Quantitative EEG: special applications and multimodal monitoring
10 Quantitative EEG: special applications and multimodal monitoring
10.1 Delayed ischemia detection
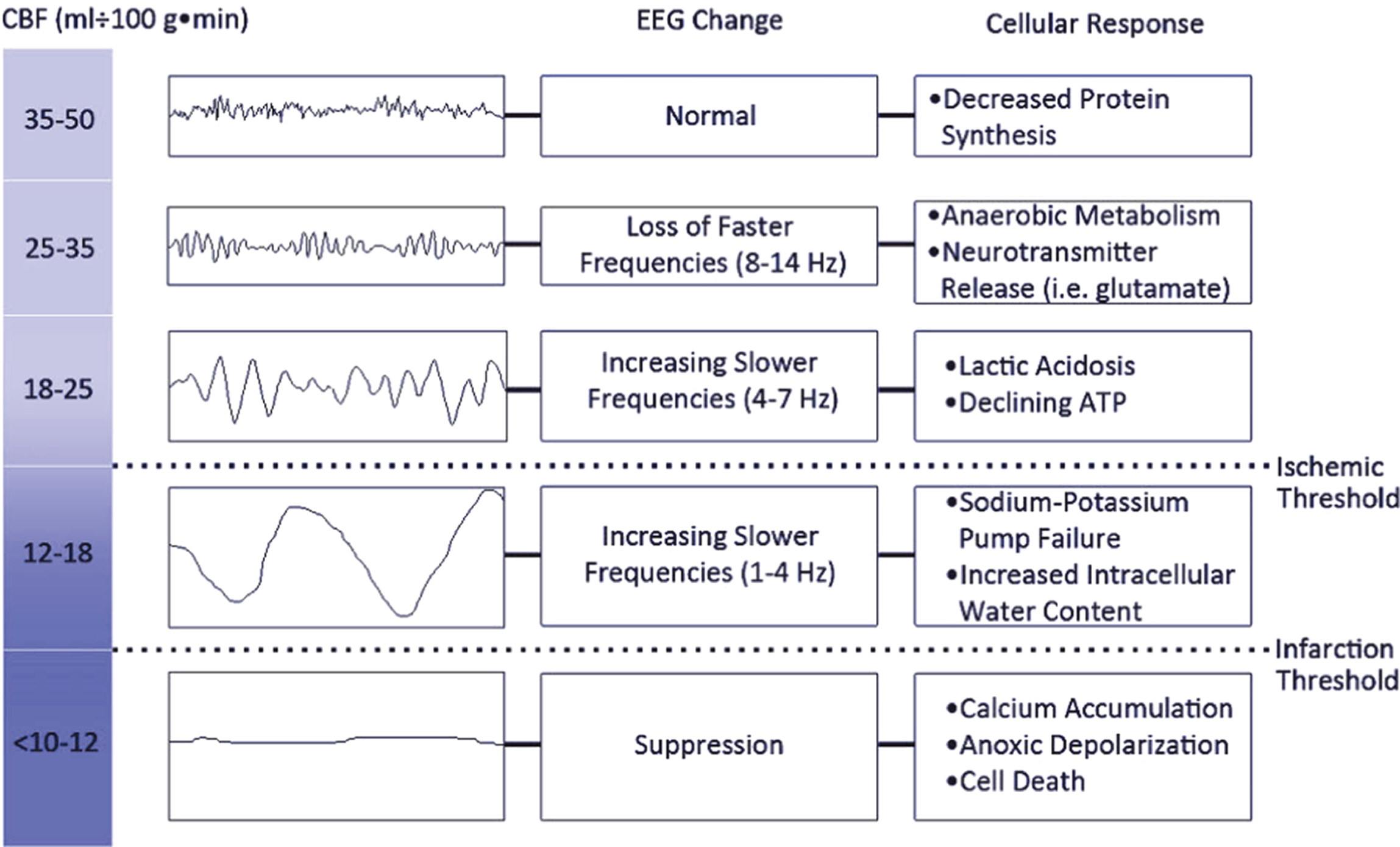
As cerebral blood flow decreases, the EEG changes in the following manner: First, there is subtle loss of faster frequencies (beta and alpha, sometimes including sleep spindles). Then, as flow drops further, slowing appears – first excess theta, then excess delta. All of this occurs while ischemia is at a reversible stage and standard anatomical imaging, including MRI with diffusion weighted imaging, remains normal. As flow continues to decline, there is suppression of all frequencies, which corresponds with irreversible neuronal death (infarction) (these changes are summarized in Figure 10.1). Thus, EEG can detect ischemia when standard imaging cannot, although perfusion imaging can also detect this. This ability of EEG to detect ischemia early with a procedure that can be done continuously is the basis for continuous EEG monitoring in patients at high risk for ischemia such as those with subarachnoid hemorrhage. Several quantitative measures can be used, which all rely on the same principle: with the development of ischemia there is loss of the more physiologic faster frequencies (activity > ∼6 Hz), and a greater degree of slowing (mostly activity <6 Hz).
