Chapter 86 Rheumatoid Arthritis
Rheumatoid arthritis is a systemic disease of unknown cause that primarily involves small blood vessels and synovium. A chronic disease, it is generally more common in females. This disorder is characterized by polyarticular symmetrical involvement of the smaller joints of the appendicular skeleton. It destroys the articular joint surfaces and the joint capsules as well as the ancillary ligaments that support the joints.1 In addition, rheumatoid arthritis can be associated with osteoporosis and erosion and cyst formation in the bone.2 The extent of myelopathy in patients with rheumatoid arthritis is difficult to evaluate because their disease may be complicated by peripheral joint destruction, peripheral neuropathies, nerve entrapments, and rheumatoid myopathy.3
The most common skeletal manifestation of rheumatoid arthritis occurs with the involvement of the metatarsophalangeal joints of the feet. This is followed in frequency by rheumatoid involvement of the cervical spine and the metacarpophalangeal joints of the hands.4 Cervical spine involvement is very common, and symptoms do not necessarily accompany extensive bony changes of the spine.5 Rheumatoid involvement of the cervical spine may be present with minimal or no clinical or radiologic expression elsewhere in the body.4 The major clinical problems result from erosive changes in the cervical spine that lead to pathologic subluxation or dislocation.6 Involvement of the thoracic and lumbar regions may also occur, although this is much less common.
The three most common lesions that cause neurologic involvement and/or intractable pain are atlantoaxial subluxation, subaxial subluxation, and vertical subluxation of the odontoid process.7 The onset of cervical spine instability is often insidious. It may be masked by weakness and loss of function associated with peripheral joint disease.8 Although any synovial joint in the spine may be involved, the earliest changes are usually observed in the upper cervical region.3 Rheumatoid involvement of the cervical spine appears to begin early and progresses in relationship to peripheral joint involvement. The cervical spine abnormalities are the result of destruction in the joints, ligaments, and bone by synovitis.2
Atlantoaxial subluxation represents the most common and significant manifestation of rheumatoid involvement of the cervical spine.6 The extent of neurologic deficit does not correlate with the degree of subluxation observed on lateral radiographs. This discrepancy may be the result of the formation of a pannus between the dens and the dura mater. This may contribute to spinal cord compression that cannot be visualized on plain radiographs. In 1830, Sir Charles Bell9 reported the first case of an atlantoaxial subluxation resulting from an inflammatory process. Incompetence of the transverse atlantal ligament was demonstrated pathologically.
The rate of development of neurologic signs and symptoms is usually slow. Numerous large surgical and nonsurgical series of patients with rheumatoid arthritis have demonstrated that the average duration of disease before surgery is 15 to 20 years.7,8,10–15 Although life expectancy in patients with moderate or severe rheumatoid arthritis is less than that of the general population, the presence of a cervical subluxation does not necessarily influence life expectancy.14
The most common clinical finding in rheumatoid involvement of the cervical spine is pain. Typically, this pain is severe and persistent and is usually located in the occipital region4,10,16,17 or the neck,18 or it may radiate toward the vertex of the skull.16 Characteristically, this pain is exacerbated by neck motion.4,5,19 Tears in the transverse atlantal and alar ligaments and in the atlanto-occipital membrane may give rise to retro-orbital or temporal region pains.19 Pain in the arms is usually absent. This type of pain helps distinguish these disorders from cervical spondylosis.20 Neurologic signs and symptoms that are useful for detection of the onset of myelopathy in rheumatoid arthritis patients include neck pain, occipital neuralgia, Lhermitte sign (electric-like shocks produced with neck flexion), and the patient’s account of diminished motor ability or a documented worsening in the motor examination from the previous neurologic examination.21
Myelopathy may develop as a result of spinal cord compression. This usually occurs in late middle age, following many years of disability.21 Because of the frequent, severe deforming effects of rheumatoid arthritis in the extremities, the development of long tract signs is useful in detecting myelopathy. These include hyperreflexia and extensor plantar responses.12,17 Additional signs of myelopathy such as spasticity, presence of a Hoffman sign, and ankle clonus may also be detected. The myelopathy that occurs in rheumatoid arthritis is most likely caused by the effects of compression, stretch, and movement, not by ischemia.22
Because of patient selection and referral patterns, there is a marked discrepancy between the incidence of neurologic involvement of rheumatoid disease of the cervical spine in surgical and nonsurgical series. In two large nonsurgical series of more than 2000 patients with rheumatoid arthritis, reported by Smith et al. and Nakano et al., the incidence of cervical myelopathy was less than 3% in each series.12,14 Interosseous erosive disease of the peripheral joints has been correlated to the severity of involvement of the cervical spine.18,24
The executive committee of the American Rheumatism Association established criteria for rheumatoid arthritis that must be applied only to patients with a clear-cut diagnosis. In addition, this committee has adopted a classification of functional capacity that is used in rheumatologic studies.25
Ranawat et al. developed a classification based on signs and symptoms.7 In this surgical series, neurologic deficits were divided into three classes: I, no neurologic deficits; II, subjective weakness, hyperreflexia, and dysesthesias; and III, objective weakness and long tract signs (A, ambulatory, and B, quadriparetic, not ambulatory).
