Lateral view (left) and posterior view (right) of the spine. The cervical, thoracic, and lumbar vertebrae are separated by a cartilaginous disc that provides cushioning and allows for movement. The sacral and coccygeal vertebrae are already fused
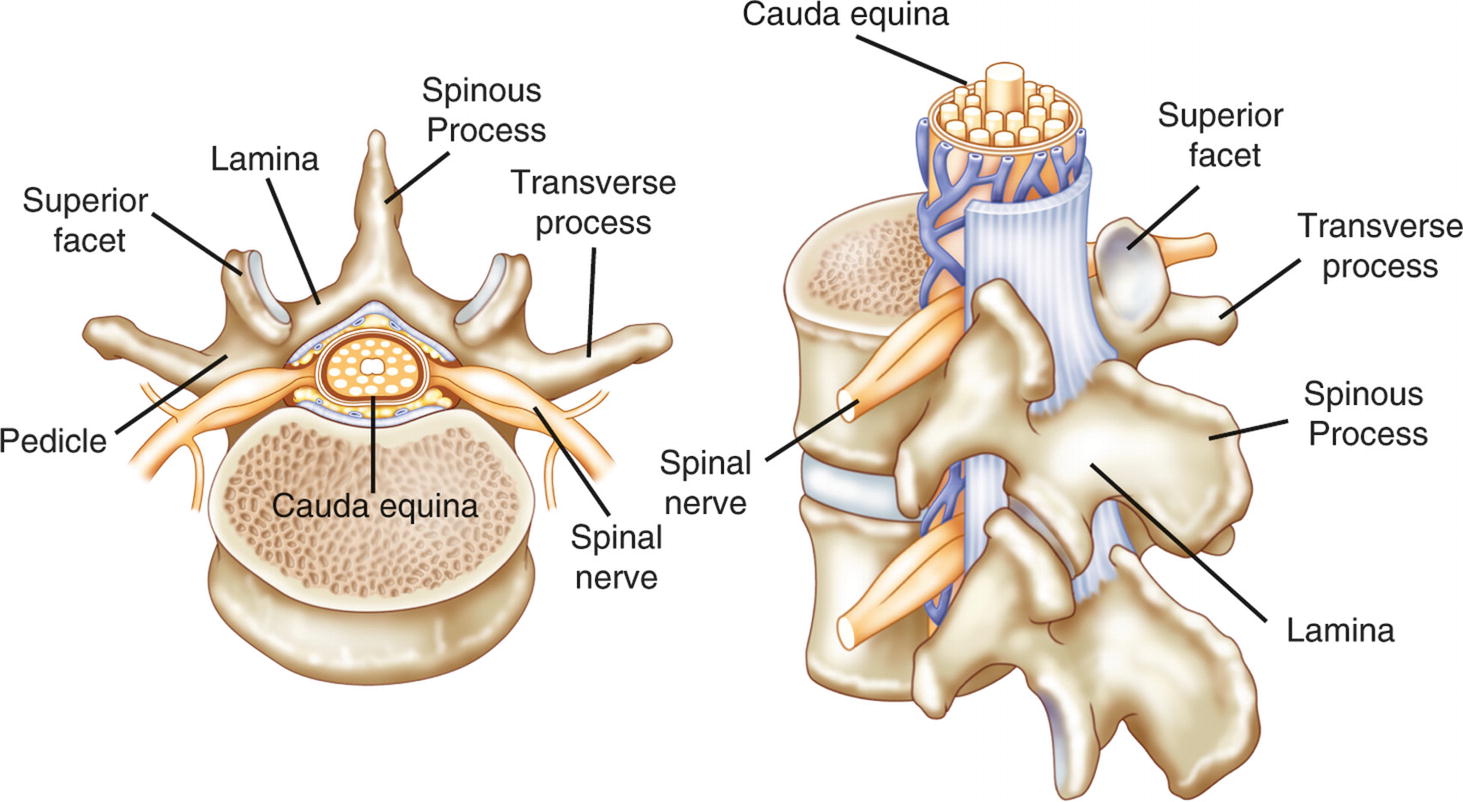
Superior view of a vertebra showing the location of the critical functional parts relative to the spinal canal. The vertebral arch protects the spinal cord and exiting nerve roots and is formed from bilateral pedicles, lamina, transverse processes, and facet joints and a single posterior spinous process
The spinal cord extends from the foramen magnum to around spinal level L1. At L1, the terminal portion of the spinal cord is called the conus medullaris. From the conus, a bundle of spinal nerves called the cauda equina further extend down to their respective vertebral level where they exit the spinal column.