10.2 Quantitative thresholds and alarms
Having multiple objective quantified trends to follow allows for the setting of thresholds and alarms to those thresholds. Alarms can alert clinicians to the earliest undesirable change so that reactive changes in therapy can be made as earliest as possible. For example, if a patient was in refractory status epilepticus and the goal was to maintain a certain level of sedation, then an alarm could be set if the power increased above a certain threshold (absolute value or relative to a defined baseline), or if the suppression percent dropped below a certain value. Seizure alarms can also be set. These often have a significant false positive rate; however, if a patient has a reliably detectable seizure pattern with little other activity, then an alarm can alert the clinician to the earliest seizure recurrence. Alarms can also be used to detect changes in cerebral function, such as delayed ischemia after subarachnoid hemorrhage (SAH). For example, an alarm can be set if the alpha/delta ratio falls below a certain value, prompting clinician review of the patient and EEG. Many variants of the fast:slow ratio can be used, and these are sensitive and fairly specific measures of ischemia. Other changes that suggest ischemia are decreases in EEG variability, including in the variability of relative alpha (alpha power/total power), and increase in epileptiform activity.
10.3 Multimodal monitoring, including intracranial EEG
With further advances in technology, multimodal monitoring has become more widely available and even a standard of care in many neurological/neurosurgical ICUs. Multimodal systems allow the integrated recording of invasive and non-invasive physiological parameters. Non-invasive measures such as heart rate, oxygen saturation, blood pressure and surface EEG can be recorded synchronously with arterial pressure, intracranial pressure, CSF measurements including lactate and neuron specific enolase, and intracranial EEG strip or depth electrode recordings. Transcranial Dopplers and near-infrared spectroscopy can be included as well. Other invasive monitoring techniques include use of intracerebral microdialysis (sample of the interstitial fluid to measure lactate, pyruvate, glucose, glutamate, glycerol, etc.), brain tissue oxygen levels, focal cerebral blood flow, brain temperature, pH and more. Such multimodal monitoring has allowed advances in our understanding of epileptiform patterns, and most importantly how these epileptiform patterns affect brain and systemic physiology.
Intracranial EEG recordings in the ICU can be obtained via subdural strips (usually placed in the operating room if neurosurgery is being performed) or intraparenchymal ‘depth’ electrodes, which can be placed bedside (or in the operating room); both types can be removed bedside and have been reported to add little if any morbidity to patients already getting other invasive brain monitoring. These electrodes can detect seizure activity that is otherwise not visible on the scalp, can provide artifact-free recordings for real-time monitoring and setting highly specific alarms, can help clarify equivocal patterns seen on the scalp EEG, and can detect peri-injury depolarization (PIDs). PIDs are related to cortical spreading depression and seem to be very common in acute brain injury, including ischemia, trauma and hemorrhages. Similar to seizures, they seem to contribute to secondary neuronal injury and are potentially treatable or preventable.