Vertebral artery compression leading to vertebrobasilar insufficiency may occur in rheumatoid arthritis. The most common potential sites for mechanical compression of the vertebral artery include the foramen transversarium, the atlantoaxial joint, and the occipitoatlantal joint. Vertebral artery insufficiency may be the result of kinking of the vertebral artery at one of these locations or the involvement of the brainstem by upward migration of the dens.24 Symptoms that have been attributed to vertebral artery insufficiency secondary to rheumatoid disease of the cervical spine include dizziness, tinnitus, vertigo, diplopia, suboccipital headache, dysphasia, blurring of vision, cortical blindness, nystagmus, transient blackout spells, confusion, and dysarthria.17,24–26 The frequency with which vertebral artery symptoms may occur is poorly documented. Henderson et al. published nine autopsy cases of severe end-stage rheumatoid arthritis patients with vertical subluxation of the dens that showed the vertebral artery to be patent in all specimens.22
The pathologic changes in rheumatoid arthritis of the cervical spine are predominantly secondary to synovitis. Synovitic proliferation destroys the facet joints, erodes and deforms the dens, and weakens the ligamentous attachments.24 A characteristic pannus may form between the odontoid peg and the ventral dura mater that can compress the spinal cord. This pannus is usually firm, gray-pink tissue that shows end-stage chronic inflammation of synovial tissue.21 In addition to this proliferation of the synovial tissue, osteoporosis and destruction of cartilage and subchondral bone can occur.4,26 Localized bone loss around the inflamed joints is the result of prostaglandin and cytokine synthesis during the inflammatory process, which increases bone resorption.27 Inflammatory destruction of the lateral atlantoaxial joints can lead to vertical translocation of the dens.24 When the odontoid process herniates through the foramen magnum, it can cause flattening, softening, and atrophy of the medulla.28
The specific mechanism by which ischemia causes damage to the spinal cord is unclear. Two separate studies have postulated that intermittent compression of the ventral spinal artery was responsible for the spinal cord injury.1,12 However, in a necropsy study of nine patients, Henderson et al. demonstrated that the histopathologic changes were localized principally to the dorsal white matter of the spinal cord. In this study, the territory of the ventral spinal artery was spared.22 O’Brien et al. performed a histologic study of specimens removed during ventral decompressions of the cervicomedullary junction. They determined that repetitive mechanical damage caused by instability at the atlantoaxial joint, rather than an acute compressive effect from an inflammatory pannus, was the cause of spinal cord compression and subsequent axonal injury.29 In addition, Crockard and Grob have stated that there is no evidence that avascular necrosis or vasculitis is involved in the inflammatory process of rheumatoid arthritis involvement of the spine. They believe that it is the repetitive movement of the unstable atlantoaxial joint against the neuraxis that causes a mechanical “wear-and-tear” phenomenon that leads to the development of a myelopathy.21
In rheumatoid arthritis (due to deficient osteogenesis) osteophytes do not form.1,4,16 This may be contrasted to osteoarthritis that is characterized by the development of osteophytic spurs, which often have a stabilizing effect.1,16,19
Imaging Studies
