Quadrigeminal Cistern Mass
Gregory L. Katzman, MD, MBA
DIFFERENTIAL DIAGNOSIS
Common
Metastases
Less Common
Cavum Velum Interpositum (CVI)
Arachnoid Cyst
Neurocysticercosis
Ascending Transtentorial Herniation
Rare but Important
Lipoma
Epidermoid Cyst
Dermoid Cyst
Vein of Galen Malformation
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Quadrigeminal cistern (QC) lesions are smaller subset of “pineal region masses”
Bounded by quadrigeminal plate, splenium, vermis, & tentorial margin
Extends between layers of tela choroidea
Contents: Caudal internal cerebral veins, vein of Galen, PCA (quadrigeminal or P3 segment), posteromedial choroidal arteries, CNIV exit
Masses arising from QC itself (and its contents) < < those from nearby structures
Helpful Clues for Common Diagnoses
Metastases
Linear &/or nodular enhancing lesions
Image entire neuraxis!
Helpful Clues for Less Common Diagnoses
Cavum Velum Interpositum (CVI)
Axial MR/CT shows triangular-shaped CSF space between bodies of lateral ventricles
FLAIR suppresses completely
Arachnoid Cyst
Sharply demarcated extra-axial cyst that follows CSF attenuation/signal
No diffusion restriction
Neurocysticercosis
Cystic lesion isointense to CSF, may see discrete, eccentric scolex
Basal cistern cysts may be racemose
Ascending Transtentorial Herniation
Large posterior fossa mass → upward herniation of vermis → mass effect on quadrigeminal cistern ± obstructive hydrocephalus
Helpful Clues for Rare Diagnoses
Lipoma
Well-delineated, lobulated, extra-axial mass with fat attenuation/intensity
Ca++ varies from none to extensive
Epidermoid Cyst
Lobulated, irregular, CSF-like mass
FLAIR usually doesn’t completely null; diffusion yields high signal restriction
Vein of Galen Malformation
Dilated arteries feeding into large midline venous pouch
Look for prominent “flow voids” and phase artifact
Image Gallery
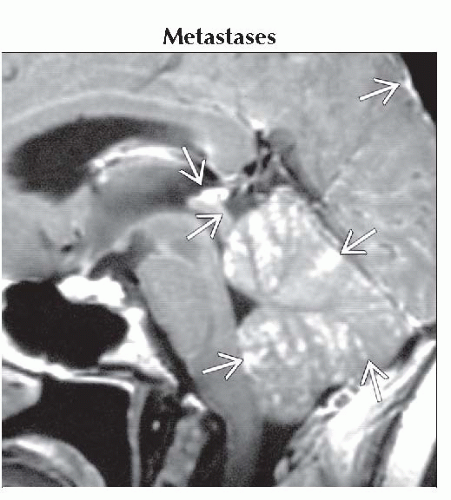 Sagittal T1 C+ MR shows typical leptomeningeal (pia & arachnoid) metastases
 in the quadrigeminal cistern as well as widespread throughout the cerebellar folia. in the quadrigeminal cistern as well as widespread throughout the cerebellar folia.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|