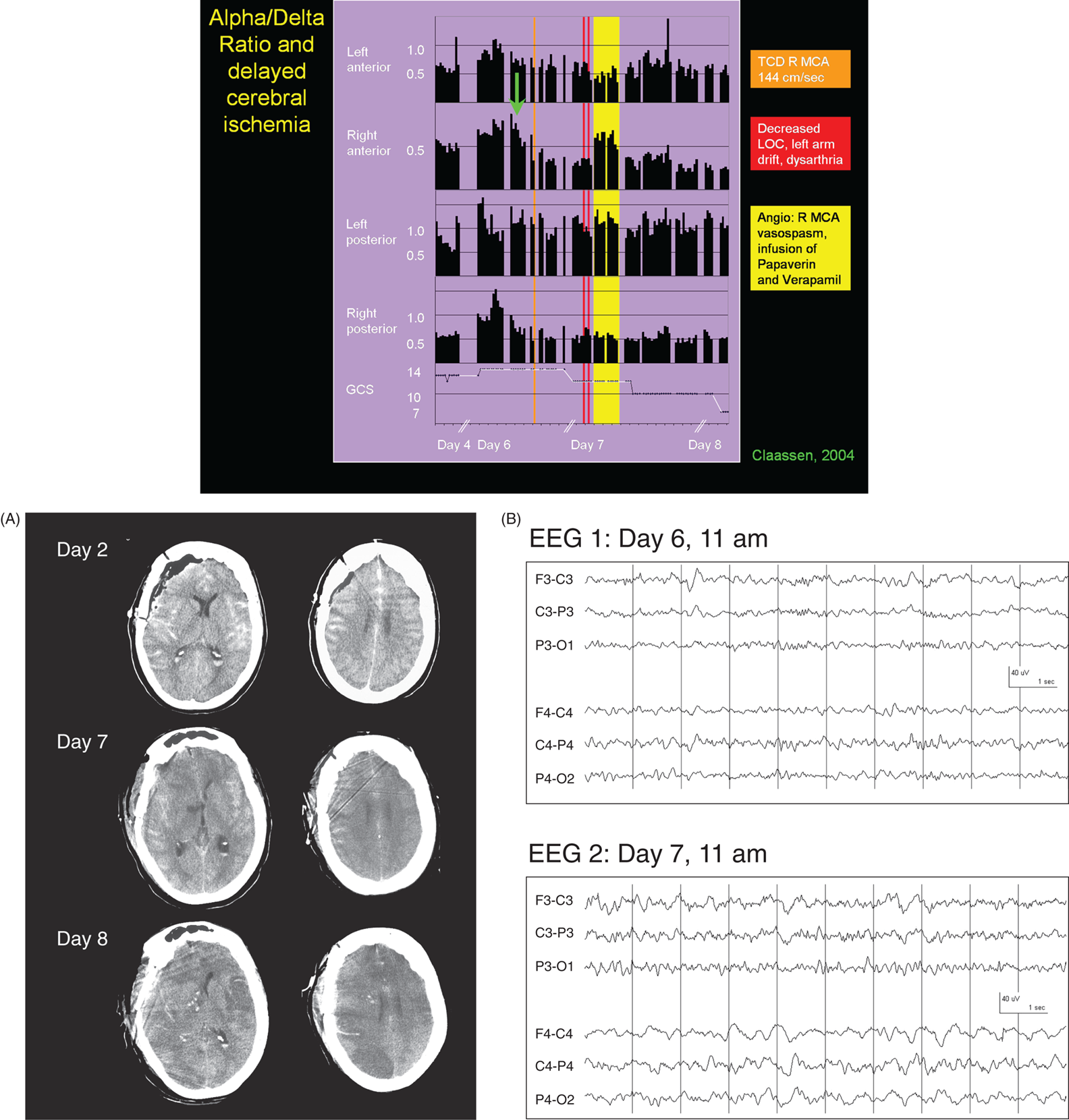
Figure 10.2 Ischemia detection: multimodality monitoring for delayed cerebral ischemia after subarachnoid hemorrhage (SAH); alpha-delta ratio.