In a study by Younes et al., 72.5% of patients who met American College of Rheumatology criteria for rheumatoid arthritis had pathology of the cervical spine identified in at least one imaging modality (plain radiographs, MRI, or CT).30
On plain radiographs, small or absent osteophytes, osteoporotic vertebrae, and eroded vertebral end plates characterize rheumatoid arthritis.4 In the absence of rheumatoid arthritis, degenerative changes are more marked in the lower cervical spine with advancing age. Radiographic changes at the C1-2 level are not present unless a specific process, such as rheumatoid arthritis, is affecting this region. These changes are independent of age.30 Bland et al. found 86% of patients with classic or definite rheumatoid arthritis to have evidence of cervical spine involvement on plain radiographs. These changes may frequently be asymptomatic and may not be associated with any neurologic deficit.5 In patients with severe polyarticular rheumatoid arthritis for more than 20 years, Santavirta et al. found radiographic subluxation of the cervical spine in more than 80% of patients.13
The most common radiologic abnormality in rheumatoid arthritis is ventral subluxation of the atlas. The atlantodental interval (ADI) measures the distance between the ventral aspect of the dens and the dorsal ring of the atlas. In normal adult patients, this distance is less than 3 mm.31 An ADI of between 3 and 5 mm in an adult is abnormal and indicates a tear or insufficiency of the transverse atlantal ligament. A separation of greater than 5 mm indicates rupture or attenuation of the alar ligaments in addition to the transverse atlantal ligament.16 Many studies have shown a poor correlation between abnormalities of the ADI and neurologic deficits. In an innovative study, Boden et al. defined the dorsal atlanto-odontoid interval (AOI) as the distance between the dorsal surface of the dens and the ventral edge of the dorsal ring of the atlas measured along the transverse axis of the ring of the atlas. They demonstrated an excellent correlation between the dorsal AOI and the severity of the neurologic deficit. A dorsal AOI of less than 14 mm correlated significantly with the presence and severity of a neurologic deficit. This dorsal AOI was also found to be a good predictor of neurologic recovery postoperatively. These authors stated that the weak correlation of the ventral ADI with a neurologic deficit may be due to variations in the diameter of the atlas as well as the presence of a pannus behind the odontoid process.32 Weissman et al. studied 109 patients with rheumatoid arthritis and atlantoaxial subluxations for 5 years. They found that the ADI increased by more than 2 mm in 41%, remained unchanged in 40%, and decreased in 19% by more than 2 mm. Of the patients whose ADI decreased, more than 50% had developed vertical subluxation of the odontoid process.15 Henderson et al. have stated that vertical subluxation may cause a pseudofixation of the ADI. Interpretation of the ADI must therefore be made in conjunction with measurement of the vertical axial subluxation.22
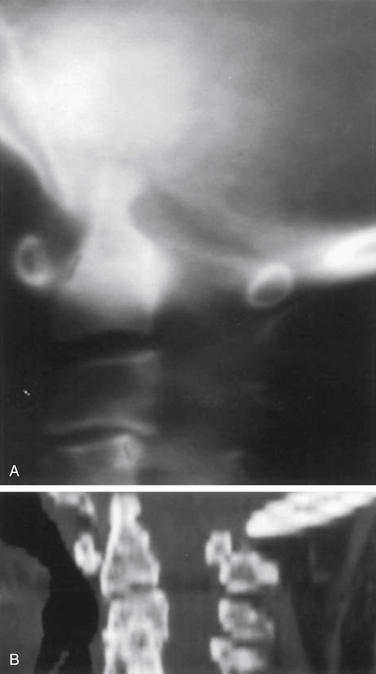
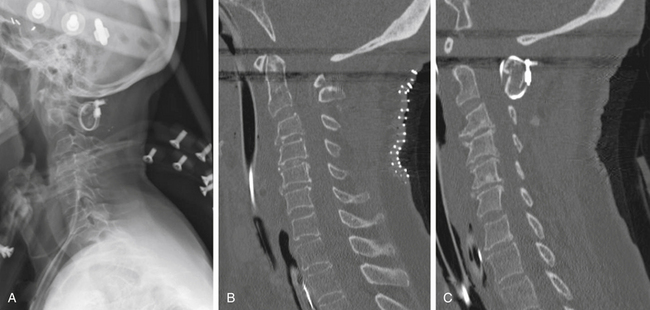
Vertical subluxation of the dens is an upward migration of the dens into the foramen magnum (Fig. 86-1). In this location, the dens competes for space with the spinal cord and the brainstem. Vertical subluxation requires the lateral facet joints to be damaged.12 Vertical subluxation is the second most common upper cervical spine abnormality in rheumatoid arthritis, after atlantoaxial subluxation, and may accompany ventral atlantoaxial subluxation. An increase in the vertical subluxation may actually produce a decrease in the measured ventral atlantoaxial subluxation.15 In vertical subluxation, the presence of a rheumatoid pannus, together with the invaginated dens, may produce ventral compression of the cervicomedullary junction.17
