40 Radiofrequency Kyphoplasty: A Novel Approach to Minimally Invasive Treatment of Vertebral Compression Fractures
KEY POINTS
Introduction
Percutaneous treatment of vertebral compression fractures (VCFs) was first performed in France in 1984 by Galibert and Deramond.1 The two most commonly performed minimally invasive VCF procedures are known as vertebroplasty and kyphoplasty. The primary difference is that in kyphoplasty, commonly referred to as percutaneous vertebral augmentation, a cavity using a mechanical device is created before cement delivery.∗ Both procedures have been shown to provide dramatic pain relief in vertebral body fractures associated with underlying osteoporosis or malignancy, and have been successfully applied in cases in which conservative management has failed and surgery is undesirable.1–7, 10–14 Because they have a higher incidence of osteoporosis, most patients referred for this procedure are women. However, men with vertebral body fractures from osteoporosis also present for treatment. Many of the characteristics of the male population with osteoporotic vertebral body fractures have recently been described.4,7 Vertebral body fractures are the most common osteoporotic fractures in men. Like those in women, they are associated with significant morbidity and restriction of activities of daily living.8 The economic impact of osteoporotic fractures was estimated at nearly $2.7 billion in 1995 for men alone,9 making this a substantial health care problem from the standpoint of both cost and morbidity.
Minimally invasive treatment of vertebral compression fractures requires the image-guided insertion of a needle or working cannula through or adjacent to the pedicle into the vertebral body. Acrylic or calcium phosphate bone cement is then injected into the vertebral body (either with or without performing cavity creation) where it solidifies, providing structural support and preventing the movement associated with pain.3,14
The StabiliT Vertebral Augmentation System (DFine Inc., San Jose, CA, USA) is a novel product intended for the treatment of VCFs associated with osteoporotic fractures and tumors of the spine in a procedure known as radiofrequency (RF) kyphoplasty. RF kyphoplasty is designed to minimize leakage, enable height restoration of mobile fractures, and provide pain relief through fracture stabilization by way of site- and size-specific cavity creation and extended, controlled delivery of an ultrahigh viscosity cement. This new percutaneous vertebral augmentation system combines the following unique attributes: navigational cavity creation device; RF energy modulated, ultra-high viscosity cement; unique, hydraulic delivery system; and a remotely controlled delivery mechanism to offer additional control to the physician in treatment of a VCF. The use of RF energy to modulate bone cement polymerization immediately before entering the patient permits the system to maintain cement in a reservoir at ambient temperature with a very long working time, yet deliver cement of a viscosity many times higher than conventionally delivered polymethyl methacrylate (PMMA) cement. This control during the cement delivery results in the potential for reduced venous extravasation and yet retains the ability to move bone fragments and restore height.
Materials and Methods
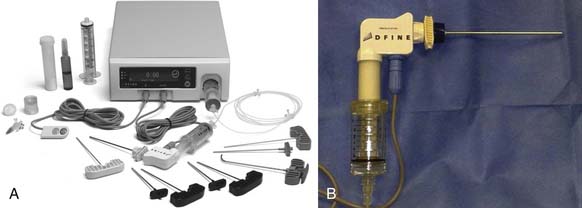
The StabiliT Vertebral Augmentation System
The StabiliT Vertebral Augmentation System is a unique RF controlled cement delivery system for the treatment of vertebral compression fractures. It has been cleared for use in the United States for percutaneous delivery of StabiliT ER (Energy Responsive) Bone Cement in kyphoplasty procedures in the treatment of painful vertebral compression fractures, which may result from osteoporosis, benign lesions (hemangioma), and malignant lesions (metastatic cancers, myeloma). It contains the following components: a proprietary energy-responsive PMMA bone cement (StabiliT ER Bone Cement); a unique vacuum saturation cement mixing system (Saturate Mixing System); a controller (Mulitplex Controller) that contains both a radiofrequency generator and a hydraulic drive; introducer/working cannulae for access to the vertebral body; straight and navigational cavity creation devices to permit specificity of the site and size of the cavity; a PFA (Teflon-like)-lined heating element (Activation Element) and delivery cannulae to permit the delivery of uniquely high viscosity PMMA cement; and a 3-m-long cable to permit remote-control delivery of the cement, thereby controlling the operator’s radiation exposure (Figure 40-1). Following cavity creation using the articulated arm of the MidLine Osteotome, the StabiliT System (DFine Inc., San Jose, CA, USA) preferentially delivers cement to the cavity but further permits interdigitation of the ultra-high viscosity cement into the adjacent trabecular beds (Figure 40-2).
Related posts:
 Embryology of the Spine
Embryology of the Spine
 Non-Invasive Strength Analysis of the Spine Using Clinical CT Scans
Non-Invasive Strength Analysis of the Spine Using Clinical CT Scans
 Tumors of the Cervical Spine
Tumors of the Cervical Spine
 Rheumatoid Arthritis of the Cervical Spine
Rheumatoid Arthritis of the Cervical Spine
 Dorsal Endoscopic Rhizotomy for Chronic Nondiscogenic Axial Low Back Pain
Dorsal Endoscopic Rhizotomy for Chronic Nondiscogenic Axial Low Back Pain
 Interspinous Spacers for Minimally Invasive Treatment of Dynamic Spinal Stenosis and Low Back Pain
Interspinous Spacers for Minimally Invasive Treatment of Dynamic Spinal Stenosis and Low Back Pain
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