Figure 10.3 Ischemia detection: multimodality monitoring for delayed cerebral ischemia after SAH; ADR, and alpha variability.
Figure 10.4 Ischemia detection: multimodality monitoring for delayed cerebral ischemia after SAH, using depth electrode and alarms.
Figure 10.5 Setting of alarms: multimodality monitoring; pentobarbital coma, suppression-burst, depth electrode and QEEG alarms.
Figure 10.6 Setting of alarms: hydrocephalus and multiple QEEG alarms.
Figure 10.7. Setting of alarms: envelope (amplitude) trend analysis for neonatal seizure recognition.
Figure 10.8 Setting of alarms: envelope (amplitude) trend analysis for multiple seizures in an adult.
Figure 10.9. Ischemia detection: Brain Symmetry Index during carotid clamping.
Figure 10.10 Ischemia detection and setting of alarms: Brain Symmetry Index (BSI), seizures and alarm sent to a mobile device.
Multimodality monitoring
Figure 10.11. Multimodality monitoring: electrocorticogram (ECoG) of peri-injury depolarizations and cortical spreading depression (CSD).
Figure 10.12 Multimodality monitoring: electrocorticogram (ECoG) of peri-injury depolarizations (PIDs).
Figure 10.13 Multimodality monitoring of hemorrhagic transformation of a large infarct, including with ICP, brain tissue oxygen tension, cerebral microdialysis and depth electrode.
Figure 10.14 Multimodality monitoring of seizures on intracranial EEG after meperidine bolus, including ICP, cerebral microdialysis and depth electrode.
Figure 10.15 Multimodality monitoring of traumatic brain injury (TBI), including ICP, brain tissue oxygen tension, cerebral microdialysis and depth electrode.
Figure 10.16. Multimodal monitoring of traumatic brain injury (TBI), including ICP, brain tissue oxygen tension, cerebral microdialysis and depth electrode.
Figure 10.17 Multimodality monitoring: ictal-appearing SIRPIDs on intracranial EEG only.
Figure 10.18. Multimodality monitoring: Cyclic seizures on intracranial EEG only.
Figure 10.19 Multimodality monitoring: TBI, seizures and periodic discharges on intracranial EEG only, QEEG applied to intracranial EEG.
EEGs throughout this atlas have been shown with the following standard recording filters unless otherwise specified: LFF 1 Hz, HFF 70 Hz, notch filter off.
Suggested reading
Baang HY, Chen HY, Herman AL, et al. The utility of quantitative EEG in detecting delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage. J Clin Neurophysiol. 2021.
Claassen J, Hirsch LJ, Frontera JA, Fernandez A, Schmidt M, Kapinos G, Wittman J, Connolly ES, Emerson RG, Mayer SA. Prognostic significance of continuous EEG monitoring in patients with poor grade subarachnoid hemorrhage. Neurocrit Care 2006; 4(2):103–112.
Claassen J, Hirsch LJ, Kreiter KT, et al. Quantitative continuous EEG for detecting delayed cerebral ischemia in patients with poor-grade subarachnoid hemorrhage. Clin Neurophysiol. 2004; 115(12):2699–2710.
Claassen J, Hirsch LJ, Kreiter K, Du YE, Connolly ES, Emerson RG, Mayer SA. Quantitative continuous EEG for detecting delayed cerebral ischemia in subarachnoid hemorrhage. Clin Neurophysiol 2004; 115:2699–2710.
Claassen J, Perotte A, Albers D, et al. Nonconvulsive seizures after subarachnoid hemorrhage: multimodal detection and outcomes. Ann Neurol. 2013; 74(1):53–64.
de Vos CC, van Maarseveen SM, Brouwers PJ, van Putten MJ. Continuous EEG monitoring during thrombolysis in acute hemispheric stroke patients using the brain symmetry index. J Clin Neurophysiol. 2008 Apr; 25(2):77–82.