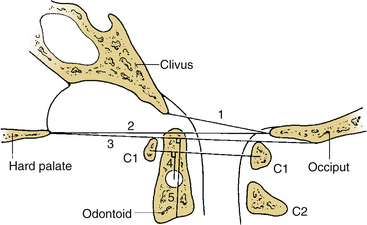
In an attempt to quantify vertical subluxation of the dens, numerous lines and indices have been proposed (Fig. 86-2). These lines are characteristically drawn between bony landmarks that are identifiable on a lateral cervical spine radiograph. The tip of the dens is then measured with respect to the various lines. A McGregor line is drawn from the hard palate to the occiput, and it is probably the most traditional measure.2 A shortcoming of these lines is that the hard palate, the dorsal edge of the foramen magnum, and the tip of the dens are not always visualized on routine lateral cervical spine radiographs in a patient with vertical subluxation of the odontoid. To avoid these difficulties, Ranawat et al. developed an index that measures the distance between the diameter of the ring of the first cervical vertebra to the center of the pedicle of the second cervical vertebra.7 In men and women with normal cervical spines, this distance measured 17 mm in men and 15 mm in women. No normal patients had an interval of less than 15 mm.
A cervical myelogram provides an indirect visualization of the spinal cord and adjacent structures silhouetted by contrast media in the subarachnoid space.33 The information obtained by myelography may be augmented by a postmyelogram CT. Computerized myelotomography, with multiplanar reconstruction, can clearly demonstrate the important contribution of proliferative rheumatoid pannus behind the odontoid peg to ventral cervicomedullary compression. In addition, bone windows on the CT scan can demonstrate bony abnormalities.
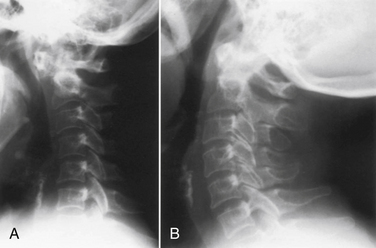
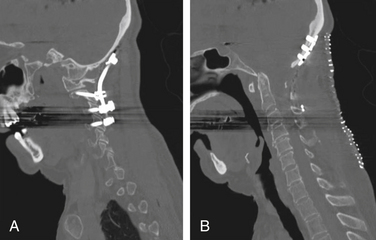
Currently, MRI is considered the ideal study to demonstrate the level and extent of spinal cord compression.33,34 The advantages of MRI include direct imaging of the entire length of the spinal cord and the cervicomedullary junction, direct imaging in multiple planes, superior demonstration of soft tissue structures, and the lack of image degradation by bone artifact at the cervicomedullary junction (Fig. 86-3). In addition, MRI is noninvasive (no intrathecal contrast is needed), can be performed on an outpatient basis, does not expose the patient to the dangers of ionizing radiation, and is generally well tolerated.6,33,35 A limitation of MRI is that it does not image compact bone as accurately as CT.34

Furthermore, Dickman et al. have shown that the transverse atlantal ligament can be consistently and clearly visualized with MRI. This determination of a loss of anatomic continuity of the transverse atlantal ligament is useful for operative planning.36 For patients who are unable to undergo MRI, CT scanning with multiplanar reconstructions provides better information than polytomography. It is important to visualize the neuraxis before surgery; injecting water-soluble contrast into the lumbar subarachnoid space provides additional important anatomic information regarding the flow of cerebrospinal fluid in the upper cervical spine region. Knowledge of the position and course of the spinal vessels, in particular the vertebral arteries, is of extreme importance in many of the surgical approaches to the craniocervical junction. CT angiography provides an excellent means of visualizing the spinal vasculature in relation to the bony anatomy of the upper cervical spine.