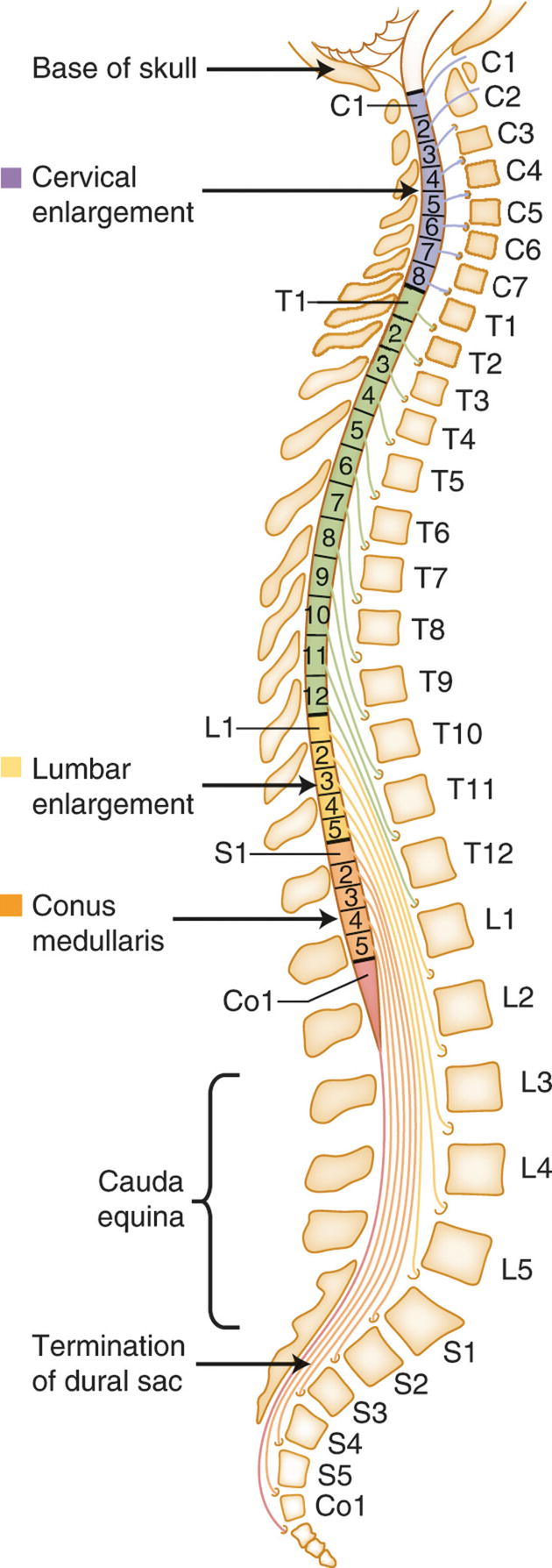
Thirty-one pairs of spinal nerve roots branch off the spinal cord. Cervical and thoracic spinal nerve roots exit laterally from the spinal canal between adjacent pedicles, while lumbosacral roots extend downward as part of the cauda equina before exiting through foramina below the spinal cord
Procedures of the Cervical Spine
The main function of the cervical spine is to support the head and allow it to move. The first cervical vertebra (C1), sometimes called the atlas , is a bony ring (not a true vertebral body) that connects directly to the skull. Together with the C2 vertebra, or axis, these two vertebral joints attach the skull to the spine and allow for a range of movement in all directions. The remaining C3–C7 vertebrae form the lordotic curve of the neck. Also specific to the cervical vertebrae is the presence of transverse foramina that enclose and protect the vertebral arteries.