Dohmen C, Sakowitz OW, Fabricius M, Bosche B, Reithmeier T, Ernestus RI, Brinker G, Dreier JP, Woitzik J, Strong AJ, Graf R; Co-Operative Study of Brain Injury Depolarisations (COSBID). Spreading depolarizations occur in human ischemic stroke with high incidence. Ann Neurol. 2008 Jun; 63(6):720–728.
Dreier JP, Woitzik J, Fabricius M, Bhatia R, Major S, Drenckhahn C, Lehmann TN, Sarrafzadeh A, Willumsen L, Hartings JA, Sakowitz OW, Seemann JH, Thieme A, Lauritzen M, Strong AJ. Delayed ischaemic neurological deficits after subarachnoid haemorrhage are associated with clusters of spreading depolarizations. Brain. 2006 Dec; 129(Pt 12):3224–3237.
Fabricius M, Fuhr S, Bhatia R, Boutelle M, Hashemi P, Strong AJ, Lauritzen M. Cortical spreading depression and peri-infarct depolarization in acutely injured human cerebral cortex. Brain. 2006 Mar; 129(Pt 3):778–790.
Fabricius M, Fuhr S, Willumsen L, Dreier JP, Bhatia R, Boutelle MG, Hartings JA, Bullock R, Strong AJ, Lauritzen M. Association of seizures with cortical spreading depression and peri-infarct depolarisations in the acutely injured human brain. Clin Neurophysiol. 2008 Sep; 119(9):1973–1984.
Foreman B, Claassen J. Quantitative EEG for the detection of brain ischemia. Crit Care. 2012; 16(2):216
Foreman B, Albers D, Schmidt JM, et al. Intracortical electrophysiological correlates of blood flow after severe SAH: A multimodality monitoring study. J Cereb Blood Flow Metab. 2018; 38(3):506–517.
Hartings JA, Andaluz N, Bullock MR, et al. Prognostic value of spreading depolarizations in patients with severe traumatic brain injury. JAMA Neurol. 2020; 77(4):489–499.
Kim JA, Zheng WL, Elmer J, et al. High epileptiform discharge burden predicts delayed cerebral ischemia after subarachnoid hemorrhage. Clin Neurophysiol. 2021.
Kramer AH, Kromm J. Quantitative continuous EEG: Bridging the gap between the ICU bedside and the EEG interpreter. Neurocrit Care. 2019; 30(3):499–504.
Leão AAP. Spreading depression of activity in the cerebral cortex. Journal of Neurophysiology. 1944; 7(6):359–390.
Mikell CB, Dyster TG, Claassen J. Invasive seizure monitoring in the critically-ill brain injury patient: current practices and a review of the literature. Seizure. 2016; 41:201–205.
Ponten SC, Ronner HE, Strijers RLM, et al. Feasibility of online seizure detection with continuous EEG monitoring in the intensive care unit. Seizure. 2010; 19(9):580–586.
Rathakrishnan R, Gotman J, Dubeau F, Angle M. Using continuous electroencephalography in the management of delayed cerebral ischemia following subarachnoid hemorrhage. Neurocrit Care. 2011; 14(2):152–161.
Rosenthal ES, Biswal S, Zafar SF, et al. Continuous electroencephalography predicts delayed cerebral ischemia after subarachnoid hemorrhage: A prospective study of diagnostic accuracy. Ann Neurol. 2018; 83(5):958–969.
Rots ML, van Putten MJ, Hoedemaekers CW, Horn J. Continuous EEG monitoring for early detection of delayed cerebral ischemia in subarachnoid hemorrhage: a pilot study. Neurocrit Care. 2016; 24(2):207–216.