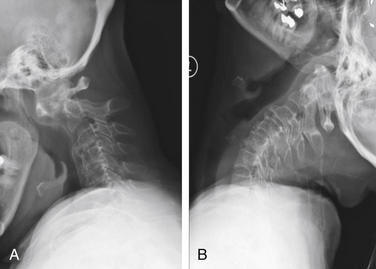
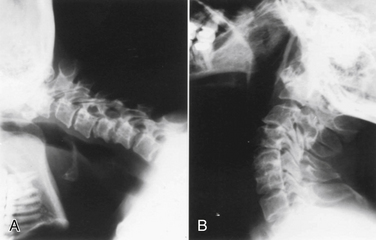
Dynamic views of the cervical spine, in flexion and extension, provide useful information about the degree of instability of the occiput–C1-2 complex (Fig. 86-4). These flexion-extension views can be obtained on plain films, tomograms, computerized myelotomography scans, and MRI studies. Dickman et al. recommend routine lateral cervical radiographs in flexion and extension for all patients undergoing transoral surgery.36 Furthermore, Sharp and Purser recommend lateral flexion and extension radiographs in any patient with severe rheumatoid arthritis undergoing general anesthesia for any surgical procedure.37 Bell and Stearns have found MRI in flexion and extension to be very useful for demonstrating dynamic changes in spinal cord configuration. They have used this information to determine the proximal extent of fusion required and have stated that it provides an accurate and dynamic study of the relationship between the spinal cord and the surrounding bony and soft tissue structures.38 Additionally, upright MRI of the cervical spine can help reveal pathology that may be missed at the craniocervical junction in supine position.39,40
Operative Indications
As a general rule, the presence of myelopathy or a progressive neurologic deficit continues to be a strong indication for surgical intervention in patients with rheumatoid changes of the cervical spine.*
Likewise, intractable pain is an indication for operative intervention.2,3,6,11,18,24,29,32 A much more controversial topic is whether a patient with markedly abnormal radiographs, in the absence of pain or progressive neurologic deficit, should undergo surgery. Numerous authors believe that radiologic evidence of an impending neurologic deficit is an indication for surgery.1,7,41,42 Pellicci et al. believe that radiographic evidence of disease progresses to a greater degree than does neural involvement.18 As such, they believe that no fusion should be recommended on the basis of a radiographic abnormality or radiographic deterioration alone. Others have supported this more conservative viewpoint.2,13,19,28 In an intermediate position, Boden et al. stated that only patients with a neurologic deficit underwent surgery in their series. Nevertheless, they recommended surgery for patients with or without a neurologic deficit, if certain radiographic criteria are met.32
Specific Regions of the Spine
Upper Cervical Spine
To fully understand the complex pathologic changes that occur in the occiput–C1-2 region, a thorough understanding of the biomechanics of this region is necessary. The majority of axial rotation occurs in the upper cervical spine. Approximately 60% of the axial rotation of the entire cervical spine and occiput is found in the upper region (occiput–C1-2) and 40% is found in the subaxial region (below C2). There is no axial rotation between the occiput and C1 unless there has been an occipitoatlantal disruption.44 An extensive amount of axial rotation, 47 degrees, occurs at the C1-2 level.45 White and Panjabi have identified two distinct reasons why this increased motion can occur at the C1-2 level. First, the articular surfaces of the lateral masses of both C1 and C2 have a convex orientation in the sagittal plane that allows for considerable mobility. Second, a taut yellow ligament is not present between the dorsal elements of C1 and C2. Instead, a loose, readily mobile atlantoaxial membrane connects the dorsal elements of C1 and C2, thereby enhancing the motion capacity of this region.45 Craniovertebral junction instability in rheumatoid arthritis patients occurs from a combination of bone softening, ligamentous destruction, and inflammatory pannus formation.46 Unlike the lower cervical spine, the upper cervical spine cannot clearly be divided into ventral and dorsal elements with corresponding mechanical properties.47 White and Panjabi have defined clinical instability as “loss of the capacity of the spine, under physiologic loads, to maintain relationships between vertebrae so that no spinal cord or nerve root damage occurs and no incapacitating deformity or pain develops.”45 This definition has led to certain anatomic measurements from plain film radiographs that can lead to a suspicion of clinical instability. In adults, a ventral ADI of greater than 3 mm on a lateral radiograph is regarded as potentially unstable. Although less widely used, a dorsal AOI of less than 14 mm is also suspicious for clinical instability.28 With this basic understanding of the biomechanical relationships of the upper cervical spine, the two most common abnormalities in this region are ventral atlantoaxial subluxation, caused by incompetent ligaments, and vertical subluxation of the odontoid process that occurs because of lateral mass erosion.
Atlantoaxial Subluxation
Ventral atlantoaxial subluxation is the most common abnormality of the spine in rheumatoid arthritis. Classically, atlantoaxial subluxation is considered present if the ADI is greater than 3 mm in an adult or greater than 4 mm in a child.24 Due to selection biases between surgical and nonsurgical studies of patients with rheumatoid arthritis, there are marked discrepancies in the frequency with which atlantoaxial subluxation occurs. In a large study in the rheumatologic literature on the prevalence of atlantoaxial subluxation in rheumatoid arthritis patients, the authors found that an atlantoaxial subluxation was present in 1 of 30 patients with any evidence of rheumatoid arthritis, in 1 of 15 patients with clinical evidence of the disease, and in 1 of 5 patients with rheumatoid arthritis admitted to the hospital.37 This last group of patients are those more likely to be seen by a spine surgeon. Indeed, in the study by Weissman et al., ventral atlantoaxial subluxation was found to occur in one fourth to one third of rheumatoid arthritis patients.15 Disruption of the transverse ligament of the atlas is the most important pathologic abnormality responsible for atlantoaxial instability.36
The degree of atlantoaxial subluxation is poorly correlated with clinical evidence of a compressive myelopathy.33 Similarly, no correlation between the magnitude of an atlantoaxial subluxation and mortality was found in a 10-year follow-up study.13 In a large radiologic review of 189 rheumatoid arthritis patients with atlantoaxial subluxations, Weissman et al. found the incidence of spinal cord compression to be 11%.15 These findings underscore the necessity of an accurate history and physical examination to determine which patients with atlantoaxial subluxations demonstrate evidence of neurologic abnormalities related to this radiographic abnormality. A characteristic clinical finding of ventral atlantoaxial subluxation is difficulty in raising the head to the neutral position following downward gaze. This sensation of the head “falling forward” has been referred to as the Sharp-Purser sign.37 An extremely rare abnormality is dorsal atlantoaxial subluxation. For a dorsal atlantoaxial subluxation to occur, the dens must be destroyed, fractured, or congenitally absent; alternatively, the ventral arch of the atlas must be destroyed or congenitally absent.15,31,48,49
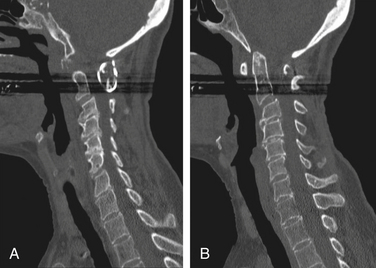
Vertical subluxation of the dens can occur simultaneously with a ventral atlantoaxial subluxation. When this occurs, the ADI can appear to actually decrease in size.50 Isolated ventral subluxation is more common than either vertical subluxation or a combination of ventral subluxation and vertical subluxation. Kraus et al. studied 55 patients with atlantoaxial subluxations who received dorsal fusion and found that none developed subsequent vertical subluxations. They believed that the dorsal fusion operation may have a protective effect in preventing vertical subluxation.11 This protective effect of dorsal fusion has not been demonstrated in a prospective study. Contrary to the findings of Kraus et al.,11 we present the case of a patient with rheumatoid arthritis that initially presented with atlantoaxial subluxation that was treated with a Brooks-type fusion. The patient subsequently developed vertical subluxation 6 months after the operation despite fusion at C1-2, which was treated with occipitocervical fusion (see Figs. 86-8 to 86-11).
