(Vestibular Schwannomas)
♦ Preoperative
Operative Planning
- Gamma knife should be considered for small- or medium-sized tumors, depending on the patient’s age, medical condition, hearing status, and desires
- Magnetic resonance imaging: determine location, size, and relationships of tumor to adjacent structures such as brain stem and encased arteries
- Computed tomography (optional): assess bony anatomy of petrous temporal bone, middle fossa, posterior fossa, internal auditory canal, vestibule, semicircular canals, mastoid and petrous air cells, and jugular bulb
Additional Testing
- Comprehensive audiologic evaluation: pure-tone audiometry, speech discrimination testing, and brain stem auditory evoked responses
Equipment
- Craniotomy tray
- Irrigating bipolar cautery
- Kartush dissector/nerve stimulator
Anesthetic Issues
- Anesthesiologist needs to be aware that electrophysiological monitoring of cranial nerve (CN) VII, CN VIII, and somatosensory evoked potential will be performed
♦ Intraoperative (Fig. 14.1)
Removal of Small Tumors
- The inferolateral cerebellar hemisphere is retracted gently to allow cerebrospinal fluid (CSF) drainage from the cisterna magna
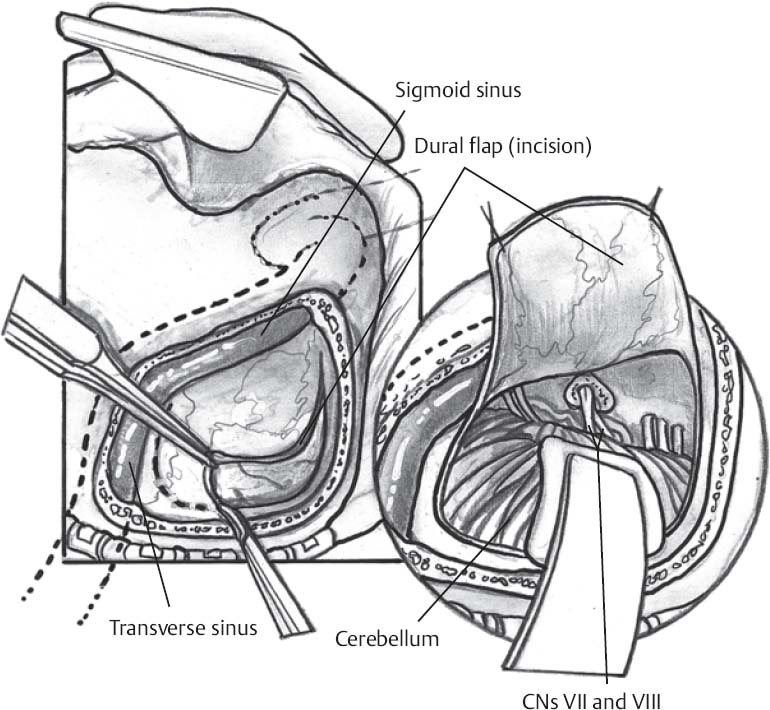
Fig. 14.1 Illustration of retrosigmoid approach to acoustic neuromas. CNs, cranial nerves.