Cervical spine surgery is generally performed to treat nerve impingements (radiculopathy), spinal cord compression (myelopathy), or spinal instability that is causing pain and weakness. Common cervical procedures include anterior cervical discectomy and fusion (ACDF), posterior cervical fusion (PCF), and cervical corpectomy. Risks during surgery include but are not limited to cord contusion, motor loss or weakness, peripheral nerve injury, or vascular compromise.
Injury to the C5 nerve root is the most common injury from cervical surgery and can result in pain, paresis, or paralysis of the shoulder. Other nerve roots are subject to postoperative palsy, but most complications occur at C5 due to its shorter length and more obtuse angle of exit from the foramen [1, 2]. The C5 nerve root is the only nerve supply to the deltoid muscle of the shoulder, so injury to the nerve root leads to an obvious weakness of this muscle and difficulty raising the arm to the side [2]. The potential for C5 palsies can be detected by using EMG and Tc-MEP monitoring during spinal surgery with specific focus on the deltoid and biceps brachii muscles. Brachial plexopathy resulting from positional or traction-induced injury may mimic C5 palsy [3]. Many surgeons maintain downward traction on the shoulders during a cervical surgery. Injury to the brachial plexus may result from this traction and can be detected by monitoring SSEPs during the procedure.
Anterior Cervical Discectomy and Fusion
ACDF is a procedure often performed to remove a herniated or degenerative disc. Narrowing of the vertebral canal, a condition called spinal stenosis, can cause chronic pain, numbness, and muscle weakness in both upper and lower extremities. Bone spurs can also develop resulting in foraminal stenosis thus compressing the exiting spinal nerves.
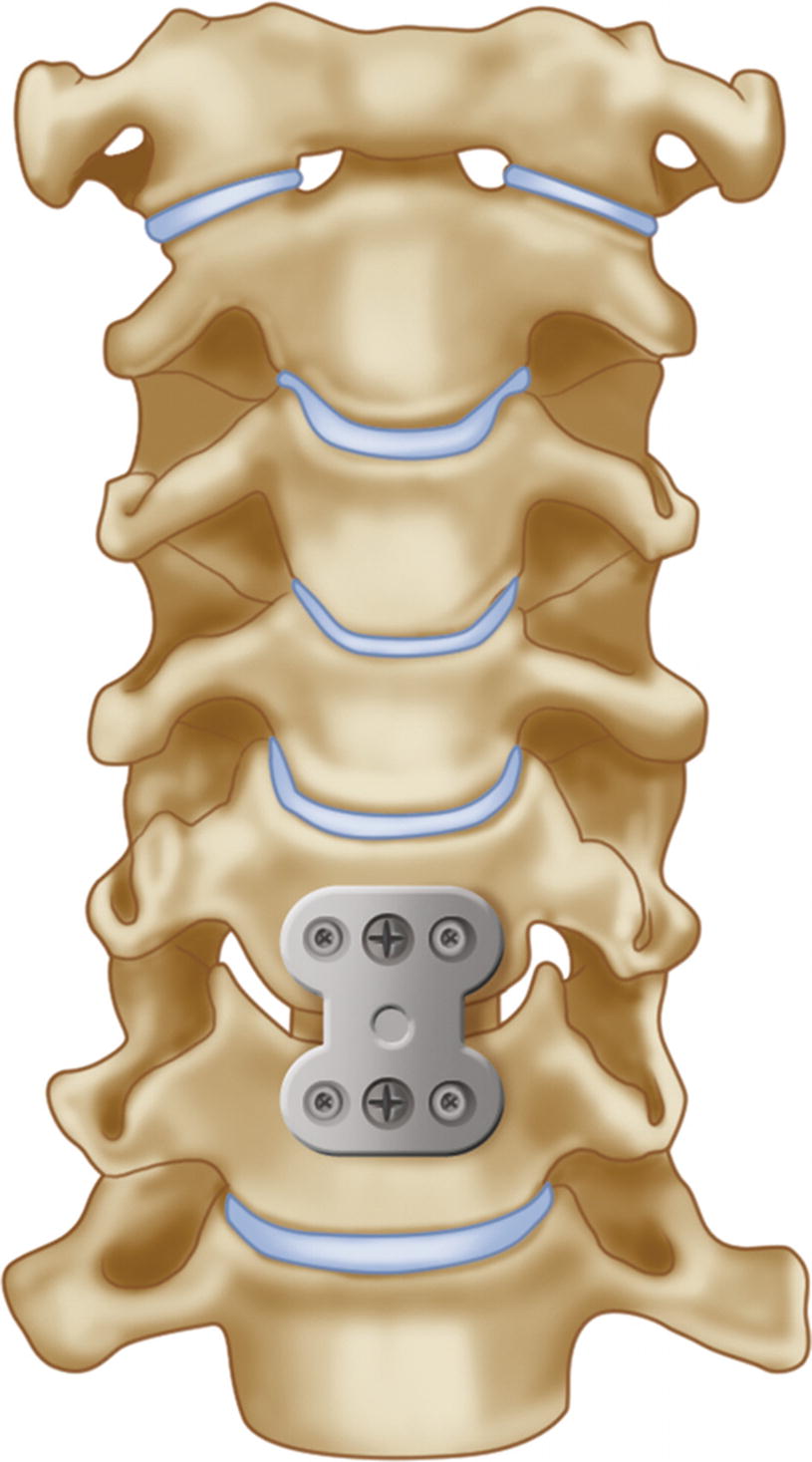
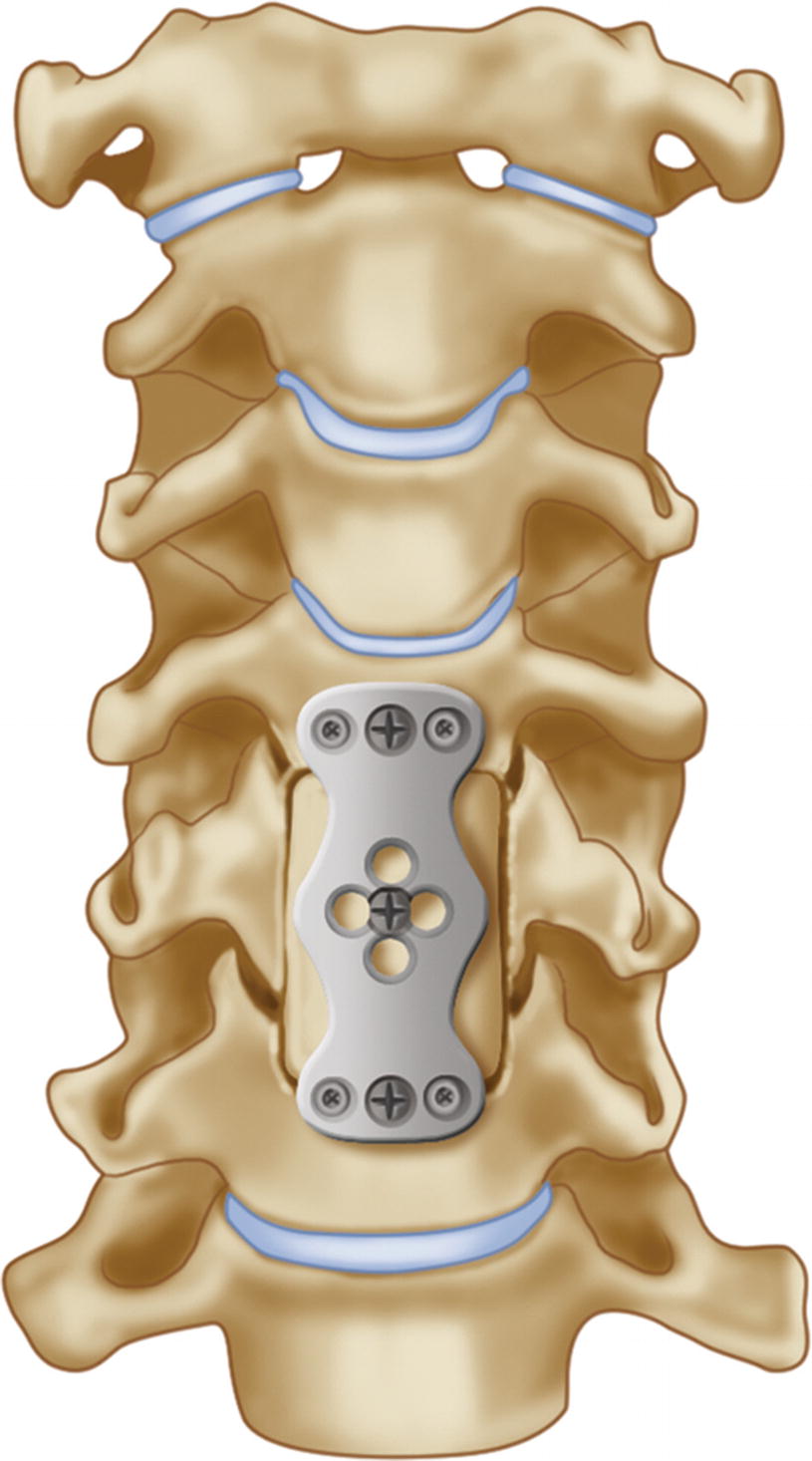
Example of a metal plate and screws placed over the bone graft during ACDF surgery
A common complication in anterior cervical surgery is vocal cord paralysis resulting from an injury to the recurrent laryngeal nerve (RLN) . Patients with RLN palsy may experience hoarseness, develop a cough, or lose their voice completely and it may take several months for the nerve to recover [4, 5]. EMG monitoring using a special endotracheal tube has been shown to be useful in detecting injury to the RLN. Monitoring the RLN is discussed in detail in Chap. 16 of this book.
Multimodality monitoring for anterior cervical fusions should include upper and lower SSEPs and Tc-MEPs to monitor spinal cord function, as well as EMG from the myotomes at risk to provide protection for the nerve roots. Positional injury may also be detected with upper extremity SSEP monitoring.
Posterior Cervical Fusion
If spinal stenosis cannot be relieved by an anterior approach, or if the patient’s spine is not stable enough before or after an anterior approach, the surgeon may opt for a posterior cervical laminectomy and fusion (PCF). The object of this procedure is the decompression of the neural elements and stabilization of the cervical spine. Posterior fusions are also performed for instability of the cervical spine resulting from trauma or a degenerative pathology.
