♦ Preoperative
Operative Planning
- While peripheral nerve tumors often present with subtle signs and symptoms, a thorough physical examination and history is essential.
- Magnetic resonance imaging of the extremity with and without contrast. On occasion, fat suppression sequences may facilitate better visualization.
- Electrophysiology: electromyography (EMG) is necessary to define any motor and sensory deficit (with the understanding that EMGs are operator-dependent).
- Major set-up
- Intraoperative electrophysiology including the ability to directly stimulate and record from the nerve
Operating Room Set-up
- Headlight
- Loupes
- Bipolar cautery and Bovie cautery
Anesthetic Issues
- Short-acting muscle relaxants and paralytics are essential for good intraoperative monitoring.
- Regional anesthetic blocks will also interfere with intraoperative EMG.
Monitoring
- Intraoperative monitoring mentioned previously
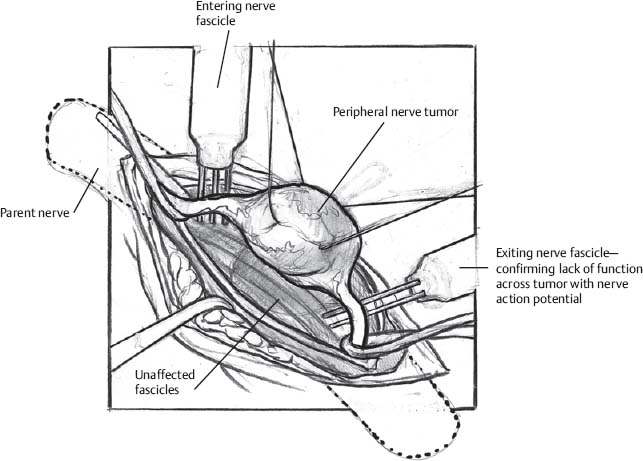
♦ Intraoperative (Fig. 155.1)
Peripheral Neural Sheath Tumor
Benign schwannomas and neurofibromas have different techniques because of differing patterns of fascicular involvement.
- Schwannoma grows extrinsic to its parent fascicles
- Patient is positioned such that the involved limb’s response to electrophysiologic stimulation can be observed.
- Lengthy longitudinal incision over the mass to include exposure of the nerve at points proximal and distal to the tumor
- Entering/exiting whole nerves are encircled with Penrose drains.
- Incision made down to the tumor capsule
- Displaced and “thinned out” nerve fascicles are dissected away from the tumor capsule.
- Interfascicular dissection both at proximal and distal ends of the tumor for a singular and small fascicular input and similar output
- Isolate fascicles with vasoloops.
- Nerve action potential stimulation and recording across the fascicle entering and exiting each pole of the tumor usually show them to be nonfunctional.
- They are then sacrificed.
- Isolate fascicles with vasoloops.
- Tumor is removed as a single mass whenever possible; with large tumors, the tumor capsule may be opened longitudinally, enucleate the usually soft/homogeneous and sometimes cystic tumoral contents. Then, resect the capsule from the spared fascicles. When the tumor mass is large and firm, Cavitron ultrasonic aspirator may be used to debulk the tumor.
- Patient is positioned such that the involved limb’s response to electrophysiologic stimulation can be observed.
Only gold members can continue reading. Log In or Register to continue