Intraoperative Monitoring
- Surgical dissection and resection are assisted by electrophysiological monitoring of CN V, CN VII, and CN VIII for small to medium tumors as well as lower CN IX, CN X, and CN XI for large tumors
- After placement of the brain retractor on the later cerebellar hemisphere, the operating microscope is positioned
- The facial and vestibulocochlear nerves, which are usually anteriorly displaced by the tumor, are identified both at the brain stem and within the internal auditory canal (IAC)
- The facial nerve origin at the brain stem is adjacent to the pontomedullary sulcus, which marks the junction of the pons and medulla
- The vestibulocochlear nerve joins the brain stem and the pontomedullary sulcus 1 to 2 mm posterior to the facial nerve origin
- The origins of cranial nerves IX, X, and XI are 2 to 3 mm inferior to the origin of the facial nerve
- The facial nerve origin at the brain stem is adjacent to the pontomedullary sulcus, which marks the junction of the pons and medulla
- After originating at the basilar artery, the anterior inferior cerebellar artery (AICA) courses laterally supply branches to the cochlear nerve in the IAC, then forms a meatal loop that continues medially between CN VIII and CN IX to supply the brain stem and cerebellum
- The meatal loop is usually situated in front of the porus acusticus or within the IAC
- The AICA can be displaced inferiorly, anteriorly, superiorly by the tumor
- The posterior inferior cerebellar artery (PICA) originates from the vertebral artery in close proximity CN IX, CN X, and CN XI
- The petrosal vein is identified
- The dura overlying the posterior wall of the acoustic meatus is coagulated, incised sharply with a no. 11 blade, and then mobilized with a curette
- A high-speed drill with a 5-mm and 2-mm diamond burr is used to remove the posterior wall of the IAC; the extent of bone removal is guided by the size of the intracanalicular portion of the tumor
- After the bone removal is completed, the intracanalicular dura is exposed, coagulated, opened horizontally, and reflected to reveal the intracanalicular part of the tumor, which has usually displaced the facial and cochlear nerves anteriorly
- The arachnoid overlying the tumor is opened
- The tumor capsule is coagulated and incised with microscissors
- Internal decompression of the tumor is performed with suction, tumor forceps, and microfreer
- Tumor dissection in the arachnoid plane outside the tumor capsule is performed with judicious use of the Kartush nerve stimulator/dissector to confirm the position of the facial nerve
- Beginning at the medial boundary of the tumor, dissection along the facial and cochlear nerves proceeds from a medial to a lateral direction by means of straight or curved microdissectors and microscissors
- Once the superior vestibular nerve is identified to be the nerve of origin, it may be divided medial to the tumor
- Dissection is performed from alternating directions to optimize exposure of the dissection plane and to minimize tension on the facial and cochlear nerves
- Preservation of the auditory artery is essential to prevent hearing compromise
- If the vestibular nerve can be identified lateral to the tumor, it may be divided at this point; if the lateral margin of the tumor continues into the IAC, the tumor is transected near the end of the canal and a small ring curette is used to remove the intracanalicular portion of the tumor
- Bone wax is used to seal the mastoid air cells within the IAC
- The meatal loop is usually situated in front of the porus acusticus or within the IAC
Removal of Medium Tumors
- Facial nerve displacement by an acoustic neuroma is most commonly anterior, followed by (in decreasing order of frequency) inferior, superior, and posterior displacement
- Following the internal decompression of a tumor with an extracanalicular component, the tumor dissection is begun at its medial aspect to eliminate its medial blood supply
- Dissection is continued in the arachnoid plane between the tumor and the brain stem as the tumor capsule is reflected laterally away from the flocculus
- The Kartush dissector is used to identify the location of the facial nerve
- The facial nerve is stretched and most susceptible to injury at the point of entry into the IAC, at the proximal rim of the porus acusticus
- The Kartush dissector is used to identify the location of the facial nerve
Removal of Large Tumors
- Resection of a portion of the lateral cerebellum may be required for access to the tumor
- The extracanalicular portion is internally decompressed to diminish the tension on the cranial nerves
- The superior cerebellar artery (SCA) courses above the trigeminal nerve and may be superiorly displaced by a tumor
- The tumor capsule is reflected off CN IX, CN X, and CN XI
- Progressive resection from a medial to lateral direction allows visualization of the brain stem
- The course of the facial nerve is identified with the Kartush dissector
- Large tumors usually require dissection from the trigeminal nerves
- Following the removal of the extracanalicular portion, dissection is continued in the region of the porus acusticus as detailed above
- The facial nerve is stimulated following completion of tumor resection to ensure continuity and to prognosticate postsurgical facial function
Closure
- Wounds irrigated
- Dural edges approximated with 4–0 silk sutures, pericranium, and stamps of muscle; dural substitute duraplasty to enhance watertight closure
- The mastoid cavity is filled with an adipose graft; the fat graft is supported with sutures to prevent migration into the posterior fossa
- Cranioplasty is fashioned with titanium mesh and methylmethacrylate to the size of the craniectomy
- Muscle reapproximated over supported adipose graft with 0–0 Vicryl
- Interrupted inverted 2–0 Vicryl sutures in fascia
- Staples or 3–0 nylon sutures in skin
- Sterile mastoid-ear dressing
♦ Postoperative
- Antibiotics continued for 24 hours
- Observe for CSF rhinorrhea and CSF leakage from skin
- Monitor for hydrocephalus due to hemorrhage or edema of the brain stem or cerebellum
- Steroids tapered slowly over 10 to 14 days
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue