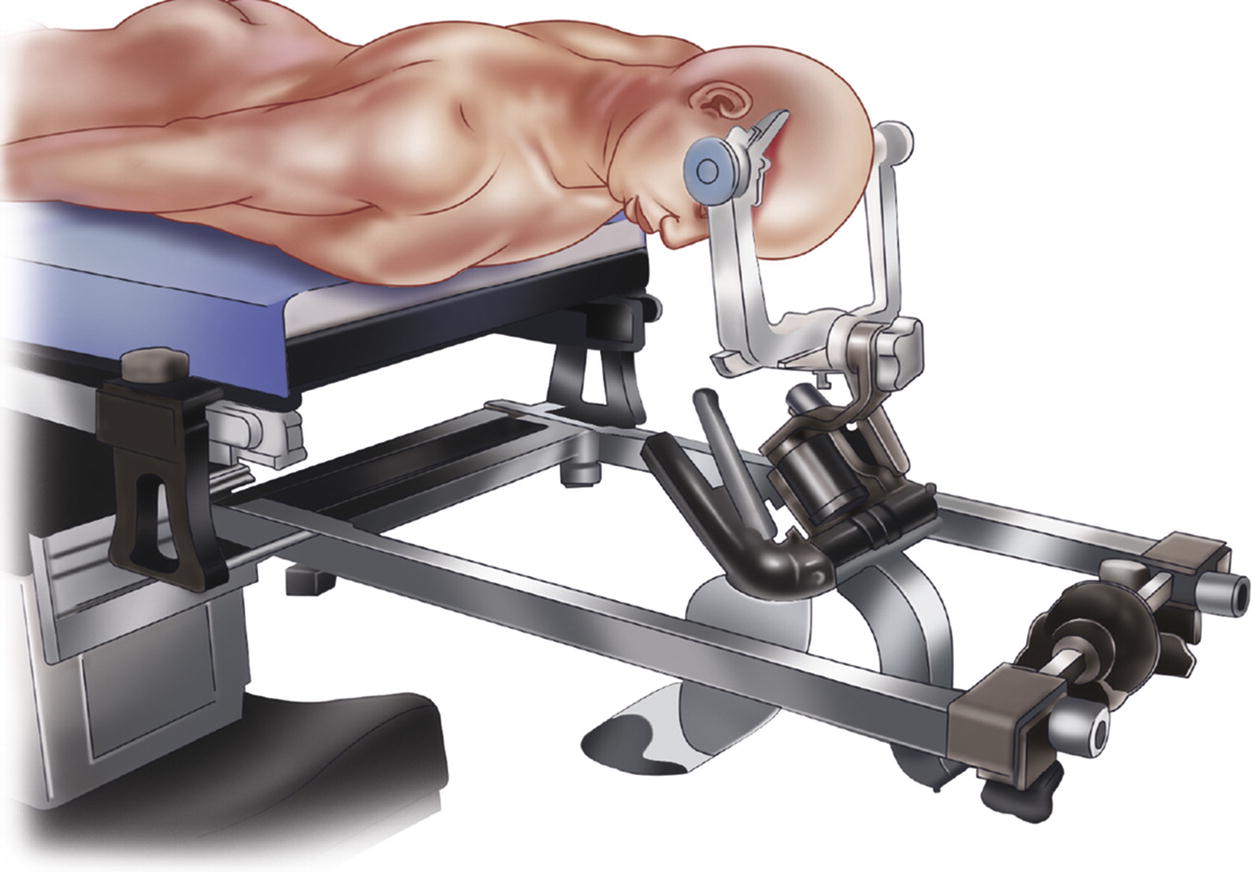
Drawing of a patient positioned for a posterior cervical fusion using a Mayfield head frame
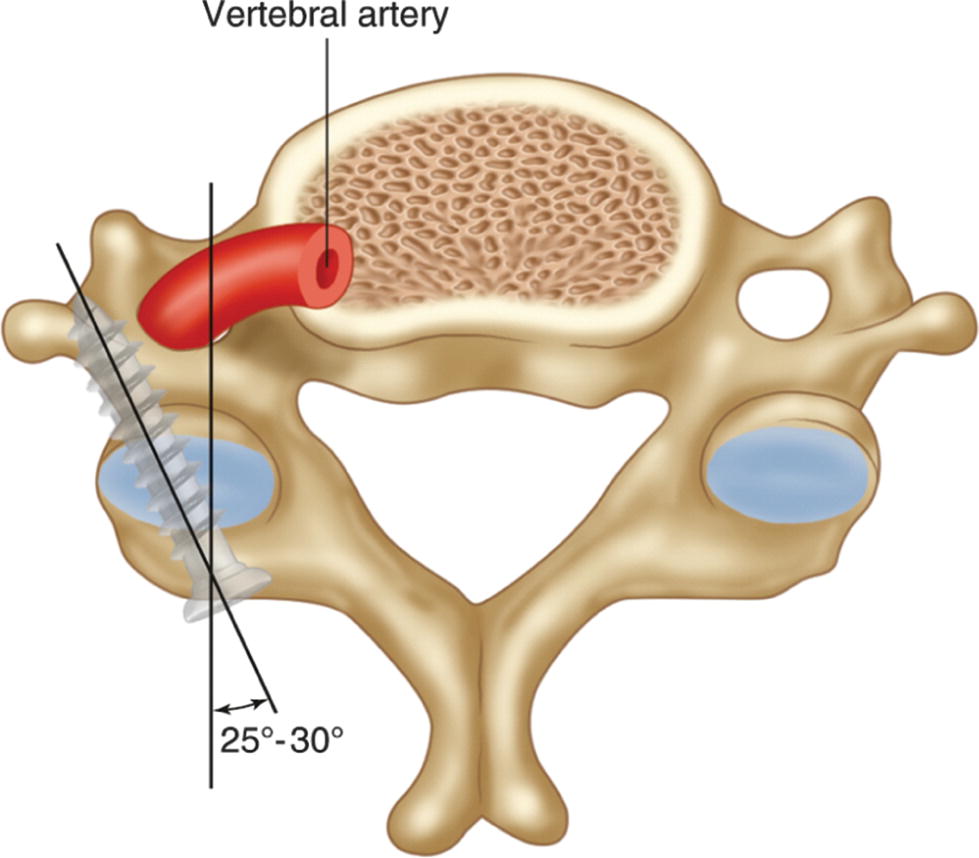
Placement of lateral mass screws in a cervical vertebra
Similar to ACDFs, multimodality monitoring using SSEPs and Tc-MEPs to monitor the spinal cord and EMGs to monitor the nerve roots is the preferred monitoring plan for PCF.
Cervical Corpectomy
Following removal of the vertebral body, a wedge-shaped bone graft is inserted into the space created by the corpectomy and is stabilized using a screw and plate system similar to an ACDF
Procedures of the Thoracic Spine
The thoracic vertebrae—T1 through T12—attach to the posterior rib cage . Due to the presence of the ribs and position of the spinous processes, the thoracic spine is stiff and motion is limited. This immobility can put strain on the adjacent cervical or lumbar spine, making the areas from C6 to T2 and T11 to L2 especially