbach et al.84 in a series of 23 patients successfully treated with a high-dose MTX-based chemotherapy without radiotherapy. Comparison between baseline evaluation at completion of the treatment and at the last follow-up (median: 44 months) showed a good preservation of cognitive functions, although one third of the patients demonstrated some degree of white matter changes at the MRI. This latter point confirmed some previously published reports showing that MTX-related leukoencephalopathy is a frequent but not necessarily universal accompaniment to deterioration of cognitive performance.86 The significantly better preservation of neurocognitive functions and quality of life observed in patients treated with chemotherapy alone as compared with those who received combined treatment was also supported by Correa et al.87 in a retrospective comparative neuropsychometric analysis of 28 patients from a single institution. The incorporation of systematic psychometric and quality of life evaluations with an appropriate standardized test battery is recommended for all future prospective trials.88 Interestingly, some functional polymorphisms interfering with the methionine metabolism might influence MTX neurotoxicity.89,90
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