Vertical Subluxation of the Odontoid
Vertical subluxation of the dens is referred to by a variety of terms, including atlantoaxial impaction, cranial settling, upward migration of the odontoid, pseudobasilar invagination, translocation of the dens, superior migration of the odontoid, basilar invagination, and vertical settling. These terms have been used interchangeably in the medical literature. Vertical subluxation occurs as a consequence of loss of substance of the lateral masses, usually the atlas. However, the lateral masses of the axis and, less commonly, the occipital condyles may also be involved.22 In vertical subluxation, the ventral arch of C1 gradually articulates with caudal portions of C2, first via the base of the dens and then with the body of C2.15 If there is more than 18 mm of translocation, the ring of the atlas is usually broken and the base of the axis has migrated within the disrupted ring. Significant vertical subluxation of the dens is generally agreed to be an indication for a fusion operation.7,13,15–17,28,42
Neurologic abnormalities are far more common with vertical subluxation of the dens than with atlantoaxial subluxation. The abnormal neurologic symptoms are the result of compression of the brainstem or upper cervical spinal cord. Neurologic abnormalities detected in vertical subluxation of the dens include hyperreflexia, extensor plantar reflexes, limb paresthesias, progressive difficulty with ambulation, a central cordlike syndrome, neurogenic bladder, and lower cranial nerve palsies.17 Rheumatoid arthritis patients with vertical subluxation are more likely to be symptomatic from spinal cord compression.13,15,17,28,51
Lower Cervical Spine
As with abnormalities of the upper cervical spine, the presence of subaxial subluxations of the lower cervical spine varies greatly in reported series. Subaxial subluxation is a gradual process in which there is a forward displacement of one or more vertebral bodies on the vertebral body immediately below (Fig. 86-5). The rheumatoid process attacks the zygapophyseal facet and uncovertebral joints, weakens the supporting ligaments, and erodes the intervertebral discs. These effects loosen the various intervertebral fixations and permit luxation between adjacent vertebral bodies.1 Subaxial subluxations are usually reducible by traction; however, the reduction is difficult to maintain.29 Classically, subaxial subluxation is a translation of one vertebra in relation to an adjacent vertebra of greater than 3.5 mm on a lateral cervical spine radiograph.31 Boden et al. found that the diameter of the subaxial sagittal spinal canal reflected the presence and degree of a neurologic deficit, more often than did the percentage of vertebral body slip.32 In addition to the bony luxations, compression from epidural rheumatoid granulations has been reported.2–4
Subaxial subluxations are usually late developments in the aggressive forms of rheumatoid arthritis.4,13 The severity of these subaxial subluxations is also closely related to the duration of rheumatoid disease.4,14 When compared with patients with atlantoaxial subluxations, the incidence of neurologic deficits is higher in patients with subaxial subluxation, and the final results are poorer.8
Typically, subaxial subluxations show a “staircase” appearance with multiple subluxations observed sequentially in the cervical spine.2,6,12 Subaxial subluxations may result in nerve root impingement from foraminal narrowing.6 The presence of a subaxial subluxation should be suspected when bizarre weakness of the hands is observed in a patient with rheumatoid arthritis. This may be difficult in patients with long-standing disease who already have crippling deformity of the hands.52 This subaxial spinal cord involvement may cause myelopathy and may explain why some patients do not respond to surgical decompression at the craniocervical junction.22 The most common site for subaxial subluxation is at the C3-4 level; however, it often occurs at multiple levels, and these typically lack osteophytes.2,3,53