susceptible to injury. Commonly trauma or metastatic lesions are the cause of thoracic spine surgery. Thoracic laminectomy, corpectomy, and fusion are performed similarly to other levels. Burst fractures (discussed below) are often seen in the lower thoracic segments. Commonly monitored procedures of the thoracic spine are for correction of scoliosis and spinal deformity.
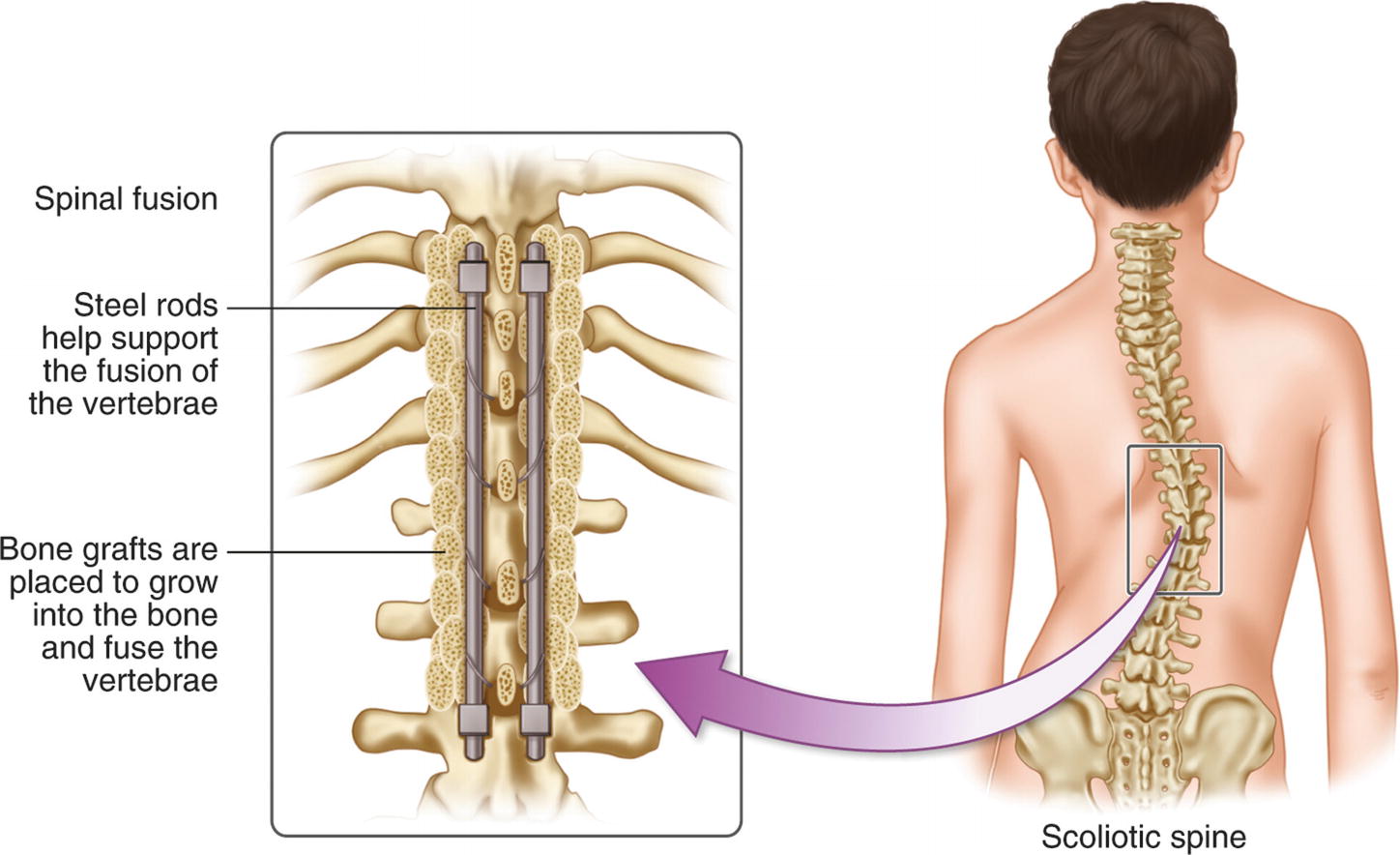
Surgery for Scoliosis Correction
Scoliosis describes an abnormal, lateral, curvature of the spine. The two most common forms of scoliosis are neuromuscular and idiopathic (also called adolescent). Neuromuscular scoliosis is usually caused by a deterioration of the facet joints and occurs most commonly in people over 65. Surgery is often performed to reduce pain. Older patients may have osteoporosis and may require many levels of instrumentation to achieve a complete fusion. Idiopathic, or adolescent scoliosis, is seen in children and teenagers and is often discovered during routine doctor’s exams. It is necessary to prevent the curvature from progressing as the child ages. If the curve measures <20°, surgeons often choose to brace the spine or continue to observe the progression of the curvature. Surgery for adolescents with scoliosis is only recommended when the curvature is >45° and continuing to progress [9]. A high degree of curvature may put the patient at risk for cardiopulmonary compromise as the curve of the spine rotates the chest and decreases the vital capacity (ability to breathe).
Scoliosis correction procedures are extensive and may require both an anterior and posterior approach in severe cases. Correcting the scoliosis involves applying different forces to the spine including distraction and rotation. These maneuvers place the spinal cord at risk for either direct injury or regional ischemic injury as blood vessels become compressed.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