Strong AJ, Anderson PJ, Watts HR, Virley DJ, Lloyd A, Irving EA, Nagafuji T, Ninomiya M, Nakamura H, Dunn AK, Graf R. Peri-infarct depolarizations lead to loss of perfusion in ischaemic gyrencephalic cerebral cortex. Brain. 2007 Apr; 130(Pt 4):995–1008.
Tu B, Assassi NJ, Bazil CW, Hamberger MJ, Hirsch LJ. Quantitative EEG is an objective, sensitive, and reliable indicator of transient anesthetic effects during Wada tests. J Clin Neurophysiol. 2015; 32(2):152–158.
van Putten MJ. The revised brain symmetry index. Clin Neurophysiol. 2007 Nov; 118(11):2362–2367. Epub 2007 Sep 20.
van Putten MJ. Extended BSI for continuous EEG monitoring in carotid endarterectomy. Clin Neurophysiol. 2006 Dec; 117(12):2661–2666.
van Putten MJ, Tavy DL. Continuous quantitative EEG monitoring in hemispheric stroke patients using the brain symmetry index. Stroke. 2004 Nov; 35(11):2489–2492.
Vespa P, Tubi M, Claassen J, et al. Metabolic crisis occurs with seizures and periodic discharges after brain trauma. Ann Neurol. 2016; 79(4):579–590.
Vespa PM, Nuwer MR, Juhász C, Alexander M, Nenov V, Martin N, Becker DP. Early detection of vasospasm after acute subarachnoid hemorrhage using continuous EEG ICU monitoring. Electroencephalogr Clin Neurophysiol. 1997 Dec; 103(6):607–615.
Vespa PM, Nuwer MR, Nenov V, et al: Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring. J Neurosurg. 1999; 91(5):750–760.
Waziri A, Claassen J, Stuart RM, et al. Intracortical electroencephalography in acute brain injury. Ann Neurol. 2009; 66(3):366–377.
Witsch J, Frey HP, Schmidt JM, et al. Electroencephalographic periodic discharges and frequency-dependent brain tissue hypoxia in acute brain injury. JAMA Neurol. 2017; 74(3):301–309.
Figure 10.1. Cerebral ischemia. The table outlines the cerebral blood flow (CBF) and the respective estimates of the cellular and molecular changes, and EEG changes (middle column). With falling CBF the brain switches to anaerobic metabolism that results in falling cerebral glucose and increasing lactate. These changes can be detected with regular intracerebral sampling (as seen in Figures 10.13–10.16). The EEG changes are well described, with progressive loss of more ‘physiologic’ rhythms (alpha and beta), with gradual increase in theta and delta activity. These changes occur while there is still ‘reversibility’, and therefore the goal of ischemia detection is to use these changes to prompt an intervention to prevent non-reversible ischemia/infarction. ATP, adenosine triphosphate.
Reproduced from Foreman B, Claassen J. Quantitative EEG for the detection of brain ischemia. Crit Care. 2012;16(2):216, with permission.
Figure 10.2. Ischemia detection: multimodal monitoring for delayed cerebral ischemia after subarachnoid hemorrhage (SAH); alpha-delta ratio.
Figure 10.2main: This 57-year-old woman was admitted for an acute subarachnoid hemorrhage (admission Hunt and Hess grade 4) from a right posterior communicating aneurysm. The aneurysm was clipped on SAH day 2. No infarcts were seen on postoperative CT, day 2 (shown, Figure 10.2A). Postoperatively she had a Glasgow Coma Score (GCS) of 14. CEEG monitoring was performed from SAH days 3 to 8 to monitor for seizures and delayed cerebral ischemia. The figure shows the Alpha/delta ratio (ADR) calculated every 15 minutes and the Glasgow Coma Score (GCS), shown for days 6–8 of continuous EEG (cEEG) monitoring. The alpha/delta ratio progressively decreased after day 6, particularly in the right anterior region (green arrow), to settle into a steady trough level later that night, reflecting loss of fast frequencies and increased slowing over the right hemisphere in the raw EEG (also shown, Figure 10.2
Only gold members can continue reading. Log In or Register to continue