Subaxial subluxations may be present at the time of surgery for an upper cervical instability. The caudal extent of the instrumentation and fusion must therefore be carefully selected to incorporate any segments with a significant subaxial subluxation.54,55 In an autopsy study of nine patients with severe end-stage rheumatoid arthritis, Henderson et al. found subaxial compression present in eight of the nine patients.22 More commonly, subaxial subluxations may occur after fusion operations in the upper cervical spine.3,6,11,53 As a result, it is essential that patients who undergo upper cervical fusions be followed closely with lateral cervical spine radiographs both for evidence of an acceptable bony fusion and for the development of subaxial subluxations. Kraus et al. found a much higher incidence of subaxial subluxations in patients whose upper cervical fusion incorporated the occiput. They postulated that this was because of a longer lever arm that results in higher forces generated at the lower cervical levels and that leads to a subaxial subluxation.11 Subaxial cervical subluxations in rheumatoid arthritis patients have been associated with quadriplegia, sudden death, and other neurologic complications resulting from damage of the spinal cord or from interference with the flow of the vertebral arteries.56
The most accurate radiographic imaging study currently available to detect the site and type of spinal cord compression in subaxial subluxation of the rheumatoid spine is MRI.13 All patients with subaxial subluxations and atlantoaxial subluxations with neurologic deficits or vertical subluxations of the dens should have an MRI study, if possible.8 In patients who cannot undergo an MRI, a myelogram followed by a postmyelogram CT scan should be obtained.
Thoracic and Lumbar Spines
Involvement of the thoracic and lumbar spines in rheumatoid arthritis patients is rare. Heywood and Meyers have stated that subcervical rheumatoid spondylitis is more common than is generally believed and have found an incidence of 0.9% in their clinic.57 Most other series of rheumatoid arthritis patients do not even address the topic of the thoracic and lumbar spines. In a study by Redlund-Johnell and Larsson, of 100 patients with severe rheumatoid arthritis who had previously undergone occipitocervical fusion, four patients with subluxation of the upper thoracic spine were found. These changes in the upper thoracic spine were radiologically similar to the destructive type of subaxial subluxation typically observed in the cervical spine. The authors believed that this upper thoracic subluxation may have been caused by increased motion as compensation for decreased mobility in the cervical spine.58 The pathogenesis of rheumatoid spondylitis in the thoracic and lumbar spines is believed to be the result of a facet joint synovitis that leads to instability. In addition, involved costovertebral joints can spread their involvement to the disc space, causing a discitis between the disc and the vertebral end plates that can lead to further instability.57 Rheumatoid granulation tissue causing compression of the thoracic spine has been reported.59,60 In addition, an extensive inflammatory synovitis of the costovertebral and costotransverse joints can occur in the thorax.61
Rheumatoid involvement of the lumbar spine is rarely recognized as a cause of nerve root or cauda equina compression. Intraspinal rheumatoid granulomatous nodules can lead to nerve root compression, causing back and leg pain.59,62 In addition, rheumatoid granulation tissue can develop in the lumbar facet joints and spread to the periarticular structures to contribute to cauda equina compression.63,64
The plain radiographic features of subcervical rheumatoid spondylitis include an ill-defined, blurred, and eroded margin to the vertebral end plates and an ill-defined, eroded facet joint complex.57 If not specifically sought, these radiographic abnormalities may be easily overlooked. Frequently, rheumatoid arthritis patients have stiff, high-positioned shoulders that may conceal the cervicothoracic junction on conventional radiographs. If clinically indicated, an MRI study allows for better visualization of the cervicothoracic junction and the remainder of the thoracic and lumbar spines.58
Related posts:
 Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


